Anterior Maxillary Intrusion and Retraction with Corticotomy-Facilitated Orthodontic Treatment and Burstone Three Piece Intrusive Arch
Ramachandra Prabhakar1, M.K Karthikeyan2, R. Saravanan3, K.S. Kannan4, M.R. Arun Raj5
1Dean & HOD, Department of Orthodontics, THAI Moogambigai Dental College & Hospital, Chennai, India.
2 Professor, Department of Orthodontics, THAI Moogambigai Dental College & Hospital, Chennai, India.
3 Professor, Department of Orthodontics, THAI Moogambigai Dental College & Hospital, Chennai, India.
4 Professor and HOD, Department of Pedodontics,Professor and HOD, Department of Pedodontics, THAI Moogambigai Dental College & Hospital, Chennai, India.
5Department of Orthodontics, THAI Moogambigai Dental College & Hospital, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR:Dr. Ramachandra Prabhakar,Dean and HOD, Department of Orthodontics, Thai Moogambigai Dental College And Hospital, Chennai, India.
Phone: 9444468399,
E-mail: dr.ramachandra.prabhakar@gmail.com
An adult patient with proclination and spacing was performed orthodontic treatment combined with corticotomy and the burstone three piece intrusive arch who desired a shortened treatment period. The patient had Angle’s Class I malocclusion with flaring of the maxillary and mandibular incisors. Pre adjusted edgewise appliance (MBT prescription) was fixed to the maxillary and mandibular teeth. Then corticotomy was performed on the cortical bone of the buccal sides in the maxillary anterior regions. Intrusion and retraction initiated immediately after the corticotomy. The intrusive arch was adjusted once in every 2 weeks. The total treatment time for intrusion was 5 months. Cephalometric superimpositions showed no anchorage loss, and panoramic radiographs showed neither significant reduction in the crestal bone height nor marked apical root resorption. A corticotomy-facilitated orthodontic treatment shortened treatment period without any anchorage loss or adverse effects.
Introduction
Adult patients who seek orthodontic treatment often desire that their treatment should be completed in a short period [1]. One possible method for completing treatment in a shorter period is through an orthodontic treatment combined with corticotomy [2].Orthodontic treatment usually lasts one to two years, and even more time is required for extraction cases. To shorten the time for orthodontic tooth movement, various attempts have been made. These attempts fall into three categories. The first is local or systemic administration of medicines [3–6]. The second category is mechanical or physical stimulation such as direct electrical current or a samarium-cobalt magnet. The last category is oral surgery, including dental distraction [7], alveolar surgeries to undermine interseptal bone [8], and alveolar corticotomies, which have been used to correct malocclusions for over 100 years [9]. Corticotomy is effective and safe to accelerate orthodontic tooth movement. It was performed by making small perforations on the alveolar bones along the way by which the tooth would be moved [10]. Corticotomy facilitated orthodontics enables the limitation of the undesirable adverse effects of the orthodontic therapy, such as root resorption and periodontal damage [11].
Case Report
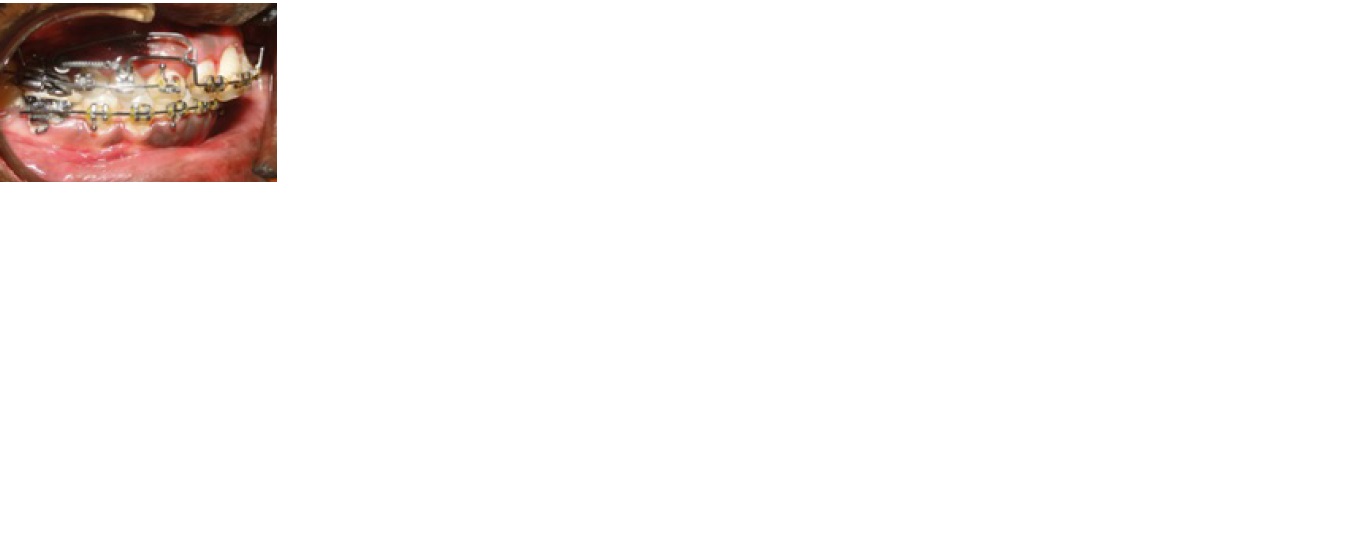
A 28–year–old male patient had a chief complaint of proclination and spacing of upper and lower incisors [Table/Fig-1,2]. He was diagnosed with Angle’s class I malocclusion with anterior spacing. Treatment plan was to intrude and retract the upper anteriors. Thick cortical bone was present in the anterior region. There was a need to finish the treatment early. So the decisionwas made to perform periodontally accelerated osteogenic orthodontics (PAOO) in this patient. The patient had no relevant medical history and the patient’s consent was taken before the treatment.
Surgical Procedures
A modified corticotomy procedures was carried out by local anesthesia. A mucoperiosteal flap was elevated labially beyond the apex of the upper incisors [12]. The vertical cuts were performed from the distal of the right upper lateral incisor to the distal of the left upper lateral incisor and the cortical bone was removed by tungsten carbide bur (245) with continuous saline irrigation. This incision preserves the interdental papilla on the buccal sides of the maxillary anteriors [Table/Fig-3] and no flap elevation or corticotomy was performed on the lingual or the palatal side in this case. Care was taken not to damage neurovascular bundles.
Platelet rich fibrin (PRF) [Table/Fig-4] was placed on apical region of anteriors [Table/Fig-5]. The horizontal envelope mucoperiosteal flap was extended to the apical region of the anteriors. The mucoperiosteal flaps were replaced and sutured with 4-0 silk sutures. The patient was given amoxicillin, 500 mg t.i.d. for 3 days. The sutures were removed after a week and advised to use chlorhexidine mouthrinse 0.12% b.i.d for 2 weeks.




After prf placement using tungsten carbide bur




Lateral ceph before treatment
Lateral ceph after treatment





Pre treatment and Post treatment cephalometric values
| Sl No | Angles | Before Intrusion | After Intrusion |
| 1 | SNA(0) | 84 | 83 |
| 2 | SNB(0) | 76 | 76 |
| 3 | ANB(0) | 8 | 7 |
| 4 | GOGN/SN(0) | 33 | 33 |
| 5 | UI-PP(0) | 125 | 106 |
| 6 | UI-PP(mm) | 33 | 30 |
| 7 | CR-PP(mm) | 16 | 13 |
| 8 | UI-PTV(mm) | 56 | 53 |
| 9 | UI-VR(mm) | 62 | 60 |
| 10 | U6-PTV(mm) | 27 | 26 |
| 11 | U6-VR(mm) | 34 | 33 |
| 12 | U6-SN(0) | 74 | 73 |
| 13 | IMPA (0) | 92 | 92 |
| 14 | OVERJET(mm) | 6 | 2 |
| 15 | OVERBITE(mm) | 5 | 2 |
| 16 | Ls-E PLANE(mm) | 4 | 3 |
| 17 | Li-E PLANE(mm) | 2 | 2 |
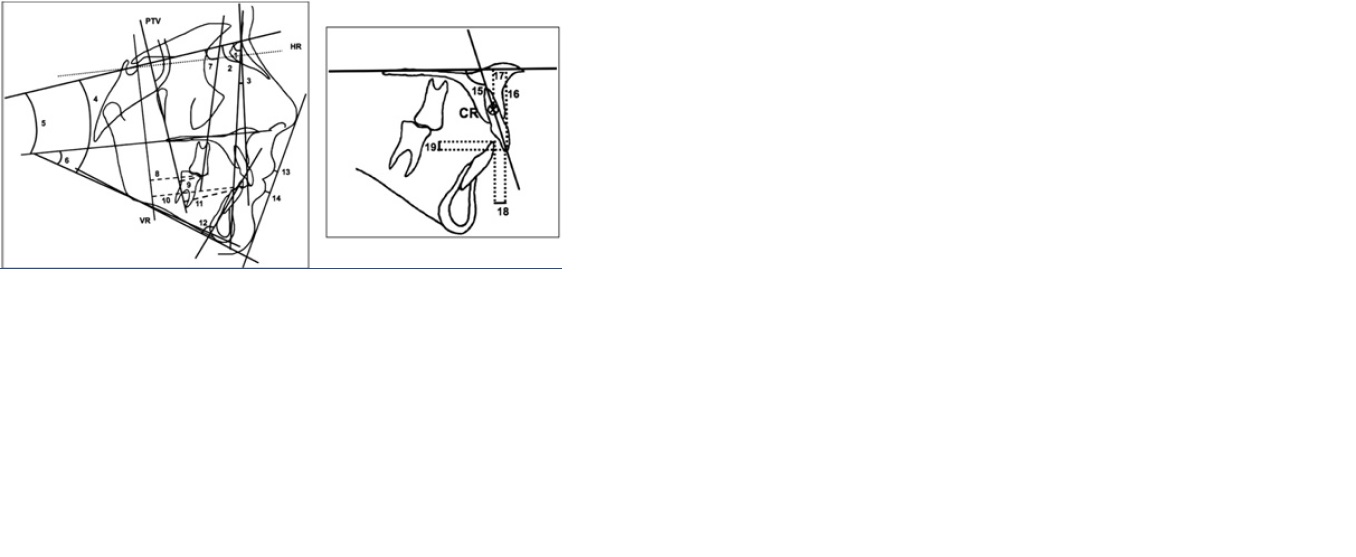
Diagram illustrating linear & angular measurements
Orthodontic Procedures
Fully banded maxillary and mandibular arches with 0.022’ x 0.028’ slot with MBT prescription was started and reached a stage of 17 x 25 S.S wire before periodontal surgery. Soon after a week of periodontal surgery, Burstone three piece intrusive arch in 17x 25TMA wire was given for simultaneous intrusion and retraction and the anterior segment was stabilised with 17 x 25 S.S wire [Table/Fig-6,7,8,9] Patient was recalled once in fifteen days and activation of the intrusion arch was done. 20 to 25 gm of intrusive force was given after four months of periodontal surgery and orthodontic treatment, deep bite got reduced from 5 mm to 2 mm. Anterior space closure was done and overjet reduced from 6 mm to 2 mm [Table/Fig-10,11,12,13,14,15] Eight months after the surgery, detailing of the occlusion was completed [Table/Fig-16]. Seventeen measurements (7 angular, 10 linear) were made on the cephalometric tracings [Table/Fig-17]. Two vertical reference planes were constructed for measurement confirmation of the dental movements. The first reference was the pterygoid vertical (PTV) drawn perpendicular to the sella-nasion (SN) plane, and the second was drawn perpendicular to the constructed horizontal plane (70to the SN plane) from the point of intersection of the anterior wall of sella turcica and the anterior clinoid process (VR). The center of resistance (CR) of the maxillary central incisor was determined rather than the CR of the anterior segment because of its ease of location and high reproducibility. The CR of the maxillary central incisor was taken as the point located at one-third of the distance of the root length apical to the alveolar crest. Results revealed that Skeletal variables SNA and ANB angle decreased slightly, GoGnSN did not show any significant change. UI-PP(0), UI-PP(mm), CRPP(mm) UI-PTV(mm), UI-VR(mm) changed slightly. The following cephalometric parameters were consider for comparing pre and post results [Table/Fig-17].
The following orthodontic results were achieved:
Ideal occlusion was obtained
Deep bite correction was from 5 mm to 2 mm
Anterior spacing was closed
Straight profile was obtained
Pleasant smile was achieved
1.SNA; 2. SNB; 3. ANB; 4. GoGn SN; 5. SN-PP; 6. GoGn-PP; 7. U6-SN; 8. U6-VR; 9. U6-PTV; 10. U1-VR; 11. U1-PTV; 12. IMPA; 13. Ls–E-plane; 14. Li–E-plane; 15. U1-PP; 16. U1-PP; 17. CRPP; 18. overjet; 19. overbite.
Discussion
Optimal force for effective intrusion without root resorption is 20 to 25g per tooth for maxillary anteriors. If the PAOO procedure is performed, heavy intermediate force is the best protocol, because it will initiate rapid tooth movement (RAP) [13]. According to Macfadden et al, treatment time was the most significant factor for occurrence of root shortening. Faster intrusion reduced root shortening [14,15,13].According to Hajii an average treatment time for the PAOO procedure was one-third to one-fourth of traditional orthodontic treatment [16]. Pure incisor intrusion is obtained and flaring is controlled by tying back the intrusion arch at the molar. Posterior tooth tend to tip back and extrude that help in deep bite correction [11]. Seong-Hun Kim et al., stated that prevention of root resorption and shorter treatment time were associated to the PAOO procedure. Wilcko et al., reported an average of 6.1 months of treatment time for the PAOO procedure [10].
Conclusion
Alveolar corticotomy is an effective treatment to decrease the treatment time, reduces the incidence of root resorption and it increases the quality of the treatment. Conservative corticotomy technique eliminates the lingual approach which reduces the operation time and patient discomfort. This technique would be expected to reduce the risk of moving the roots through the labial plate and reduce the risk of gingival recession.
[1]. An Adult Bimaxillary Protrusion Treated With Corticotomy-Facilitated Orthodontics And Titanium Miniplates. Shoichiroiinoa, Sumiosakodab, Shouichimiyawaki.Angle Orthodontist 2006 76(6) [Google Scholar]
[2]. Mostafa Yehya Ahmed, Elbokle Nader Nabil, Fayed Mona Mohamed Salah, . Samahmehanni, Mostafaheider. Ahmed, Comparison of Corticotomy- Facilitated Vs Standard Tooth-Movement Techniques In Dogs With Miniscrews As Anchor UnitsAm J Orthod Dentofacialorthop 2009 136(540):4 [Google Scholar]
[3]. Administration Pgei, W Lee, Experimental Study of The Effect of Prostaglandin Administration On Tooth Movement With Particular Emphasis On The Relationship To The Method ofAm J Orthod Dentofacialorthop 1990 98(231):41 [Google Scholar]
[4]. Ah Mohammed, Dn Tatakis, R Dziak, Leukotrienes In Orthodontic MovementJ Orthoddentofacialorthop 1989 95:231-7. [Google Scholar]
[5]. J Yamasaki K, The Role of Cyclic Amp, Calcium and Prostaglandins in the Induction of Osteoclastic Bone Resorption Associated With Experimental Tooth MovementDent Res 1983 62:877-81. [Google Scholar]
[6]. Mk Collins, Pm Sinclair, The Local Use Of Vitamin D To Increase. The Rate of Orthodontic Tooth Movement.Am J Orthoddentofacial Orthop 1998 94:278-84. [Google Scholar]
[7]. Ej Liou, Cs Huang, Rapid Canine Retraction Through Distraction of The Periodontal LigamentAm J Orthoddentofacialorthop. 1998 114:372-82. [Google Scholar]
[8]. A Ren, T Lv, N Kang, B Zhao, Y Chen, D Bai, Rapid Orthodontic Tooth Movement Aided By Alveolar Surgery In Beagles.Am J Orthod Dentofacialorthop. 2007 131(160) [Google Scholar]
[9]. Oliveira Dauro Douglas, Oliveira Bruno Franco De, Rodrigo Villamarimsoares Alveolar Corticotomies In Orthodontics: Indications And Effects On Tooth MovementDental Press J Orthod 2010 15(4):144-57. [Google Scholar]
[10]. Kim Seong-Hun, Kook Ywoon- Ah, Jeong Do-Min, lee Won, Chung Kyu-Rhim, Nelson Gerald, Clinical application of accelerated osteoginic orthodontic and partially osseo integrated mini implants for minor tooth movement. AmericanJournal Of Orthodontics And Dentofacial Orthopedics 2009 136(431):3 [Google Scholar]
[11]. . Dds, . Mdentsc, Yoon Won M, Lindauerdmd Steven J, Ddse Charls J Burrstone, Simultaneious intrusion and retraction using three-piece base arch.The Angle Orthodontist 1997 67:6 [Google Scholar]
[12]. Long Hu, Pyakurel Ujjwal, Wang Yan, Liao Lina, Zhou Yang, Interventions For Accelerating Orthodontic Tooth Movement A Systematic Review. Angle Orthodontist 2013 83:1 [Google Scholar]
[13]. Yeollee Dong, Gukpark Young, Suwon Seoul, Hun Califseong, Chung Kyu-Rhim, Accelerated Decompensation of Mandibular Incisors In Surgical Skeletal Class Iii Patients By Using Augmented Corticotomy:A Preliminary Study Hyo-Won AhnAmerican Journal Of Orthodontics And Dentofacial Orthopedics. 2012 142(2):4 [Google Scholar]
[14]. Mcfadden W. Michael, . Dmd, Christerengstrom, Ms,”, Engstrom Helene, Odont Dr., A study of the Relationship between incisor intrusion and root shortening.Am. J. Orthod. Denrofac, Orthop 1989 96:5 [Google Scholar]
[15]. Nowzari Hessam, Yorita Frank Kazuo, Chang Hsuan Chen, Periodontally Accelerated Osteogenic Orthodontics Combined With Autogenous Bone Grafting CompendiumAm J Orthod Dentofacialorthop 2008 29:4 [Google Scholar]
[16]. Ss Hajji, Louis St, The Influence of Accelerated Osteogenic Responses on Mandibular De-Crowding [Thesis]. Mo; St Louis University 2000 [Google Scholar]