Dentulous Appliance for Upper Anterior Edentulous Span
Paul Chalakkal1, Ramisetty Sabitha Devi2, G. Vijay Srinivas3, Pammi Venkataramana4
1Lecturer, Department of Pedodontics and Preventive Dentistry,Goa Dental College and HospitalBambolim, Goa – 403202, India.
2Reader, Department of Oral Pathology,St. Joseph Dental College, Duggirala, Eluru, Andhra Pradesh, India.
3Professor & HOD, Department of Oral Pathology,St.Joseph Dental College, Duggirala, Eluru, Andhra Pradesh, India.
4Professor & HOD, Department of Oral Medicine,Lenora Dental College, Rajanagaram, Rajahmundhry, Andhra Pradesh, India.
Dr. Paul Chalakkal, Lecturer, Department of Pedodontics and Preventive Dentistry, Goa Dental College and Hospital, Bambolim, Goa – 403202, India.
Phone: 99605 83896,
E-mail: atomheartpaul@yahoo.com
This article discusses about a fixed dentulous appliance that was constructed to replace the primary upper anterior edentulous span in a four year old girl. It constituted a design, whereby the maxillary primary second molars were used to support the appliance through bands and a wire that contained an acrylic flange bearing trimmed acrylic teeth, anteriorly. The appliance was functionally and aesthetically compliant.
Edentulous, Aesthetic, Fixed dentulous appliance, Space maintainer
Case Report
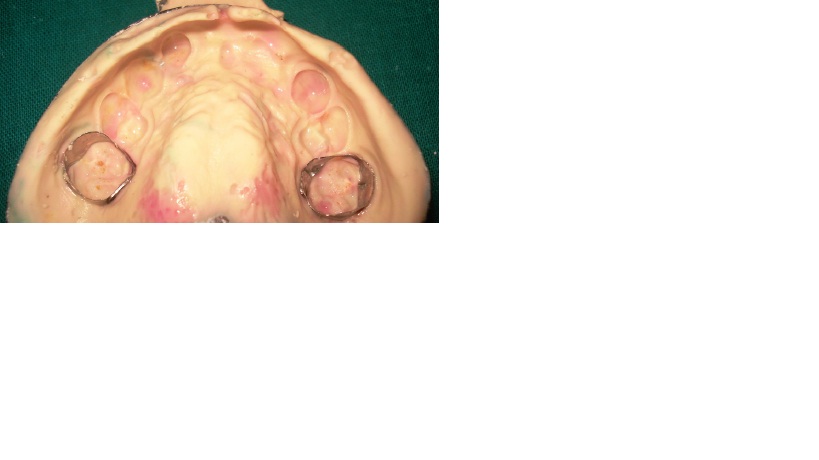
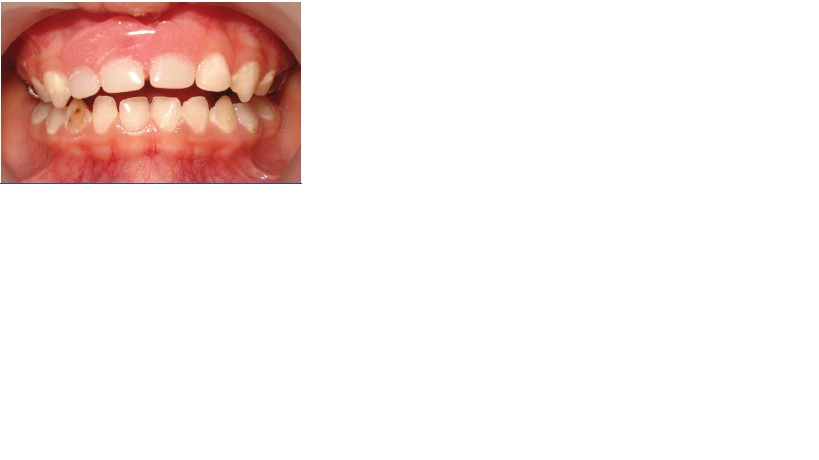
A four year old girl reported to the Department of Pedodontics and Preventive Dentistry with a complaint of missing upper anterior teeth. On examination, 52, 51 and 61 were found to be absent [Table/Fig-1,2]. An investigation revealed that these teeth were avulsed during a traumatic fall which had taken place about six months ago. The patient had not visited a dentist after the injury and the teeth were never retrieved. The patient and her parents were concerned with the deprived anterior aesthetics. It was decided to make a fixed dentulous appliance for replacing the missing anterior teeth. 55 and 65 were banded (band size: 0.005” x 0.180”) and alginate impressions [Table/Fig-3] were made for the upper and lower arches. Contra-indications of inserting anterior fixed appliances may include children with seizure disorders; mental retardation; a poor ability to be followed-up; very poor hygiene; immune- compromised patients; continuation of inappropriate feeding habits; and significant deep-bite, over-jet, or anterior crossbite. However, our patient did not suffer from any of the above conditions or issues.
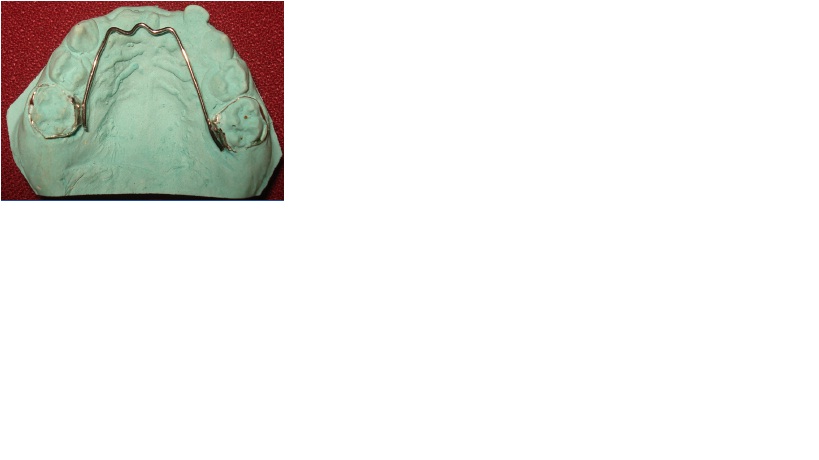
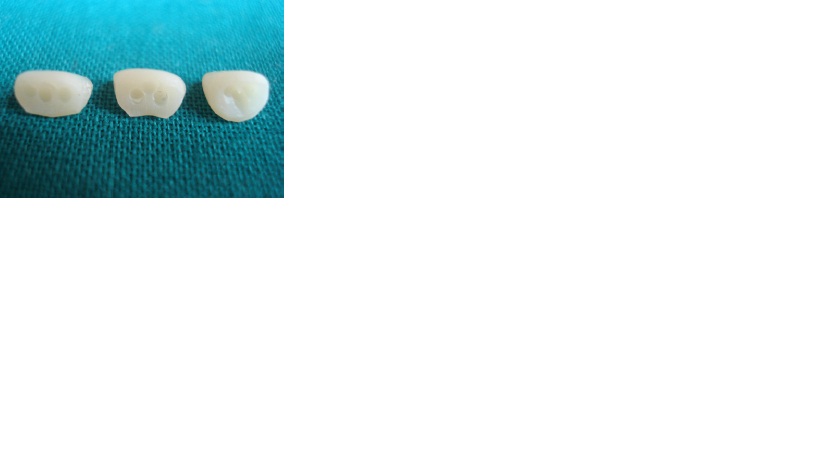
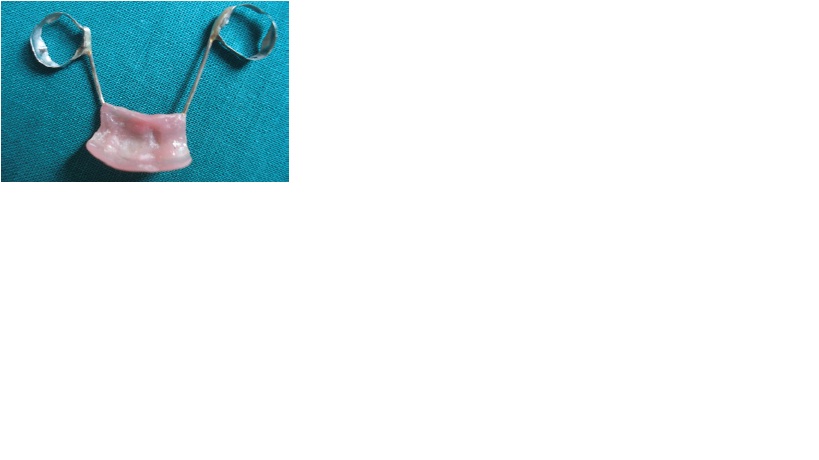
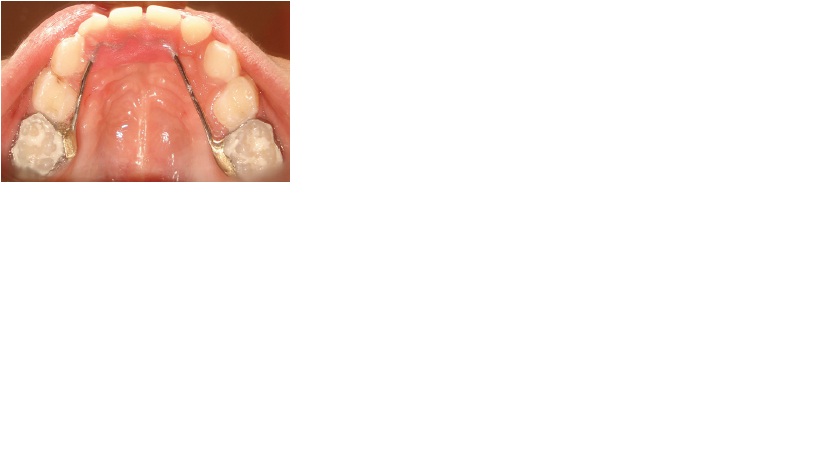
Casts were poured with dental stone. On the upper cast, a stainless steel wire (0.9 mm) framework was made, spanning from one band to the other, while making a zig-zag pattern in the anterior region [Table/Fig-4]. The anterior zig-zag wire pattern was made to reinforce the acrylic segment. The ends of the wire were then soldered to the corresponding molar bands. In the anterior region of the upper cast, a trial wax up was done with trimmed acrylic teeth (B1 shade, Acry Rock, Ruthinium® Group, New Delhi), India. The acrylic teeth were originally of adult size, which had to be trimmed to the primary tooth sizes of 52, 51 and 61 [Table/Fig-5]. Retention holes [Table/Fig-6] were created with a no: 4 round bur on the base of the teeth, so that heat cure acrylic could flow into them. After all necessary adjustments, dewaxing was carried out. After cold mould seal application and heat cure acrylic resin insertion, the cast was heat cured. The appliance was then removed from the cast [Table/Fig-7,8] and it was tried intra-orally [Table/Fig-9]. After necessary trimming and polishing, the appliance was cemented with glass ionomer luting cement (GC Corporation, Tokyo, Japan) via the molar bands on 55 and 65 [Table/Fig-10,11].
Anterior view showing absence of 52,51 and 61,

Maxillary occlusal view showing absence of 52,51 and 61

Upper alginate impression with molar bands
Upper cast with bands and wire

Trimmed acrylic teeth with retention holes
The appliance (tooth surface)
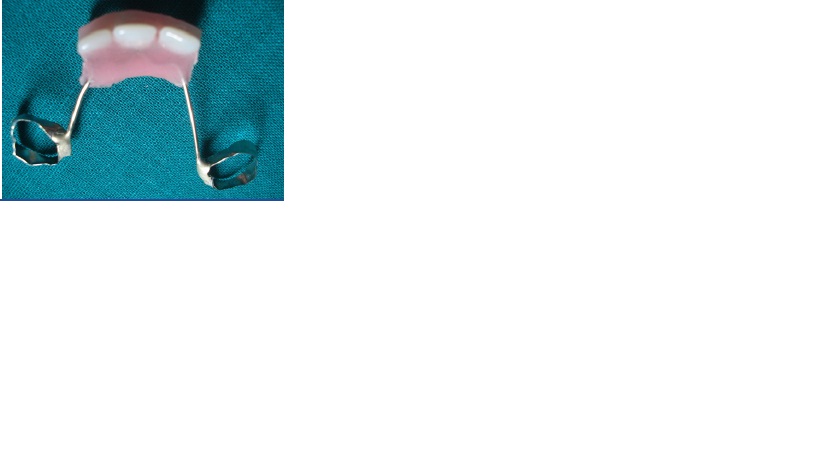
The appliance (gingival surface)
The appliance (after insertion)
The appliance (after cementation)
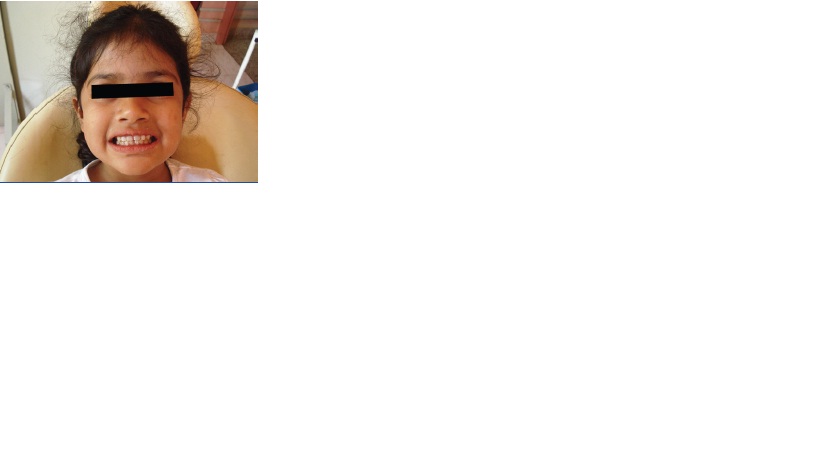
The appliance (facial view)
Discussion
The factors associated with anterior tooth loss include: tipping of adjacent teeth, over-eruption of antagonist teeth, midline deviation, masticatory impairment, speech problems and lingual dysfunction [1]. The reasons for replacing the edentulous upper anterior span with an aesthetic appliance constitute parental desire, space maintenance,restoration of aesthetics and maintenance of function [2]. Children who are under five years of age, with anterior absence of teeth, are seldom affected socially, because of limited exposure to peers unlike school aged children. However, children who attend daycare or preschool programs may become aware of their appearance. As they enter school, they may be comfortable, fitting into groups of children who actively exfoliate primary incisors [3].
Absence of maxillary anterior teeth, the lingual sides of which are needed by the tongue for certain phonations, may result in improper speech [4,5] It usually affects sounds such as ‘s’, ‘z’ and ‘th’ [6]. However, Gable et al found that early loss of incisors had no long term effects on speech [7]. Moreover, parents of children who had their incisors extracted, found no masticatory or speech difficulties in their children [3]. Speech problems are uncommon in children who are over four years of age and if they occur, they are usually compensated and reversible [2]. Our patient had no complaints with mastication or speech, but she had complaints with aesthetics. This was probably because the patient had completed four years of age when the avulsions had occurred and as she was in preschool.
Maintenance of space; prevention of over-eruption of antagonist teeth, restoration of function; allowance for maxillary growth; maintenance of hygiene; durability and low costs, are the requirements of a space maintainer [1]. The appliance which has been discussed is of the fixed type and it bears none of the disadvantages of the removable type, such as need of the patients’ cooperation and chances of breakage. A similar appliance was documented by Jasmine and Groper, in which, plastic teeth were attached to metal cleats that were soldered to the palatal wire bar instead of being attached to acrylic, as it was in our design [8]. Although, their appliance would be superior in hygiene, it may pose the risk of a gap developing between the teeth and the alveolus, due to an improper anterior fit or reduction of ridge height. Although our acrylic flange design would not pose the above risk, lack of hygiene under the inaccessible acrylic flange may result in mucosal inflammatory disease. However, if it happens, the appliance can be temporarily debanded until the tissue heals.
Unlike the posterior segment, the anterior segment from canine to canine appears to be stable, even after early loss of incisors,with no net loss of space between the canines [5]. Moreover, the intercanine growth between ages of two and four years is minimal(less than 0.5mm) and it is clinically insignificant [9]. Changes in arch length with tooth migration generally occur after the eruption of the first permanent molar. At this time, the appliance can be removed, as it coincides with the eruption of the central incisors [2]. In a crowded dentition, if one or more incisors are lost, there may be some rearrangement of space between the remaining incisors, but no space maintenance is required if the loss occurs after the eruption of the primary maxillary canines [10]. Although there were no previous records on whether the patient had spaced, closed or crowded maxillary anterior dentition, it was known that her primary canines had erupted before the avulsion had occurred.
Conclusion
Restoration of anterior aesthetics and function with this appliance gave a huge psychological boost for the child. Oral hygiene instructions were given to the child and her parents. The child had been asked to visit the department at 3-month intervals, in order to monitor issues with regards to hygiene and eruption of the permanent first molars.
[1]. F Liegeois, M Limme, Modified bonded bridge space maintainerJ Clin Pediatr Dent 1999 23:281-84. [Google Scholar]
[2]. WF Waggoner, A Kupietzky, Anterior esthetic fixed appliances for the preschooler: considerations and a technique for placementPediatr Dent 2001 23:147-50. [Google Scholar]
[3]. LD Koroluk, GA Riekman, Parental perceptions of the effects of maxillary incisor extractions in children with nursing caries.J Dent Child 1991 58:233-36. [Google Scholar]
[4]. GA Riekman, HE El Badrawy, Effect of premature loss of primary maxillary incisors on speech.Pediatr Dent 1985 7:119-22. [Google Scholar]
[5]. JR Christensen, FW Fields, Space maintenance in the primary dentition. In: Pinkham JR, editor. Pediatric Dentistry: Infancy through adolescence 1994 2nd editionPhiladelphiaW.B. Saunders Company:358-63. [Google Scholar]
[6]. L Fymbo, The relation of malocclusion of the teeth to defects of speechArch Speech. 1936 1:204-16. [Google Scholar]
[7]. TO Gable, AW Kummer, L Lee, NA Creaghead, LJ Moore, Premature loss of the primary maxillary incisors: Effects on speech production.J Dent Child 1995 62:173-79. [Google Scholar]
[8]. JR Jasmin, JN Groper, Fabrication of a more durable fixed anterior esthetic appliance.J Dent Child 1984 51:124-27. [Google Scholar]
[9]. CC Scures, Report of the increase in bicanine diameter in 2 to 4-year-old childrenJ Dent Child 1967 34:332-35. [Google Scholar]
[10]. P Ngan, SHY Wei, Management of space in the primary and mixed dentitions. In: Wei SHY 1988 Philadelphia: Lea and Febigereditor. Pediatric Dentistry: Total patient care.:462-70. [Google Scholar]