Case Report
A 34-year-old man reported to the Department of Oral Medicine and Radiology, Educare Institute of Dental Sciences, Malappuram, Kerala, India, with chief complaints of bad breath and mobile lower front teeth, which were there since 2 years
The family and medical histories were non-contributory. There were no signs of any identified syndrome.
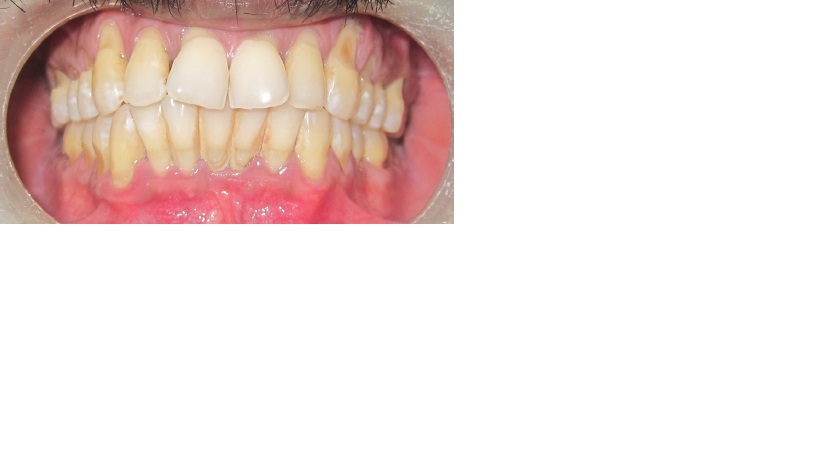
On intra–oral examination, he was found to have severe calculus, generalized cervical abrasion and generalized periodontitis, with mobility with respect to lower incisors. A careful examination revealed five incisors in the mandibular anterior region. All five incisors were separate, with well formed morphologies [Table/Fig-1,2] show five mandibular incisors which are well formed and separate – frontal and occlusal views respectively.
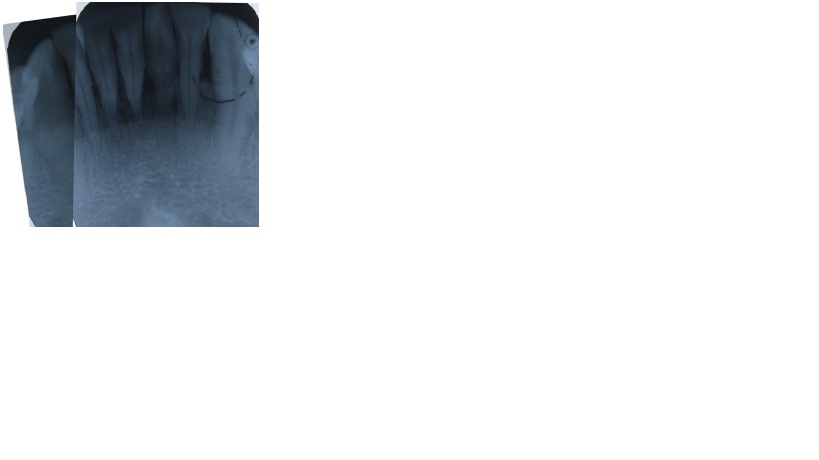
It was a daunting task to distinguish the supernumerary tooth with the normal incisors, clinically or radiographically, as there was no fusion between crowns or roots [Table/Fig-3] is a merged radiograph which shows five mandibular incisors. This was the only supernumerary tooth that was detected in the patient and none was seen among his other family members. The patient himself was unaware of the presence of this additional tooth in that area.
To distinguish between them, the following steps were adopted. During examination, the median area was defined positionally by the inferior labial frenum and radiographically by the genial tubercle; it appeared that the supernumerary tooth was more towards the right side from the midline. Upon carefully examining all 5 incisors clinically and radiographically, a conclusion was drawn that the distal most incisors on either side of midline were normal lateral incisors,as their crown measurements were greater than those of the remaining 3 incisors. Distinguishing the supernumerary tooth among the 3 incisors was quite challenging, as crown measurements of all the 3 were found to be roughly the same. Since the second incisor from left showed a marked rotation and thereby caused crowding, with the presence of labial frenum just in front of the incisor, it was concluded that the tooth positioned centrally was the supernumerary one. A final diagnosis of mandibular mesiodens of supplemental type and chronic generalized periodontitis was made.
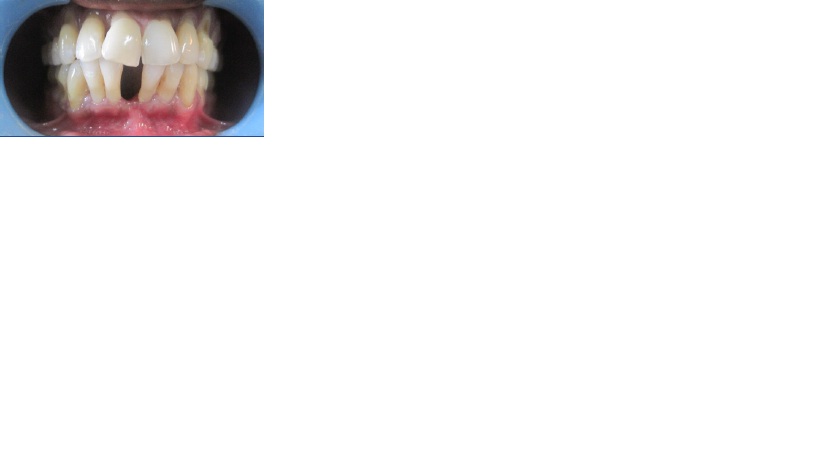
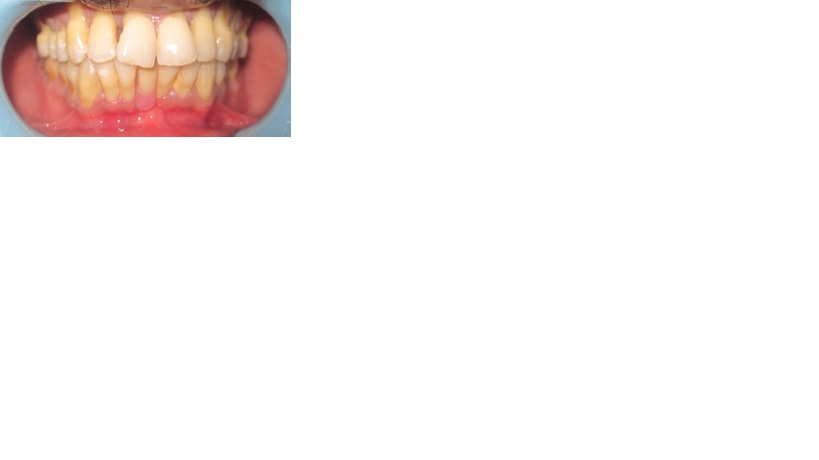
As the tooth was grade II mobile and as the patient was also willing to get the tooth removed, it was extracted uneventfully [Table/Fig-4] shows extracted space of the mandibular mesiodens. Later, the same was replaced by a removable partial denture [Table/Fig-5] shows extracted mesiodens which was replaced by a removable partial denture.
Shows five mandibular incisors which are well formed and separate
frontal and occlusal views respectively

Is a merged radiograph which shows five mandibular incisors
Shows extracted space of the mandibular mesiodensShows extracted space of the mandibular mesiodens
Shows extracted mesiodens which was replaced by a removable partial denture
Discussion
Stafne reported that the incidence of supernumerary teeth in permanent dentition was 1-3% [1]. Most common supernumerary tooth is mesiodens, which is usually small and conical, placed between maxillary incisors [2]. This is generally followed by maxillary lateral incisor, maxillary fourth molar and mandibular third premolars, in descending order. Maxillary premolar, maxillary canine and mandible fourth molar are the least common ones. Approximately 90-98% of all supernumerary teeth occur in the maxilla, with a strong predilection for the anterior region [3,4]. Their incidence in the mandibular anterior region is about 0.01% [5]. Very few cases of 5 mandibular incisors have been reported in the literature [5–9] and no case of supplemental mandibular mesiodens has been distinguished and reported till date.
In the present case, supernumerary mandibular incisor was well formed, separate and normal in all morphological patterns, both clinically and radiographically. In such conditions, their differentiation from their supernumerary counterparts assumes a difficult procedure [9–11]. There are chances of being overlooked, misdiagnosed or ignored attributing to normal appearance.
Occurrence of supplemental teeth in primary dentition is less common, while one fifth of that is seen in permanent dentition. Mesiodens is the most common anomaly which is seen in permanent counterpart. Literature reveals bilateral supplemental lateral incisors in primary dentition occasionally erupt normally [6,12].
The diagnosis, though it is difficult, plays an important role in terms of identifying any syndrome related conditions, wherein multiple supernumerary teeth are a constant feature. The examples of such syndromes are Gardener’s syndrome, acrofacial dystosis, etc [5,6,9,10,11].
Distinguishing between a normal tooth and its supplemental “twin” was difficult in this case. Case reports which have been published earlier have suggested that the supplemental teeth may exhibit deep palatal pits and coronal invaginations, or that when no morphological abnormalities are noted, the tooth with minimum measurement among other anterior teeth is regarded as supernumerary one [5,6].Interestingly, in our case, both these features stood irrelevant.
The origin of such teeth was attributed to autosomal recessive inheritance, which possibly ran through generations. Another theory states that the cause of hyperdontia may be implicated due to “atavism” and /or dichotomy of tooth germ, which can produce two or more separate units [4,9,12,13].
This was not the situation in our case, where the siblings did not report with any supernumerary teeth. A possible association between supernumerary teeth and aggressive periodontitis has been described, though it is uncommon [9]. Reports made by Odell and Hughes in 1995, attributed them to have familial tendencies, with rare occurrences [6,11,14,15]. Our patient reported to us with periodontitis which was generalized and hence, the existence of aggressive periodontitis was ruled out.
Treatment of such anomalies lies not just in identification of the supplemental tooth with normal dentition, but it should be determined as to which tooth is healthy and it should be held logical, to be extracted. The tooth that is most prominently displaced from line of arch or periodontally compromised can be removed [5,9,10].
Whereas those that do not compromise the development of other normal teeth and do not influence their eruption patterns can be observed and immediate treatment should be instituted, if any pathology arises in any instance [4–6,9,12,13].
In our case, the supplemental tooth was periodontially affected and hence, it was extracted and replaced by a removable partial denture.
Conclusion
Mandibular mesiodens is an uncommon occurrence and a supplemental type is an even rarer event. The above article focuses on the diagnosis and management of a supernumerary tooth, which may be overlooked due to its normal appearance. Given the condition where the identification of supernumerary tooth is difficult, careful observation of the alignment of all the teeth in the region for displacement, rotation, etc, along with measurements, is the key for the diagnosis. Knowledge on the existence of supplemental type of mandibular mesiodens is essential, as an early recognition could permit an interceptive orthodontic approach and allow early correction of arch crowding.
Acknowledgment
The author thanks Dr. Suhas Nayak, and Dr. Reshma VJ, Senior lecturers at Educare institute of dental sciences, Malappuram,Kerala, India for the support.
[1]. G Kökten, H Balcýo lu, M Büyükerten, Supernumerary fourth and fifth molars: a report of two cases.Journal of Contemporary Dental Practice 2003 4:653-65. [Google Scholar]
[2]. EC Stafne, Supernumerary teethDental Cosmos 1932 74:653-659. [Google Scholar]
[3]. RE Primosch, Anterior supernumerary teeth assessment and surgical intervention in childrenPediatr Dent 1981 3:204-15. [Google Scholar]
[4]. MT Garvey, HJ Barry, M Blake, Supernumerary teeth - an overview of classification, diagnosis and management.Journal of the Canadian Dental Association 1999 65:612-16. [Google Scholar]
[5]. T Yokose, T Sakamoto, K Sueishi, K Yatabe, K Tsujino, S Kubo, Two cases with supernumerary teeth in lower incisor regionThe Bulletin of Tokyo Dental College. 2006 47:19-23. [Google Scholar]
[6]. A Cassia, S El-Toum, A Feki, A Megarbane, Five mandibular incisors; an autosomal recessive trait?Br Dent J. 2004 197:307-9. [Google Scholar]
[7]. Y Fukuta, M Totsuka, Y Takeda, H Yamamoto, Supernumerary teeth with eumorphism in the lower incisor region: A report of five cases and a review of theliterature. J Oral Sci 1999 41:199-202. [Google Scholar]
[8]. SY Cho, Six mandibular permanent incisors: report of a caseGen Dent 2006 54:428-30. [Google Scholar]
[9]. V Vikas, G Amit, Sabir Mohd., Supernumerary eumorphic mandibular incisor in association with aggressive periodontitis.J of Indian Society of Periodontology 2010 14:136-38. [Google Scholar]
[10]. M Bhat, Supplemental mandibular central incisorJ Indian Soc Pedod Prev Dent 2006 24:20-3. [Google Scholar]
[11]. KG Deepak, M Sanjeev, G Mona, S Harmesh, Unilateral supplemental primary maxillary lateral incisor without a permanent supernumerary: a rare case report.Indian Journal Oral Sciences 2012 3(1):45-8. [Google Scholar]
[12]. A Sharma, VP Singh, Supernumerary teeth in Indian children. A survey of 300 cases.International Journal of Dentistry 2012 :1-5. [Google Scholar]
[13]. AK Brook, Dental anomalies of number, form and size: their prevalence in British school children.J Int Assoc Dent Child 1974 5:37-53. [Google Scholar]
[14]. SN Bhaskar, Synopsis of oral pathology 1986 USA : MosbySaint Louis [Google Scholar]
[15]. E Piette, H Reychler, Traite de pathologies buccale et maxillofaciale. Bruxelles: De Boeck Universite 1991 [Google Scholar]