Introduction
Dentistry and sports merge in the exciting practice of sports dentistry. According to the International Academy for Sports Dentistry, the main goals of sports dentistry include prevention and treatment of sports related dental/orofacial injuries, information collection, information dissemination and promotion of research on the preventive procedures related to injuries of such a specific aetiology [1].
It combines skills to both protect the athlete from orofacial injures and treats them. Prevention is certainly a hallmark of dentistry. The National youth sports foundation for the prevention of Athletic injuries has reported that dental/orofacial injuries are the most common type sustained during participation in sports. These include soft-tissue lacerations, abrasions and contusions, tooth intrusions, or avulsions, crown or/and root fracture [Table/Fig-1], loss of one or several teeth most frequently loss of maxillary incisors [Table/Fig-2]. The less frequent trauma includes fractures of the zygoma, mandibular fractures, alveolar fractures and traumatic injuries to the temporomandibular joint [2]. Temporomandibular injuries and disorders in sport can be caused by direct blows to the temporomandibular region and indirectly by blows into the chin or laterally into the lower jaw wherein the force is transferred into one or both jaws. At the same time, the pathogenic effect of the force can be dissipated and modified by surrounding muscles, articular and extra-articular ligaments, articular disc and capsule, teeth. It should be stressed that a pair of joints plays a significant role in this type of trauma. Macro traumas are the cause of jaw fractures, condylar fractures and dislocations, cranial base fractures, brain concussions, injuries and displacements of the articular disc, intra-capsular haemorrhages and edematous changes. Micro traumas can cause tendinitis, synovitis, capsulitis, osseous or fibrous ankylosis, articular disc displacement, subluxation and condylar dislocation [1,3]. There is a wide range of symptoms including: limited mouth opening, deviations of the lower jaw on mouth opening towards the injured side, malocclusions, noise in the joint, sensation of pain in the joint, muscles and surrounding tissues, inhibited mouth closing (open bite) bilaterally or contra laterally in cases of condylar process fractures and bilaterally and ipsilaterally in cases of articular luxations [4]. The prevalence of orofacial injuries varies depending on the type of sport played, the degree of contact, and the age, gender and geographical location of the subject studied [2]. Orofacial injuries have widespread and problematic implications. Such injuries may impact physical, psychological, social, and economic aspects of life. Physically, orofacial injuries can result in abnormal primary teeth exfoliation, failure in permanent teeth eruption, unfavourable colour changes in teeth, [Table/Fig-3] development of painful abscesses, [Table/Fig-4] and tooth loss resulting in unaesthetic gaps in the mouth of the injured victim [5].


Nonvital discolored tooth


Protection from sport-related orofacial injuries currently comes in the form of three shielding equipments: mouth guards, facemasks, and helmets. This review focuses on the role of intra-oral mouth guards in preventing sports-related orofacial injuries. During the 1960s and 1970s, the use of mouth guards was made mandatory in many sports, including football, ice hockey, lacrosse, field hockey, boxing, martial arts, racquetball, roller hockey, rugby, shot putting, skateboarding, skydiving, soccer, squash, volley ball, water polo, wrestling and wasting.
The rationale for these rule changes was to provide additional protection against dental and orofacial injuries and to reduce a player’s risk of concussion [6]. American Dental Association has estimated that face guards and mouth guards prevent approximately 200,000 injuries each year in high school and college football alon [7]. Sports mouth guard range from ill-fitting stock guards to mouth formed guards to custom guards made on cast. Learning to fabricate laminated mouth guards specialized to individual athletes or sports is a valuable skill.
We as dentists need to understand the need for initiatives, education and development of a program to encourage the consistent use. Attitudinal factors are just as important in mouth guard success as is good mouth guard design.
What is a Mouth Guard?
The word mouth guard is universal and generic and includes a large range of products bought at the sporting good stores to professionally manufactured custom made by a dentist. The mouth guard, also referred to as a gum shield or mouth protector, is defined as a “resilient device or appliance placed inside the mouth to reduce oral injuries, particularly to teeth and surrounding structures [8].” For optimal safety and well-being of athletes competing in the 21st century, the Academy of sports dentistry has adopted the position that the single word “Mouth guard” must be placed by the term a “property fitted mouth guard.” According to the placement, mouth guards can be extra-oral, intra-oral and combined. The extra-oral mouth guard is attached to the helmet in the form of a protective net or grating. The intra-oral mouth guard is placed on the dental arch. There are monomaxillary and bimaxillary mouth guards. The monomaxillary mouth guard has retention on one dental arch. The bimaxillary mouth guard, due to its construction, has retention on both dental arches thus ensuring normal breathing [9].
Preventive and Protective Role of Intra-oral Mouth Guard
Dental/Orofacial Trauma Prevention
Mouth guard is meant to act as a buffer by moving the soft tissues in the oral cavity away from the teeth preventing lacerations, bruising of lips, cheeks, and tongue during an impact. It is supposed to prevent tooth fractures or dislocations by cushioning the teeth from direct frontal blows while redistributing the force of the blow over all the teeth. Opposing teeth are protected from seismic contact with each other. Mandible is afforded elastic, recuperative support can prevent fracture or damage to the unsupported angle of the lower jaw [1,10]. Their use can also provide substantial protection to patients receiving orthodontic treatment. It is also identified that mouth guards should be worn on the maxillary teeth, as it was evident that the maxillary anterior teeth were most prone to injury except in class III malocclusion because in such a case, the mouthguard should be worn on the mandibular teeth [11].
Concussion Prevention
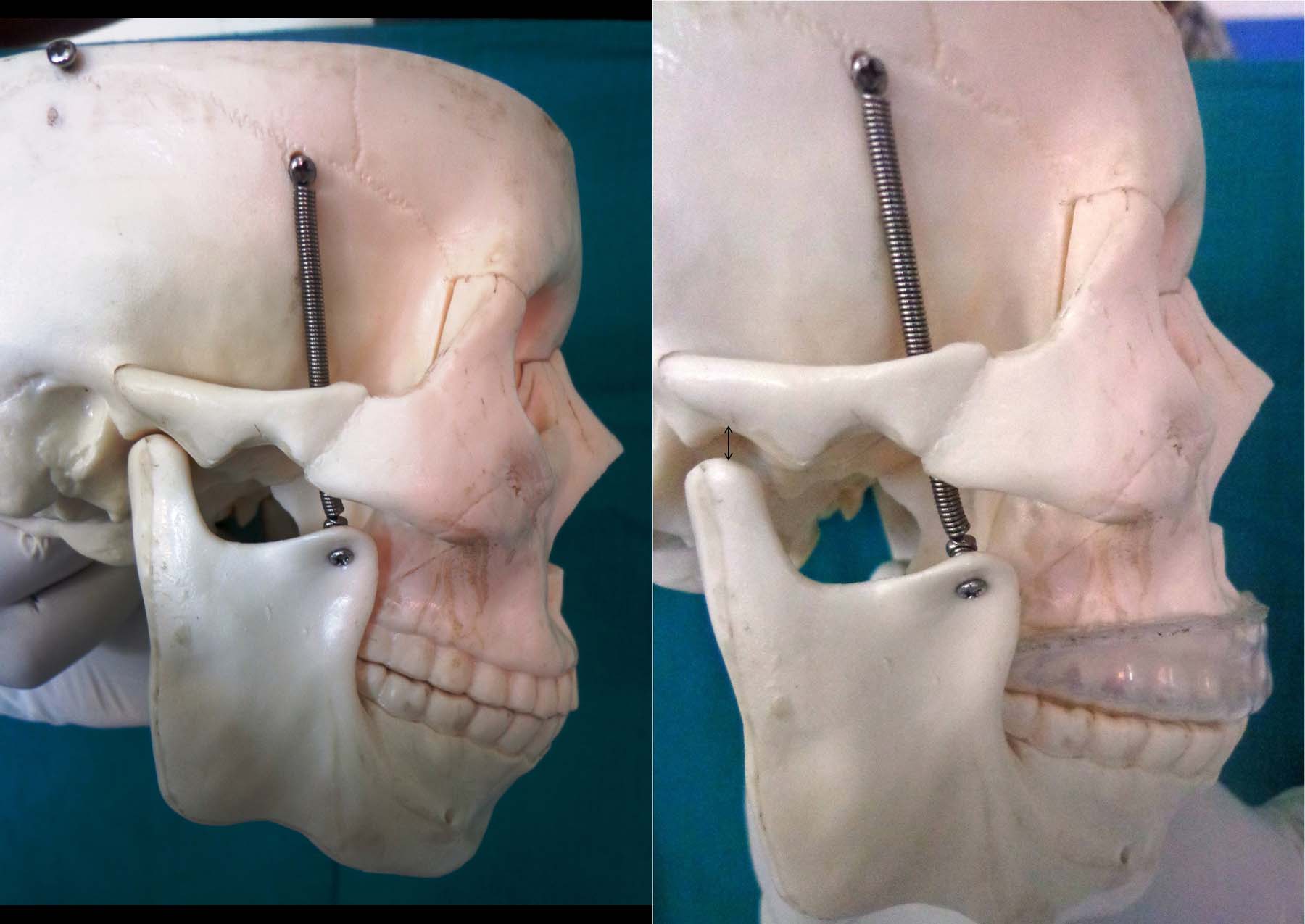
Many authors have claimed that mouth guards offer an effective means of preventing concussion and spinal injuries [12–13]. Stenger et al., [14] claimed a benefit for both head and cervical spinal injuries by mouth guard use. They concluded that a mouth guard in situ, there was an altered mandibular position on lateral skull radiographs, so that the condyles were distracted from their fossae [Table/Fig-5]. The bulk of the evidence indicating a potential protective effect of mouth guards on concussion incidence has been based on limited case series studies and retrospective, nonrandomized cross-sectional surveys [15]. There is also evidence that mouth guard use does not result in any difference in neurocognitive test performance after concussion [16].
Distance between head of the condyle from base of the skull without and with intra-oral mouth guard in place
Neuromuscular Relaxation
Muscles in the face, jaw, and neck are some of the most used muscles in the body. Because of constant use and a high propensity for stress to affect these muscles, most people experience tension, nerve pinching, and even a buildup of toxins in these areas. However, with neuromuscular treatment, all of these problems are addressed and corrected by releasing tension and aligning the jaw. Nevertheless, to get muscles in relaxed and proper position is often difficult as our bodies naturally form their own tension spots and misalignments. Part of neuromuscular treatment is to relax the muscles of the neck and face, which has a ripple effect on the muscles throughout the body, which can be, provide with a properly fitting mouth guard.
Furthermore, the body can easily become misaligned. In fact, misalignments in the hips, shoulders, and other areas of the body can be effected by neuromuscular problems in the jaw and neck.
Effect of Mouth Guards on Performance
The effects of performance oral appliances are related to neurophysiologic feedback mechanisms; the release of cortisol – the so-called stress hormone – and lactate levels have been found to play a role. It has also been found that non-functional biting (such as with an oral appliance) can impede this feedback mechanism [17]. It is further hypothesized that by repositioning the mandible, the patency of nerves and arteries in the TMJ is improved, increasing blood flow and the perfusion of oxygen to the tissues, which in turn may improve function and strength [18].
Some research suggested that mouthpieces might enhance performance. The professional football players exhibited greater arm strength with properly fitted mouth guards that resulted in changes in bite patterns [19]. More recently, research has suggested mandibular position and oral appliances positively affect not only upper-body strength, but also endurance, recovery after athletic competition, concentration, and stress response [20].
Psychological Effect
Psychologically, the athletes feel more confident. Provide the athlete with the confidence that they are less likely to sustain injuries, thus giving them the competitive edge for aggressive competition.
Classification of Mouth Guard [21]
ASTM (American society of testing and Materials) reapproved the classification for athletic mouth guards as follows.
Type I - Stock Mouth guards. (Least preferred)
Type II - Mouth formed mouth guards.
Type III - Custom fabricated (over a dental cast) mouth guards (Most preferred).
Stock Mouth Guards
Ready to wear prefabricated, available at most sporting good stores, come in limited sizes, has lowest-cost option [Table/Fig-6]. As they cannot be prepared to mimic the mouth, they fit poorly and are bulky [22]. They are designed for use without any modification and must be held in place by clenching the teeth together to provide a protective benefit [8]. Clenching a stock mouthguard in place can interfere with breathing and speaking and, for this reason, stock mouthguards are considered by many to be less protective [8]. Unfortunately, these are still the most commonly used on the market of many developing countries. Tooth arrangement & arch sizes varies too much between people. There is too much variability among dentitions for the mass production of effective mouth guards.
Bimaxillary stock mouth guard

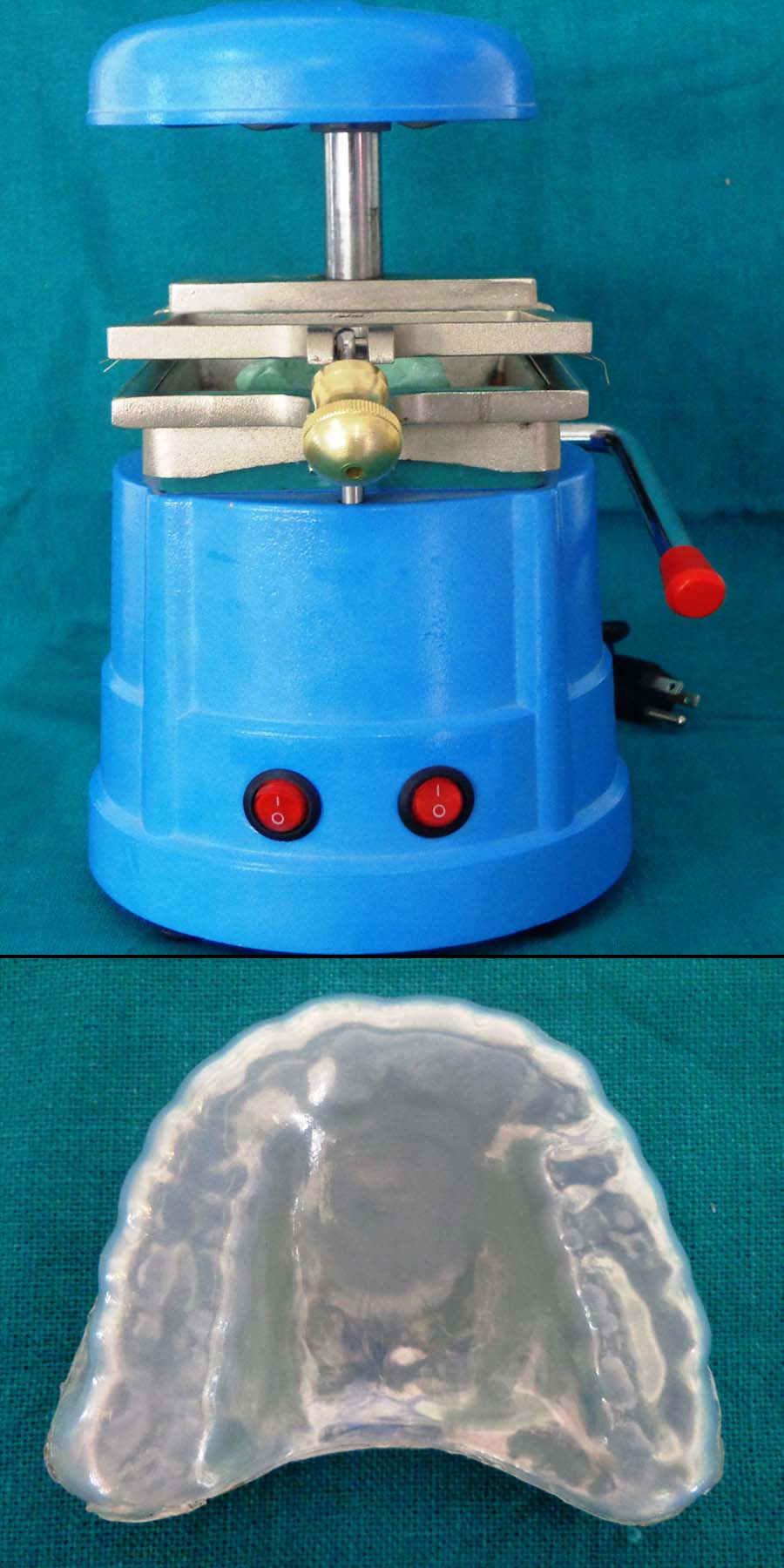
Custom mouth guard fabricated in Vacuum formed machine
Mouth Formed Mouth Guards
Mouth-formed, also known as “boil-and-bite”, mouthguards are made from a thermoplastic material adapted to the mouth by finger, tongue, and biting pressure after immersing the appliance in hot water [8]. Available commercially at department and sporting-goods stores, these are the most commonly used among athletes but vary greatly in protection, retention, comfort, and cost. Woodansey [23] added that because they are formed at body temperature, they readily distort and wear off. They often lack proper thickness and extension leading to lesser protection and retention.
Custom Made Mouth Guards
They are more expensive, most comfortable, best-fitting custom-designed mouth guards recommended by the dentist [24]. Varieties of materials are currently being used for mouth guards, most commonly polyvinyl-acetate-polyethylene copolymer and polyvinyl chloride. Silicone rubber, natural rubber, soft acrylic resin, and polyurethane are less widely used. Patrick and van Noort ranked the effectiveness of protective mouth guards, finding the laminated mouth guards with outer hard layers and an inner soft layer the most effective and stock mouth guards the least effective [25]. There is some scientific rationale that custom-fit mouth guards might be more effective at measurably absorbing the force of impact [26]. This type is fabricated on a cast of athletes (Max arch for patients with CL I or CL II Malocclusion, Mandibular arch with CL III Malocclusion) Before fabricating a thorough Medical and dental history, including, intra oral extra-oral and necessary radiographic examination is conducted. The professionally-fitted custom-made mouth guard is widely seen to give the dentist the critical capability to address several important issues in the fitting of the mouth guard, such as the appropriateness of the design for the sport being played, any history of previous dental injury or concussion, additional protection in any specific area, etc. which cannot be addressed by stock and the boil-and-bite mouth guard [27]. Their fabrication technology employs vacuum technique or pressure technique as well as thermal, polymerization (conventional or injection) and light-curing procedure and their combinations, depending on the material, type of sporting activity and individual characteristics of the jaw [4]. Theoretically, a properly fitted mouthguard should be protective, comfortable, resilient, tear-resistant, odorless, tasteless, inexpensive, easy to fabricate and should not interfere with speech or breathing [11]. Protective thickness is important because as the thickness of the material increases logarithmically, the transmitted impact force decreases logarithmically.
Professional Responsibility as a Dentist
Players’ perceptions of mouthguard use and comfort largely determine their compliance and enthusiasm. Therefore, the dental profession needs to influence and educate all stakeholders about the risk of sports-related orofacial injuries and available preventive strategies [23,25]. Routine dental visits can be an opportunity to initiate patient/parent education and make appropriate recommendations for use of a properly-fitted athletic mouthguard [1]. Dental professionals need to develop effective ways of conducting research to determine the prevalence of sports-related injuries in their communities. Sports dentistry should encompass much more than mouth guard fabrication and the treatment of fractured teeth. As dental professionals, a responsibility exists to become and remain educated and pass that education on to the community regarding the issues related to sports dentistry and specifically to the prevention of sports-related oral and maxillofacial trauma [28]. For optimal preventive techniques, it is recommended that sports dentistry should be included in dental curriculum at both undergraduate and postgraduate levels.
Suggestions for Increasing the Use of Mouth Guards
Attitudes of officials, coaches, parents, and players about wearing mouth guards influence their usage. Although coaches are perceived as the individuals with the greatest impact on whether or not players wear mouth guards, parents view themselves as equally responsible for maintaining mouth guard use [29,30]. However, surveys of parents regarding the indications for mouth guard usage reveal a lack of complete understanding of the benefits of mouth guard use [29]. Qualified athletes should serve as role models for young athletes performing public service announcements promoting the use of properly fitting mouth guards. Professional athletes team physicians, trainers and team dentists should be advocators for the use of sports mouth guards.
Future Research
Research in sports dentistry is challenging. The most evidence-based information comes from statistics in traumatology and epidemiology. Studies of injury type, age and sport studies are underway to suggest new mouth guard designs.
Conclusion
Prevention is an obligation of dentistry as well as critical patient responsibility. Safe sport participation should be the goal of any sport program. A mouth guard should be part of every athletes gear. No matter what accidents happen. It takes very little force to cause a lot of damage to a mouth so play smartly, protect your smile, and wear a mouth guard.
[1]. Ranalli DN, Sports dentistry and dental traumatologyDent Traumatol 2002 18(5):231-36. [Google Scholar]
[2]. Kumamoto DV, Maeda Y, A literature review of sports-related orofacial traumaGen Dent 2004 52(3):270-80. [Google Scholar]
[3]. Kvittem B, Hardie NA, Roettger M, Conry J, Incidence of orofacial injuries in high school sportsJ Pub Health Dent 1998 58(4):288-93. [Google Scholar]
[4]. Knapik JJ, Marshall SW, Lee RB, Darakjy SS, Jones SB, Mitchener TA, Dela Cruz GG, Jones BH, Mouthguards in sport activities: history, physical properties and injury prevention effectivenessSports Med 2007 37(2):117-44. [Google Scholar]
[5]. Torg JS, Athletic injuries to the head, neck, and face 1991 2nd edSt. LouisMosby [Google Scholar]
[6]. Mellion MB, Team physician’s handbook 2002 3rd edPhiladelphiaHanley & Belfus [Google Scholar]
[7]. Jerolimov V, Temporomandibular injuries and disorders in sport. Rad 507Medical Sciences 2010 34:149-65. [Google Scholar]
[8]. CDHACDHA Position paper on sports mouthguardsCanadian Journal of Dental Hygiene (CJDH) 2005 39(6):1-18. [Google Scholar]
[9]. ADA Council on Access, Prevention and Interprofessional Relations; ADA Council on Scientific AffairsUsing mouthguards to reduce the incidence and severity of sports-related oral injuriesJ Am Dent Assoc 2006 137(12):1712-20. [Google Scholar]
[10]. Heintz W, The case for mandatory mouth protectorsPhys Sportsmed 1975 3:61-3. [Google Scholar]
[11]. Powers JM, Godwin WC, Heintz WD, Mouth protectors and sports team dentists. Bureau of Health Education and Audiovisual Services, Council on Dental Materials, Instruments, and EquipmentJ Am Dent Assoc 1984 109:84-7. [Google Scholar]
[12]. Newsome PR, Tran DC, Cooke MS, The role of the mouthguard in the prevention of sports-related dental injuries: a reviewInt J Paediatr Dent 2001 11(6):396-404. [Google Scholar]
[13]. Badel T, Jerolimov V, Panduric J, Dental/orofacial trauma in contact sports and intra-oral mouthguard programmesKinesiology 2007 39(1):97-105. [Google Scholar]
[14]. Stenger JM, Lawson EA, Wright JM, Ricketts J, MouthGuards: Protection against Shock To Head, Neck and TeethJ Am Dent Assoc 1964 69:273-81. [Google Scholar]
[15]. Reed RV Jr, Origin and early history of the dental mouthpieceBr Dent J 1994 176(12):478-80. [Google Scholar]
[16]. Scott J, Burke FJ, Watts DC, A review of dental injuries and the use of mouthguards in contact team sportsBr Dent J 1994 176(8):310-14. [Google Scholar]
[17]. Chapman P, Mouthguards in sportSports Health 1983 1:13-15. [Google Scholar]
[18]. Chapman P, Concussion in contact sports and importance of mouthguards in protectionAust J Sci Med Sport 1985 3:170-4. [Google Scholar]
[19]. Chapman PJ, Mouthguards and the role of sporting team dentistsAust Dent J 1989 34:36-43. [Google Scholar]
[20]. Ferrari CH, Ferreria de Mederios JM, Dental trauma and level of information: mouthguard use in different contact sportsDent Traumatol 2002 18(3):144-47. [Google Scholar]
[21]. Benson BW, Hamilton GM, Meeuwisse WH, McCrory P, Dvorak J, Is protective equipment useful in preventing concussion? A systematic review of the literatureBr J Sports Med 2009 43(Suppl 1):i56-67. [Google Scholar]
[22]. Mihalik JP, McCaffrey MA, Rivera EM, Pardini JE, Guskiewicz KM, Effectiveness of mouthguards in reducing neurocognitive deficits following sports-related cerebral concussionDent Traumatol 2007 23(1):14-20. [Google Scholar]
[23]. Hori N, Yuyam N, Tamura K, Biting suppresses stress-induced expression of corticotrophin-releasing-factor (CRF) in the rat hypothalamusJ Dent Res 2004 83(2):124-8. [Google Scholar]
[24]. Fuchs CZ, The Effect of the Temporomandibular Joint Position on Isometric Muscle Strength and Power in Adult Females [dissertation] 1981 Boston, MABoston University [Google Scholar]
[25]. Gelb H, Patient evaluation. Clinical Management of Head, Neck, and TMJ Pain and Dysfunction: A Multidisciplinary Approach to Diagnosis and Treatment 1977 Philadelphia, PAWB Saunders Co:73-116. [Google Scholar]
[26]. Smith S, Muscular strength correlated to jaw posture and the temporomandibular jointN Y State Dent J 1978 44(7):278-85. [Google Scholar]
[27]. Smith SD, Adjusting mouthguards kinesiologically in professional football playersN Y State Dent J 1982 48(5):298-301. [Google Scholar]
[28]. Garabee WF, Craniomandibular orthopedics and athletic performance in the long distance runner: a three-year studyBasal Facts 1981 4(3):77-81. [Google Scholar]
[29]. Francis KT, Brasher J, Physiological effects of wearing mouthguardsBr J Sports Med 1991 25(4):227-31. [Google Scholar]
[30]. Tiep BL, Pursed lips breathing—easing does itJ Cardiopulm Rehabil Prev 2007 27(4):245-46. [Google Scholar]