Mandibular Aneurysmal Bone Cyst Associated with Cemento-Ossifying Fibroma – A Case Report
Bhavani S.N1, A Rajesh2, Narendranatha Reddy P3, Firoz Kamal4
1Senior Lecturer,SVS Institute of Dental SciencesAndhra Pradesh, India.
2Reader,CKS Teja Institute of Dental Sciences, Andhra Pradesh, India.
3Reader,CKS Teja Institute of Dental Sciences, Andhra Pradesh, India.
4Senior Lecturer,Nrayana Dental College, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bhavani S.N., Senior Lecturer, Department of Oral Pathology, SVS Institute of Dental Sciences, Mahabubnagar- 509001, Andhra Pradesh, India.
Phone: 9949336268,
E-mail: drbhavani21@yahoo.com
Aneurysmal bone cyst is an uncommon bone lesion which rarely occurs in craniofacial region. Among all the cystic lesions occurring in the jaws, aneurysmal bone cyst is infrequent and it more commonly occurs in the mandible. Most of the cases occur in the first two decades of life, with no gender predilection. Here, we are presenting a case of an aneurysmal bone cyst which occurred in the mandible of a twelve year old female patient.
Aneurysmal bone cyst, Pseudocyst, Ossifying fibroma, Cementifying fibroma, Cavernous hemangioma
Case Report
A twelve-year-old female patient came to our Outpatients Department (OPD) with a complaint of swelling and pain in the right lower back tooth region of the jaw since 10 months. Patient also gives a history of trauma 10 months back in that region. A diffuse extra-oral swelling was seen on the right side lower half of the face, which extended anteroposteriorly from corner of mouth to angle of the mandible, which measured around 4cm in size and which extended superoinferiorly from the ala - line to 1cm below the lower border of mandible, which measured about 3cm in size. The skin over the swelling appeared to be slightly stretched and it was in normal colour as that of the surrounding skin. Swelling was found to be firm in consistency and tender on palpation. There was no rise in temperature. No palpable lymph nodes were detected. A diffuse intra-oral swelling was present, which extended superoinferiorly from the marginal gingiva to the depth of the vestibular sulcus, which Obliterated it. Intra oral swelling superoinferiorly measured about 3 cms in size. It extended anteroposteriorly from distal surface of 43 to distal surface of 47 and measured about 4cm in size.The interdental gingiva between 44 and 46 was erythematous On palpation, swelling was found to be tender and firm, with a tennis ball consistency [Table/Fig-1]. Teeth were firm and vital. Orthopantamograph (OPG) showed a large solitary unilocular radiolucency extending anteroposteriorly from distal aspect of 41 to distal aspect of 47. Superiorly, it extended to the alveolar ridge and inferiorly to right lower border of the mandible. It approximately measured about 7 x 5 cms in size and was surrounded by well-delineated and scalloped borders. Thinning and downward slanting of lower border of mandible and displacement of root of 44 could also be appreciated. [Table/Fig-2]. Provisionally, lesion was diagnosed as a traumatic bone cyst and clinicoradiographic differential diagnosis included ameloblastoma, central giant cell granuloma or aneurysmal bone cyst. Haematological investigations revealed that all the values were within normal limits. Total lesion was surgically curetted and the specimen was sent to Department of Oral Pathology for making a confirmatory diagnosis. During surgical approach, on entering the lesion, excessive bleeding was encountered. Grossly, lesion showed multiple soft tissue bits along with teeth (44 and 46). A larger bit which was seen on the outer aspect showed fragments of thinned out cortical plate which was adherent to solid soft tissue. Inner aspect showed a chocolate-coloured spongy tissue enclosing multiple blood-filled locules [Table/Fig-3]. Multiple bits were taken for processing. Microscopically, H & E stained tissue sections showed many blood-filled cystic spaces of varying sizes, which were lined by spindle/plump fibroblasts, which were admixed with few giant cells. Intervening connective tissue and the solid areas were highly cellular and vascular, with large areas of haemorrhage, haemosiderin deposits, many scattered trabeculae of immature bone with osteoblastic rimming and focal osteoclastic activity, intermixed with spherical basophilic acellular calcified deposits which resembled cemental masses [Table/Fig-4]. The lesion was finally diagnosed as an aneurysmal bone cyst which was secondary to a cemento-ossifying fibroma.
Intra orally 3 x 4 cms sized diffuse swelling was seen on right side of the mandible

OPG reveal a radiolucency anteroposteriorly extending from distal portion of 41 to distal root of 47

Grossly lesion shows multiple soft tissue bits along with teeth (44 & 46)

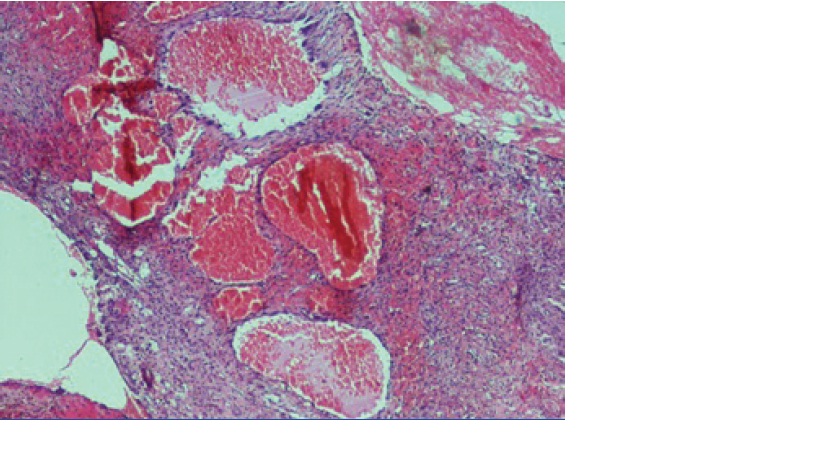
Photomicrograph showing many blood-filled cystic spaces of varying sizes lined by spindle/plump fibroblasts admixed with few giant cells (H&E 10X)
Discussion
An aneurysmal bone cyst (ABC) is a non-odontogenic, nonepithelial cyst which commonly occurs in long bones and spine [1]. According to Bruce et al., only 2-3% of the cases occur in the head and neck region and among them, 66% of the cases occur in jaws [2]. They commonly occur in the first two decades of life and do not show any gender predilection [3]. As compared to maxilla [2–6] they occur more commonly in the mandible [3,7–10]. Lesions may be asymptomatic or they may be commonly associated with swelling [2,5,6,8,9] and/or pain [4,7,10] in the involved area, as it was in the present case. Radiographic features are not diagnostic. Lesions may exhibit unilocular [4,8] or multilocular radiolucencies [7,9,10] and they may also show a blown-out appearance. Unusual features which were seen in the present case were involvement of right mandible, secondary to trauma and its radiographical presentation as a well-defined unilocular radiolucency with scalloped borders.
Origin and pathogenesis of ABC is still an enigma. According to some, it exists as a primary lesion or it may be caused by a secondary phenomenon in both, benign and malignant lesions of bone [1,2]. Microscopically, the lesion consists of many large, blood-filled spaces of varying sizes, which are not lined by endothelial cells and which are separated by loose textured fibrous tissue. Small multinucleated giant cells and scattered trabeculae of osteoid can also be appreciated in the lesion. In the present case, along with the above microscopic features, peculiar areas representing cement ossifying fibromas (COFs) were also evident. Few cases of ABCs which were associated with COFs, which had occurred in the jaws have been reported in the literature [4,7]. According to Rezwana Begum et al., two more cases of ABCs, which had occurred in association with COFs, which had involved the maxilla had been reported [4]. Unlike other cases, the present case and the case reported by Rezwana Begum et al., had a history of trauma. In contrast to the other cases,the present case had occurred in right body of the mandible and had radiographically shown a unilocular radiolucency with scalloped borders. Histologically, the present case needed to be differentiated from cavernous hemangiomas, telangiectatic osteosarcomas and giant cell lesions like giant cell tumours, cherubism, giant cell granulomas and brown tumours. In cavernous hemangiomas; large, dilated blood sinuses show an endothelial lining, but not in ABCs, as immunohistochemical studies reveal negative staining of flattened lining cells of aneurysmal bone spaces by endothelial markers like anti-factor VIII-related antigen and Monoclonal antibody BW-200 [11]. In telangiectatic osteosarcomas, along with large, blood-filled spaces, proliferation of atypical osteoblasts are also observed. In comparison to giant cell lesions, apart from clinical differences, histopathologically, ABCs also show large blood-filled cystic spaces. Surgical excision or curettage is the treatment of choice [1]. Recurrence can be seen in few cases of ABCs [10].
Conclusion
ABCs are rare in head and neck region, with variable clinical and histopathological appearances. As some of the lesions occur as secondary phenomena, multiple bits are taken from various areas of a gross specimen and the sections are observed microscopically, to know the underlying pathology for making a proper treatment plan.
[1]. Shear Mervyn, Speight Paul M, Cysts of the oral and maxillofacial regions 2007 Blackwell Munksgaard Publishers:150-55. [Google Scholar]
[2]. Matt Bruce H, Aneurysmal bone cyst of the maxilla: case report and review of the literature.International Journal of Pediatric Otorhinolaryngology 1993 25:211-26. [Google Scholar]
[3]. Motamedi Mohammad Hosein Kalantar, , Finanavi, , Pooyansadreshkevari, Mehdijafari Seyed, Shams Mohammad Ghasem, Taheri Maryam, Abbas Fatemeh Mashhadi, Motahhari Pourya, Variable presentations of Aneurysmal bone cyst of the jaws: 51 cases treated e H. Matt. Aneurysmal bone cyst of the maxilla: case report and review of the literature.International Journal of Pediatric Otorhinolaryngology 1993 25:217-26. [Google Scholar]
[4]. Mohammed Rezwana Begum, Rani G Shirisha, Chowdary Mundru Supraja, , Arshiashereen, Yellarti Pavan Kumar, Aneurysmal bone cyst of Maxilla – A rare case report and review 2013 6:49-53. [Google Scholar]
[5]. Dursun Ayse, Ataoglu Omur, Edali Naci, Cento-Ossifying Fibroma withan Aneurysmal Bone CystThe Turkish Journal of Pathology 1991 7(1):32-33. [Google Scholar]
[6]. Sankaranarayanan S, Srinivas S, Sivakumar P, Sudhakar R, Elangovan S, “Hybrid” lesion of the MaxillaJ Oral Maxillofac Pathol 2011 15:299-302. [Google Scholar]
[7]. M Parvathi Devi, Chandara Sunira, Singh Gurez, Kaur Navdeep, Cementoossifying fibroma with aneurysmal bone cyst -a rare case reportInternational Journal of Oral Health Sciences and Advances 2013 1:19-23. [Google Scholar]
[8]. S Kiattavorncharoen, U Joos, Brinksschmidt C, Wermeister R, Aneurysmal bone cyst of the mandible: a case reportInternational Journal of Oral and Maxillofacial Surgery 2003 32:419-22. [Google Scholar]
[9]. Shete Anagha, Chavan Mahesh, Diwan Nikhil, Shete Mrinal, Aneurysmal bone cyst: Rarity in mandible and its ambiguity with central giant cell granuloma 2012 4:51-55. [Google Scholar]
[10]. Banu Khurshida, Ehtaih Mohammed, Hari Sri, Sharad Veena, Giant recurrent aneurysmal bone cyst of the mandible.Annals of Maxillofacial Surgery 2012 2:174-77. [Google Scholar]
[11]. Alles JU, Schulz A, Immunocytochemical markers (Endothelial and histiocytic) and ultrastructure of primary aneurismal bone cystHuman Pathol 1986 17:39-45. [Google Scholar]