Intraoral Lipoma: A Rare Case Report and Review of Literature
Ravi Kiran A1, Purnachandrarao Naik N2, Samatha Y3, Vijay Kumar A4, Kalyan Kumar D5
1Professor & HOD, Department of Oral Medicine and Radiology,Sibar Institute of Dental Sciences, Takkellapadu, Guntur, Andhra Pradesh-522509, India.
2Senior Lecturer, Department of Oral Medicine and Radiology,Sibar Institute of Dental Sciences, Takkellapadu, Guntur, Andhra Pradesh-522509, India.
3Reader, Department of Oral Medicine and Radiology,Sibar Institute of Dental Sciences, Takkellapadu, Guntur, Andhra Pradesh-522509, India.
4Senior Lecturer, Department of Oral Medicine and Radiology,Sibar Institute of Dental Sciences, Takkellapadu, Guntur, Andhra Pradesh-522509, India.
5Senior Lecturer, Department of Oral Medicine and Radiology,Sibar Institute of Dental Sciences, Takkellapadu, Guntur, Andhra Pradesh-522509, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Purnachandrarao Naik N., Department of Oral Medicine and Radiology, Sibar Institute of Dental Sciences, Takkellapadu, Guntur, Andhra Pradesh-522509, India.
Phone: 09989857600,
E-mail: purnachandraraonaik@gmail.com
Benign soft tissue neoplasms commonly occur in oral cavity. Lipoma is one such benign tumour which rarely occurs in the oral mucosa. About 20% of lipomas occur in the head and neck region among which oral lipomas comprise only 1-4% of all lipomas. They slowly enlarge and they are known to grow to large sizes, thus causing mastication and speech difficulties. Usually, the lesion consists of a well circumscribed, lobulated mass of mature fat cells. Oral lipomas are usually asymptomatic, but in some situations, the covering mucosa becomes ulcerated and it presents difficulties in diagnosis. Here with, the present paper reports a rare case of intaoral lipoma in a 53-year-old female patient
Lipoma, Neoplasm, Oral cavity
Case Report
A 53-year-old female patient was reported to the department with chief complaint of a growth in right side of the cheek region. History of presenting illness revealed that the growth was small at the time of her initial observation, 2 years back, which had gradually enlarged and had attained the present size. It was not associated with any pain, but pain was occasionally felt, with some discomfort, while chewing food. On intraoral examination, a single, dome shaped, sessile growth was noted on the right buccal vestibular region, whose size was approximately 1×1 cm in diameter, which was well circumscribed, smooth surfaced. The colour of the growth was normal to that of the adjacent mucosa. Palpatory findings revealed that it was soft in consistency, with slippery borders and that it was non-tender [Table/Fig-1].
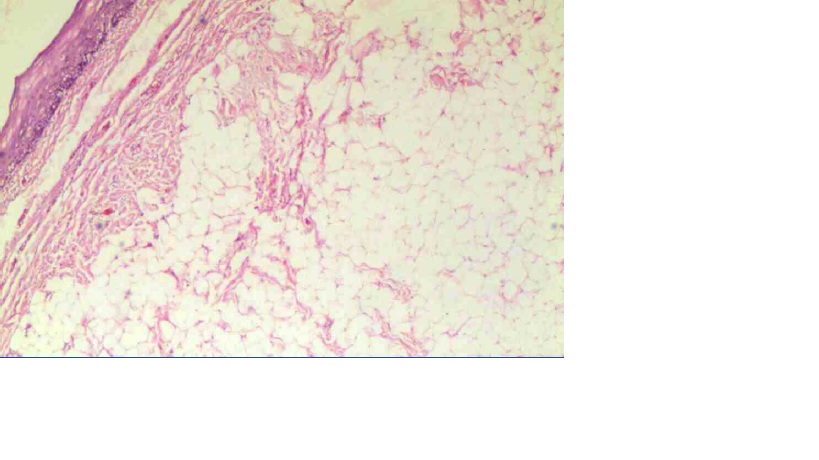
Provisionally, a diagnosis of a fibroma was given, based on its above mentioned clinical features, and a first differential diagnosis of a lipoma was given, because of its consistency and slippery borders. The lesion was excised completely and it was sent for a histopathological examination. Histopathological picture showed parakeratinized, stratified, squamous epithelium and fibrocellular connective tissue stroma, having large round to oval vacuolated cells with peripheral flat nuclei, resembling adipocytes [Table/Fig-2]. By correlating both the above clinical and histological findings, a final diagnosis of an intraoral lipoma was made.
Intra oral growth on the right buccal vestibular region

Photomicrograph showing fibrocellular connective tissue stroma, having large round to oval vacuolated cells with peripheral flat nuclei resembling adipocytes
Discussion
Since, the buccal mucosa is the region where there is abundant fatty tissue, it is reported to be the most common location of lipomas which occur in the oral cavity, followed by tongue and hard palate, which show very low occurrences of lipomas because they have lesser fatty tissues [1]. The aetiology and pathogenesis of lipoma remain unclear, but few influences have been reported in the literature, that include endocrine, mechanical, and inflammatory causes[2,3]. Very few reported cases of intra oral lipomas have shown rearrangements of 12q, 13q, and 6p chromosomes [4]. Clinically, these are painless, mobile, sub-mucosal nodules, which have a yellowish colour. They can be sessile or pedunculated, and the consistency varies from soft to firm [5].
Clinically, differential diagnosis of lipomas include dermoid cysts, ranulae, thyroglossal duct cysts, pleomorphic adenomas, ectopic thyroid tissues, mucoepidermoid carcinomas, angiolipomas, fibrolipomas and malignant lymphomas. Oral lymphoepithelial cysts present as painless, movable, sub-mucosal nodules with a yellow or yellowish-white colouration. They differ from oral lipomas in which the nodules are small at the time of diagnosis and they usually occur in the first to third decades of life. Also, most of the oral lymphoepithelial cysts are found on the floor of the mouth, soft palate and mucosa of the pharyngeal tonsil, which are uncommon sites for occurrence of oral lipomas [6]. Oral dermoid and epidermoid cysts present as sub-mucosal nodules and they typically occur on the midline of the floor of the mouth; but they can also occur in other locations of the oral mucosa [7]. Sometimes, oral lipomas can present as deep nodules with a normal surface colour. In such situations, salivary gland tumours and benign mesenchymal neoplasms should also be included in the differential diagnosis [7]. The definitive diagnosis of lipomas depends on correlation between the clinical and histological features.
Histopathology is considered to be the gold standard in the diagnosis of lipomas. The diagnosis is made, based on pathology of an incisional or excisional specimen and an important feature is that the tumour tends to float when it is placed in a 10% formaldehyde solution.
The treatment of oral lipomas is a simple surgical excision. Recurrence of intra-oral lipomas is rare, but intra-muscular type of lipomas have a higher recurrence rate because of their infiltrative growth pattern, but this type of variant is rare in the oral and maxillofacial region[8].
Conclusion
Intraoral lipomas are very rare and they are slow growing in their clinical course. Clinicians must be able to recognize these rare entities clinically, by differentiating them from other entitities, so that adequate surgical excisions can be done, in order to reduce the recurrence rate and to thereby ensure that the patients get comfort and quality of life.
[1]. T Sakai, S Iida, M Kishino, Sialolipoma of the hard palateJ Oral Pathol Med 2006 35(6):376-78. [Google Scholar]
[2]. ER Fregnani, FR Pires, R Falzoni, MA Lopes, PA Vargas, Lipomas of the oral cavity: clinical findings, histological classification and proliferative activity of 46 cases.Int J Oral Maxillofac Surg 2003 32(1):49-53. [Google Scholar]
[3]. MC Aust, M Spies, S Kall, A Gohritz, P Boorboor, P Kolokythas, Lipomas after blunt soft tissue trauma: are they real? Analysis of 31 casesBr J Dermatol 2007 157:92-9. [Google Scholar]
[4]. MA Furlong, JC Fanburg-Smith, EL Childers, Lipoma of the oral and maxillofacial region: Site and subclassification of 125 casesOral Surg Oral Med Oral Pathol. Oral Radiol Endod 2004 98(4):441-50. [Google Scholar]
[5]. RP Kaur, S Kler, A Bhullar, Intra-oral lipomas: Report of three casesDent Res J (Isfahan) Winter 2011 8(1):48-51. [Google Scholar]
[6]. CM Flaitz, Oral lymphoepithelial cyst in a young childPediatr Dent 2000 22(5):422-3. [Google Scholar]
[7]. F Longo, P Maremonti, GM Mangone, G De Maria, L Califano, Midline (dermoid) cysts of the floor of the mouth: report of 16 cases and review of surgical techniques.Plast Reconstr Surg 2003 112(6):1560-5. [Google Scholar]
[8]. Raj Mahendra, Ramadoss Tanuja, Anuradha G, Devi Shobana, Intraoral lipoma: review of literature and case reportJournal of Indian academy of oral medicine and radiology January–March 2012 24(1):36-38. [Google Scholar]