Case report
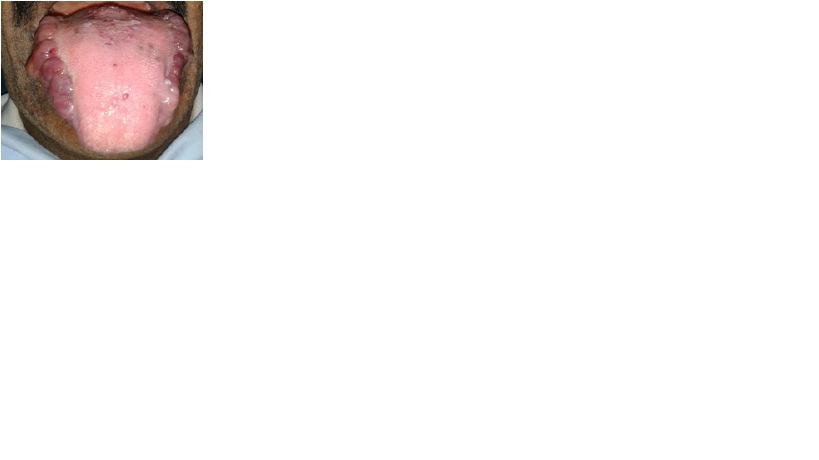
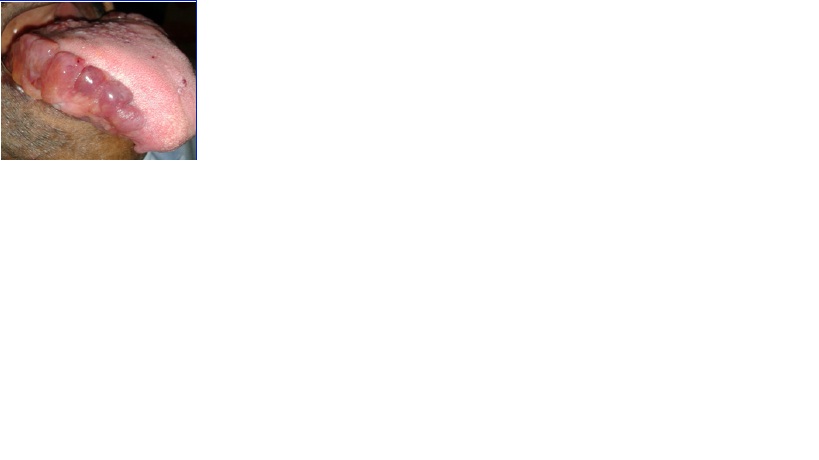
A 54–year–old man reported with swelling of tongue, which had been seen since one year. On examination, he appeared to be in good general health, but his speech had been slurred ostensibly, due to tongue swelling. On clinical examination, the patient was found to be edentulous, with tongue grossly enlarged, with multiple rubbery nodules and striations on the lateral borders [Table/Fig-1,Table/Fig-2]. No ulcerations were seen over the surface. Bilaterally symmetrical violaceous purpuric patches which were interspersed with nodules were seen surrounding the eyes. Well circumscribed hyperpigmented plaques were present over the nasal bridge [Table/Fig-3]. Similar small nodules were also seen on the right angle of the mouth and on ala of the nose.
An incisional biopsy was performed on the lateral border of the tongue. Histopathological examination of haematoxylin and eosin (H and E) stained sections revealed extracellular deposition of amorphous, eosinophilic hyaline-like material in the sub-mucosal connective tissue, which appeared to be amyloid [Table/Fig-4]. To confirm the presence of amyloid, a special staining with Congo red was performed, which showed peach red colour on light microscopy [Table/Fig-5] and apple green birefringence on polarized light microscopy [Table/Fig-6].
To rule out a systemic involvement, we performed a series of investigations, which included biochemical tests which included urine for Bence-Jones proteins, serum proteins, serum immunoglobulin levels, liver function tests, cardiac and renal evaluation. All these results turned out to be negative. Based on these findings, a definitive diagnosis of amyloidosis of tongue was given.
Extra oral photograph showing bilateral symmetrical violaceous purpuric patches interspersed with nodules surrounding the eyes

Intraoral photograph showing bilateral involvement of the lesion
Intraoral photograph showing the lesion involving the lateral side of the tongue
Photomicrograph of the lesion showing surface epithelium ,homogenous eosinophilic area in the connective tissue (H & E, 10x)

Photomicrograph of the lesion showing surface epithelium,amyloid appears as peach redcolor, in the connective tissue (Congo red, 10x)

Photomicrograph of the lesion showing apple green birefrengence .(Stained with congored and observed under polarized microscopy)

Discussion
Amyloidosis of the oral cavity is uncommon. The tongue is the most frequent site, followed by the floor of the mouth, buccal mucosa, soft palate, gingiva, hard palate and lower lip region [1].The head and neck region is affected in 12-90% of the amyloidosis patients [2]. It can also affect pharynx, orbital sinuses, larynx and salivary glands [3].
Amyloid results from an abnormal folding of proteins which are not recyclable or biodegradable and cannot be broken down easily. Therefore, the body finds it difficult to remove these proteins. This leads to the formation of oligomeres and fibrils, that are deposited in tissues and organs [4,5].
Amyloidosis can be acquired (it develops over time due to unknown reasons) or hereditary (it occurs due to a faulty gene which is passed on within families). It can be localized (amyloid protein is produced and deposited only in one small area of the body), or systemic (amyloid protein circulates in the blood and it gets deposited in one or several organs of the body) [4].
Earlier, amyloidosis was typically classified into four major types: primary amyloidosis, secondary amyloidosis, familial or hereditary amyloidosis and localized amyloidosis. Primary amyloidosis includes deposition of fibrillar aggregates of monoclonal immunoglobulin light chain in vital organs like liver, heart, kidney, liver, spleen. Secondary amyloidosis is a serious complication of some primary diseases such as rheumatic arthritis, multiple myeloma, chronic suppuration, Hodgkin’s lymphoma, tuberculosis, Syphilis And Rickets [6,7].
Hereditary or familial amyloidosis occurs when a gene mutation is inherited, leading to the life-long production of an abnormal protein. The most common types of hereditary amyloidosis are ATTR (transthyretin gene mutation) and AFib (fibrinogen alpha chain gene mutation) [4,7].
Localized amyloidosis is a rare type of amyloidosis which is not associated with either multiple myeloma or systemic amyloidosis and which does not usually progress to systemic amyloidosis [2]. Head and neck involvement of amyloidosis is commonly seen in both localized and systemic forms of this disease. Cases of localized tongue amyloidosis are extremely rare, with not more than 30 cases being reported in the literature so far. Present case was a localized form of disease
Symptoms vary greatly from patient to patient and between the different types of amyloidosis. Symptoms are often vague, mimicking other medical conditions. The most common symptoms are fatigue, unexplained weight loss, swelling of the ankles and legs due to fluid accumulation (oedema), shortness of breath, loss of appetite, an enlarged tongue (macroglossia), unexplained bruising around the eyes, numbness or tingling in the hands and feet (peripheral neuropathy) [8]. Our patient did not show any of the above features.
Clinically, for generalized macroglossia, besides amyloidosis, one should consider tuberculosis, lymphangioma, hypothyroidism,acromegaly, granular cell tumours, lingual infarction caused by giant cell arteritis, idiopathic muscular hypertrophy and Beckwith- Wiedemann syndrome under differential diagnosis [9]. All these pathologies were ruled out after the biopsy was done, which furnished the final diagnosis as confirmed amyloidosis [2].
Localized amyloidosis of tongue typically presents as macroglossia, tongue protrusion beyond the alveolar ridge, speech impairment and dysphagia [4]. On the lateral borders, they present as yellow or raised white nodules. Kyle and Bayrd, in their review, found only 22 cases (9%) that were localized [10]. Kerner et al., University of California, Los Angeles, reported a similar series. They observed that localized amyloidosis did not evolve to primary or secondary systemic amyloidosis or multiple myeloma[11]. In a review made by Kenji et al., a total number of 5 cases had been reported, which did not have any secondary involvement (Angiero et al,. Haraguchi et al., Koren et al.,). Our present case also showed similar features as were reported in the above studies [12].
All amyloid deposits share the following physical characteristics, which include (a) appearance of amorphous, eosinophilic deposits under light microscope after haematoxylin and eosin staining (b) a bright, apple green birefringence under polarized light after staining with Congo red, and (c) a β-pleated sheet structure which is demonstrated on x-ray diffraction [13]. An oral involvement is extremely rare, but when it is involved, it presents primarily on the tongue. The present case fulfilled all these criteria.
It is very essential to rule out systemic from localized amyloidosis, since the aetiology, treatment and outcome of both vary. This can be done by carrying out extensive biochemical investigations, which include serum and urine immunofixation, to detect Bence-Jones Proteins and by doing a bone marrow examination for plasma cell dyscrasia [7]. An echocardiogram can be obtained, to rule out a cardiac involvement. Abdominal fat biopsy, which according to Dr G Gallo’s experience had a 94% success rate, shows positivity if systemic amyloidosis is involved[14].All the above tests were negative in our case
We can also use ancillary techniques like magnetic resonance imaging, Tc-99m phosphate radionuclide imaging and I serum amyloid P scintigraphy [2]. Surgical excision is usually the treatment of choice. Our patient refused any surgical intervention. Adjuvant therapies like chemotherapy and steroids were not beneficial [13].
There is no cure for amyloidosis. The prognosis is poor in generalized and myeloma associated amyloidosis; those with immunocyte derived amyloidosis have a median survival rate of two years after the diagnosis. Treatment is essential, which is given to suppress the development of the amyloid-forming protein. If amyloidosis is related to another condition, then treatment will include targeting of that underlying condition. Our patient refused to take treatment, because it did not cause any major problem for him.
In summary, amyloidosis of tongue is rare and its features resemble those of a benign tumour. A series of tests are necessary to rule out all the possible known aetiological factors which are cause for secondary amyloidosis. New therapeutic strategies are targeted at correcting protein misfolding and inhibitory fibrillogenesis.
[1]. Andreadis Dimitrios, Poulopoulos Athanasios, Papadopoulos Petros, Epivatianos Apostolos, Localized Tongue Amyloidosis in a Patient with Neurofibromatosis Type II.Head and Neck Pathol 2011 5:302-305. [Google Scholar]
[2]. Fahrner Kristen S, Black Candice C, Gosselin Benoit J, Localized Amyloidosis of the Tongue: A ReviewAm J Otolaryngol 2004 25(3):186-89. [Google Scholar]
[3]. Balatsouras Dimitrios G, Eliopoulos Panayotis, Dimitrios Assimakopoulos, Stavros Korres. Primary local amyloidosis of the palate.Otolaryngol Head Neck Surg. 2007 137(2):348-49. [Google Scholar]
[4]. Memari Faramarz, Jahandideh Hesam, Moghtader Khosro, Harandi Ali Amini, Narrowing of the upper airway due to amyloidosis: A case report.Journal of Clinical Medicine and Research 2011 3(4):52-56. [Google Scholar]
[5]. Neely Pat, Understanding amyloidosis: a guide for patients and families. December 2010, booklet, Leukemia Foundation,www.leukaemia.org.au [Google Scholar]
[6]. LI Yanzhong, Liu Na, Xu Yi, Wang Jiayi, Wu Lanyan, Zhou YU, Zhu Xiaohan, Jin Xin, Chen Qianming, Zeng Xin, Zeng Xin, Widespread purple bulla-like masses of the oral mucosaOral Surg Oral Med Oral Pathol Oral Radiol 2012 114(5):552-557. [Google Scholar]
[7]. Akyildiz S, Doganavsargil B, G¨ode S, A. Veral. Solitary Amyloid Tumor of the Tongue Base.Int J Otolaryngol 2009 515068 [Google Scholar]
[8]. S Robbins, RS Cotran, V Kumar, AK Abbas, Pathologic Basis of Disease 2010 8th edition:258-64. [Google Scholar]
[9]. Topouzelis Nikolaos, Iliopoulos Christos, Kolokitha Olga Elpis, Macroglossia. Int Dent J 2011 61(2):63-69. [Google Scholar]
[10]. RA Kyle, ED Bayrd, Amyloidosis: Review of 236 casesMedicine 1975 54(4):271-99. [Google Scholar]
[11]. MM Kerner, MB Wang, G Angier, Amyloidosis of the head and neck—A clinicopathologic study of the UCLA experience,Arch Otolaryngol Head Neck Surg 1955-1991 121:778-82. [Google Scholar]
[12]. Guvenc Isil Adadan, Amyloidosis-An Insight to Disease of Systems and Novel Therapies.Cleft Palate Craniofac J 2011 10:141-52.www.intechopen.com [Google Scholar]
[13]. Speranza Vinnie Della, , Amyloid, Histologic Preparations: Common Problems and Their Solutions www.cap.org/apps/docs/cap_press/Amyloid.pdf Accessed on 14 Aug 2013. [Google Scholar]
[14]. M Maria, Picken. Amyloidosis—Where Are We Now and Where Are We Heading?Arch Pathol Lab Med 2010 134:545-51. [Google Scholar]