The study on fingerprints and skin patterns, referred to as “Dermatoglyphics”, is probably the oldest of all sciences, since it’s importance featured significantly millions of years ago. “Dermatoglyphics”, as defined by Cummins and Midlo [1], refers to the study on the intricate dermal ridge configuration on the skin covering the palmar and plantar surfaces of the hands and feet. Dermal configurations appear at the 12th week of intra-uterine life and they are established by the 24th week. Thereafter, they remain constant, except for the change in their sizes. Dermatoglyphics has been reported to be associated with a number of conditions. One such condition is dental occlusion. This association between Dermatoglyphics and dental occlusion is due to the fact that the development of dentition and the palate occurs during the same period as the development of dermal patterns. Both the dermal patterns and craniofacial constitution are strongly but not exclusively genetically governed structures [2]. Review of literature yielded a few results on relationship of Dermatoglyphics with Dentistry. Most of the studies were conducted to correlate the periodontal diseases and caries [3–6] with Dermatoglyphics. A few other studies have been cited in the literature, which have correlated malocclusions with Dermatoglyphics [7–11]. These studies were either inconclusive or they had not considered all the parameters of Dermatoglyphics. Our present study was a comprehensive study which was done to correlate the total finger and palm patterns with different types of sagittal malocclusions.
Material and Methods
This study was conducted at the Department of Orthodontics and Dentofacial Orthopedics, JSS Dental College and Hospital, Mysore, India and the finger prints were analyzed at the Fingerprint Bureau, Bangalore, Karnataka, India. A convenience sample of 90 south Indian subjects attending the department for treatment of malocclusions, ranging in age from 15-25 years, were divided into 3 groups of 30 each. The control group consisted of 30 subjects who were randomly selected from among the dental students and post graduates who were in the age group of 15-25 years.
Exclusion Criteria
Patients in whom orthodontic treatment was given earlier or those who were undergoing orthodontic treatment.
Patients with syndromic features except malocclusions.
Patients with large coronal restorations or prostheses that could affect the shape and size of the crown.
Patients with a history of trauma or surgical procedures done in the orofacial region.
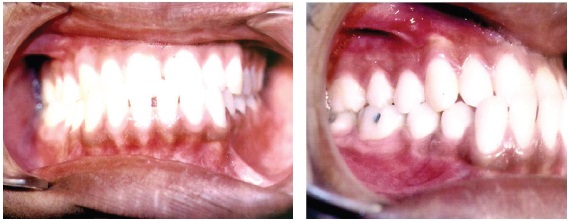
Group 1(control group) Consisted of 30 subjects with normal Angle’s Class I occlusions, an aesthetically pleasing soft tissues profile and an acceptable overjet and overbite. ANB angle of 2- 3 degrees ( Angle formed between point ’A’on maxilla and point ‘B’ on mandible in reference to Nasion ‘N’) [Table/Fig-1a].
Group 2 Thirty subjects with Angle’s Class I malocclusions. ANB angle of 2-3 degrees [Table/Fig-1b].
Group 3 Fifteen subjects each with Angle’s Class II Div. 1 and Class II Div. 2 malocclusions ANB angle of more than 3 degrees [Table/Fig-1c].
Group 4 Twenty subjects with Angle’s Class III malocclusions in which mandibular first permanent molar was full cusp mesial to the maxillary first permanent molar. ANB angle of less than 2 degrees [Table/Fig-1d].


Class II Div 1 malocclusion

Photograph of class I Div 2 malocclusion
The procedures and purpose of the study were explained to all the participants and consent forms were obtained from the participants in the study. Ethical committee clearance was obtained at the institutional level, as the most procedures involved were carried out as a part of diagnostic evaluation in treating the malocclusions and as they did not cause any harm to the participants. Lateral cephalograms of all individuals were taken by using Planmeca 2002 unit (Planmeca, Helsinki, Finland) using standard technique and exposure parameters of 68-70 kilovolts, 12 milliamperes current and an exposure time of 0.8 seconds. A cephalometric evaluation was done on the basis of Steiner’s analysis, Down’s analysis and wits appraisal, applying south Indian norms [12] to determine the craniofacial patterns of the subjects. Study models were made to showcase the dental relationship according to Angle’s classification [13] [Table/Fig-2a, b and c].
Cephalogram of class I skeletal pattern

Cephalogram of class II skeletal pattern

Cephalogram of class III skeletal pattern

Procedure for Obtaining Palm and Finger Prints
The palm and fingerprints of both the hands of the subjects were recorded by the ink and roller method, as was suggested by Cummins and Midlo [14] where quantitative assessment of the ridge pattern could be done. The hands of the subjects were first cleaned with soap and water prior to the recording of palm prints, so as to remove dirt, oily secretions, sweat and they were then dried with a towel. A small amount of ink was dispensed onto the inking slab and it was thoroughly rolled until a thin and even film of pigment covered the entire surface. The subject was made to stand in front of and at fore arm length from the inking plate. The palmar surface of the right hand was placed on the inking slab and it was gently pressed. The completely inked palmar surface was then gently pressed on a clean, white bond paper and it was removed immediately. The same procedure was repeated for the left hand. In taking the rolled impressions of individual fingers, the bulb of the finger was placed at right angles to the surface of the plate. The finger was then rolled or turned until the bulb faced the opposite direction. The finger was then placed on the white paper and it was rolled in the same manner, to obtain a clean, rolled impression of the finger pattern. In case of unsatisfactory prints, the procedure was repeated [Table/Fig-3].
Palmar impression of ridges

The palm and fingerprints of the individuals were studied under the following headings;
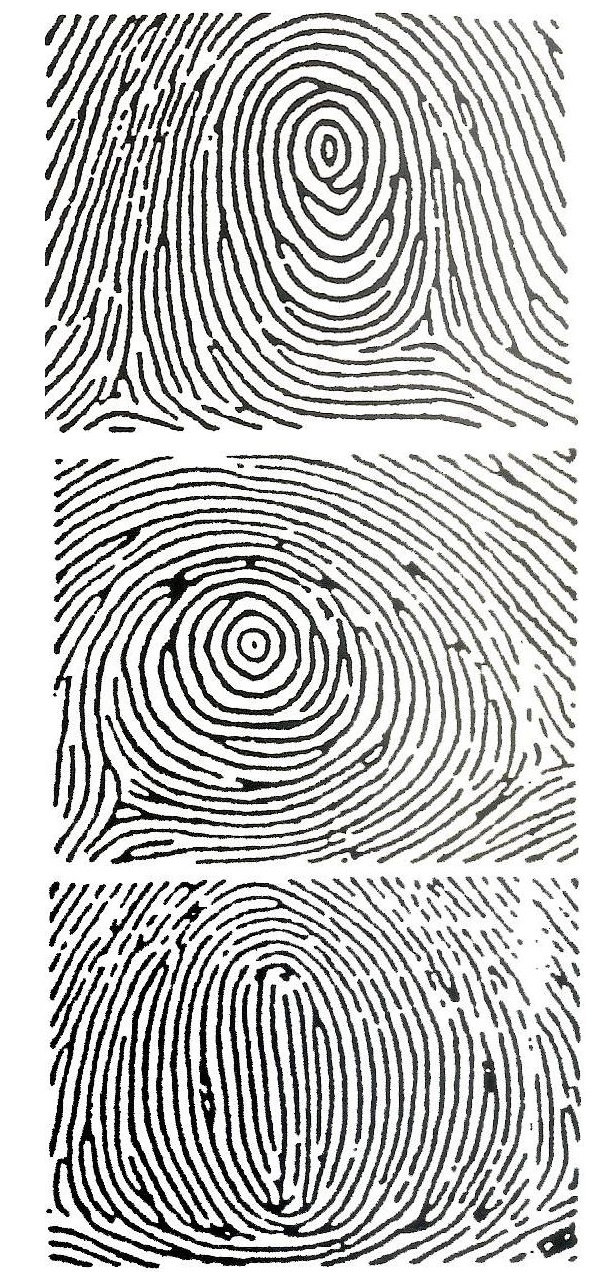
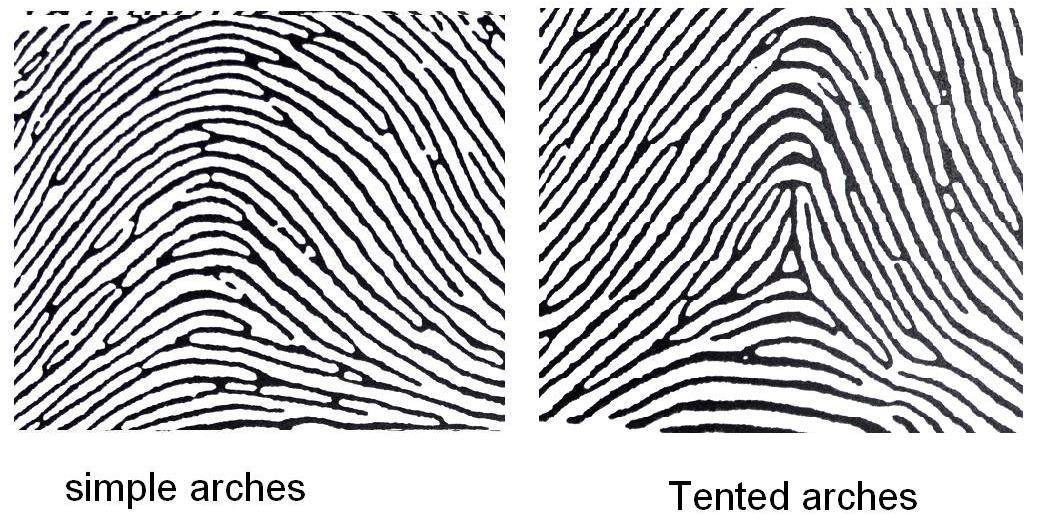
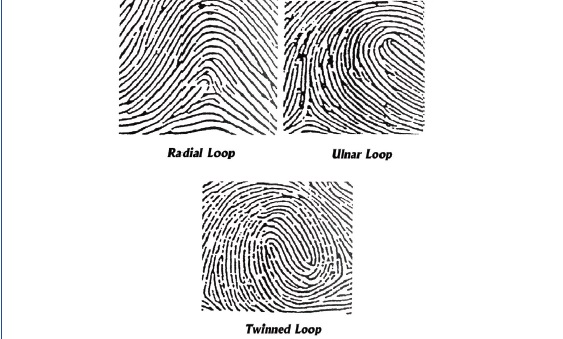
Type of Pattern on the Fingers of both Right and Left Hands
The percentage frequencies of arches, whorls, ulnar loops, radial loops, twined loops and central pocket loops were calculated separately for each of the five digits. The frequency of occurrence was noted separately for right and left hands and finally, combined scores for each of these, were recorded [15] [Table/Fig-4–6].
Total Finger Ridge Count
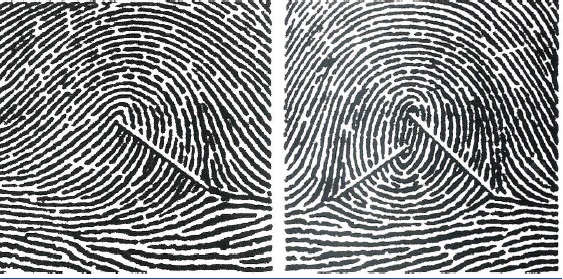
This is indicative of the pattern size. Ridge count is the number of ridges between the triradius and the core or between two triradii (a-b ridge count). Ridge counts for fingertip patterns were done by following the method of Cummins and Midlo [1,14]. The Total Finger Fridge Count (TFRC) represents the sum of the ridge counts of all ten fingers. Only the larger count was used on those digits with more than one ridge count [Table/Fig-7].
Diagrammatic representation of ridge count
Atd Angle of each Hand
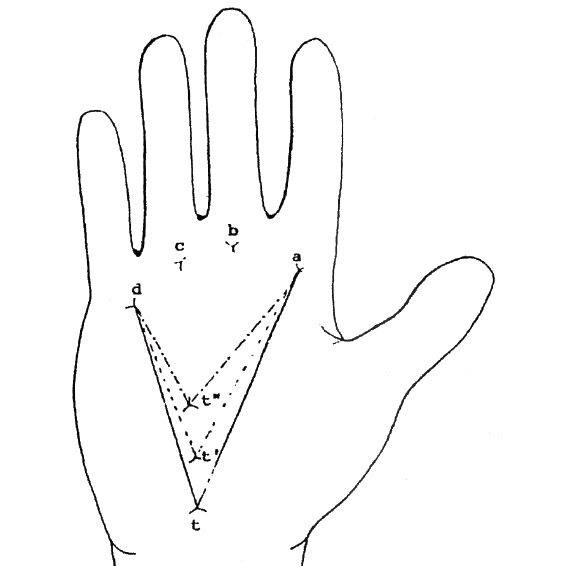
The axial triradius ‘t’ is an important dermatoglyphic landmark on all normally developed hands. This triradius is located near the proximal palmar margin, superficial to the wrist bones, near the axis of the fourth metacarpal bone. The position of this triradius may vary in the proximal distal direction. The normal position of the axial triradius in the proximal region of the palm, near the wrist crease and it is denoted by the symbol “t. The method which is most widely used to interpret the position of axial triradius in the palm is the ‘atd’ angle. This angle is formed by lines drawn from the digital triradius ‘a’ to axial triradius and to ‘d’. The more distal is the position of axial triradius, the larger is the ‘atd’ angle. Palms with patterns in hypothenar area may have more than one axial triradius. In such cases, the widest ‘atd’ angle i.e. the angle from the distal ‘t’ was recorded [Table/Fig-8].
Diagrammatic representation of measurement of angle “atd’
A-B Ridge Count of each Hand
The ridge count in palmar area is frequently obtained for ‘a’ and ‘b’ triradii and it is referred to as the a-b ridge count. It was taken according to the method given by Holt [16].
Results and Observations
The data was entered by using Statistical Software SPSS, version 18 and Microsoft Excel 2007 Software. The values obtained were statistically analyzed using Student’s t-test, ANOVA test for correlating the different parameters of finger print patterns with normal, class I, class II Div 1, class II Div 2 and class III malocclusions. Analysis of the differences between each corresponding pattern among different groups was done by using the Students t-test of significance at a confidence interval of 95%. ANOVA test was carried out for the group comparisons for total finger ridge counts, average a-b ridge count and angle ‘atd’’.
Total Percentage Frequency of Patterns
The percentage frequency of occurrence of different patterns was noted separately for right and left hands and finally, combined scores for each of these were recorded [Table/Fig-9 and 10]. The overall percentage frequency was highest for ulnar loops, ranging from 10-85 on different digits and it was lowest for central pocket loops, ranging from 1-10, which was noted on different digits. The total percentage frequency in ideal cases was lowest in central pocket loops and it was highest in ulnar loops, which was 85 percent. The presence of twinned loops in class II Div 1 and Div 2 on digit 2, which exhibited around 20 and 10 percent frequency, was a significant finding as compared to that in ideal cases, which was zero [Table/Fig-10]. The presence of pocket loops with 10 percent frequency in class II Div 2 group as compared to that in ideal cases, was a notable finding. The absence of radial loops in class III groups- zero percent as compared to that in other groups, was also a noteworthy finding. The left and right discrepancies of findings were more prominent for arches and they were least for ulnar loops and whorls [Table/Fig-9].
Percentage frequency of Different types of Pattern – Arches , whorls and ulnar loops of Class I, Class II Div 1, Class II Div 2 and Class III on right and left hand separately.
| Type of pattern | Group | Hand | Digits |
|---|
| I | II | III | IV | V | Total |
|---|
| Arches | Ideal | Right | 0 | 5.0 ** | 0 | 0 | 0 | 01.0 |
| Left | 0 | 0 | 0 | 0 | 0 | 0 |
| Class I | Right | 25.0 ** | 5.0 | 5.0 | 0 | 5.0 | 8.0 |
| Left | 0 | 0 | 0 | 0 | 0 | 0 |
| Class II.Div 1 | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 10.00** | 0 | 0 | 0 | 10.00 ** | 4.0 |
| Class IIDiv 2 | Right | 5.0 ** | 5.0 ** | 0 | 0 | 0 | 2.0 |
| Left | 5.0 | 10.0 ** | 0 | 5.0 | 0 | 4.0 |
| Class III | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 0 | 0 | 5.0 ** | 0 | 0 | 1.0 |
| Whorl | Ideal | Right | 35.0 | 30.0 | 30.0 | 50.0** | 20.0 | 33.0 |
| Left | 40.0 | 40.0 | 15.0 | 65.0** | 20.0 | 36.0 |
| Class I | Right | 30.0 | 45.0 | 15.0 | 50.0** | 25.0 | 33.0 |
| Left | 40.0 | 50.0 | 35.0 | 40.0 | 40.0 | 41.0 |
| Class II.Div 1 | Right | 50.0 | 30.0 | 10.0 | 60.0** | 30.0 | 36.0 |
| Left | 30.0 | 40.0 | 20.0 | 70.0** | 40.0 | 40.0 |
| Class IIDiv 2 | Right | 40.0 | 40.0 | 40.0 | 60.0** | 30.0 | 42.0 |
| Left | 30.0 | 40.0 | 40.0 | 50.0* | 30.0 | 38.0 |
| Class III | Right | 25.0 | 30.0 | 10.0 | 55.0** | 25.0 | 29.0 |
| Left | 20.0 | 35.0 | 10.0 | 55.0** | 20.0 | 28.0 |
| Ulnar Loops | Ideal | Right | 50.0 | 60.0 | 70.0 | 50.0 | 80.0* | 62.0 |
| Left | 55.0 | 50.0 | 85.0** | 35.0 | 75.0 | 60.0 |
| Class I | Right | 35.0 | 45.0 | 75.0** | 50.0 | 65.0 | 54.0 |
| Left | 50.0 | 40.0 | 60.0 | 55.0 | 60.0 | 53.0 |
| Class II.Div 1 | Right | 50.0 | 40.0 | 90.0** | 40.0 | 70.0 | 58.0 |
| Left | 20.0 | 50.0 | 60.0** | 20.0 | 50.0 | 40.0 |
| Class IIDiv 2 | Right | 60.0 | 65.0 | 85.0** | 45.0 | 75.0 | 66.0 |
| Left | 70.0 | 55.0 | 85.0** | 40.0 | 75.0 | 65.0 |
| Class III | Right | 50.0 | 40.0 | 60.0 | 40.0 | 70.0* | 52.0 |
| Left | 50.0 | 40.0 | 50.0 | 40.0 | 70.0* | 50.0 |
**p<0.05- statistically most; *p<0.01- statistically Significant
Percentage frequency of Different types of Pattern–Radial loops, twinned loops and central pocket loops of Class I, Class II Div 1, Class II Div 2 and Class III on right and left hand separately.
| Type of pattern | Group | Hand | Digits |
|---|
| I | II | III | IV | V | Total |
|---|
| Radial Loops | Ideal | Right | 0 | 5.0** | 0 | 0 | 0 | 1.0 |
| Left | 0 | 10.0** | | 0 | 5.0 | 3.0 |
| Class I | Right | 0 | 5.0** | 0 | 0 | 5.0 | 2.0 |
| Left | 0 | 10.0** | 0 | 0 | 0 | 2.0 |
| Class II.Div 1 | Right | 0 | 10.0** | 0 | 0 | 0 | 2.0 |
| Left | 0 | 10.0** | 0 | 0 | 0 | 2.0 |
| Class IIDiv 2 | Right | 0 | 10.0** | 0 | 0 | 0 | 2.0 |
| Left | 0 | 10.0** | 0 | 10.0** | 0 | 4.0 |
| Class III | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 0 | 0 | 0 | 0 | 0 | 0 |
| Twinned loops | Ideal | Right | 15.0** | 0 | 0 | 0 | 0 | 3.0 |
| Left | 5.0* | 0 | 0 | 0 | 0 | 1.0 |
| Class I | Right | 10.0** | 0 | 5.0 | 0 | 0 | 3.0 |
| Left | 10.0** | 0 | 5.0 | 5.0 | 0 | 4.0 |
| Class II.Div 1 | Right | 0 | 20.0** | 0 | 0 | 0 | 4.0 |
| Left | 40.0** | 0 | 20.0 | 0 | 0 | 12.0 |
| Class II.Div 2 | Right | 10.0** | 10.0** | 0 | 0 | 0 | 4.0 |
| Left | 20.0* | 10.0 | 10.0 | 0 | 0 | 8.0 |
| Class III | Right | 10.0** | 0 | 5.0 | 0 | 0 | 3.0 |
| Left | 5.0** | 0 | 0 | 0 | 0 | 1.0 |
| Central pocket loops | Ideal | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 0 | 0 | 0 | 0 | 0 | 0 |
| Class I | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 0 | 0 | 0 | 0 | 0 | 0 |
| Class II.Div 1 | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 0 | 0 | 0 | 10.0** | 0 | 2.0 |
| Class IIDiv 2 | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 0 | 0 | 0 | 0 | 0 | 0 |
| Class III | Right | 0 | 0 | 0 | 0 | 0 | 0 |
| Left | 0 | 0 | 0 | 0 | 5.0 | 1.0 |
**p<0.05- statistically most; *p<0.01- statistically Significant
Total Finger Ridge Count
The average total finger ridge count in the ideal group was “128.00” (S.D. = 31.21). All the groups showed an increase in this total finger ridge count. However, no statistical significance was attached [Table/Fig-11].
Average Total Finger Ridge Counts of right and left hands NS: Non Significant.
| Groups | Right | Left | Total |
|---|
| Mean | S.D. | Mean | S.D. | Mean | S.D. |
|---|
| Ideal | 64.20 | 16.50 | 63.80 | 16.05 | 128.00 | 31.21 |
| C-I | 75.25 | 19.67 | 74.20 | 20.35 | 149.45 | 39.80 |
| C-II D-1 | 73.80 | 20.36 | 69.90 | 23.10 | 143.70 | 42.63 |
| C-II D-2 | 79.20 | 14.81 | 75.50 | 11.00 | 154.70 | 25.16 |
| C-III | 65.20 | 26.97 | 67.70 | 19.91 | 132.90 | 40.13 |
| F Value | | 1.562 | | 1.087 | | 1.476 |
| P Value | | 193.NS | | .369-NS | | .218-NS |
Atd Angle
The mean “atd” angle was 37.95 ± 3.63 on the right hand and it was 38.15 ± 2.48 on the left hand of the ideal group. All the groups exhibited higher values as compared to those of the ideal cases. The mean “atd” angle increased in all study groups as compared to that in control group and there was no significant difference between right and left hands [Table/Fig-12].
Average atd angle or right and left hands
| Groups | Right | Left |
|---|
| Mean | S.D. | Mean | S.D. |
|---|
| Ideal | 37.95 | 3.63 | 38.15 | 2.48 |
| C-I | 42.40 | 6.73 | 41.93 | 8.05 |
| C-II D-1 | 40.85 | 4.59 | 41.10 | 4.23 |
| C-II D-2 | 39.80 | 3.55 | 41.75 | 4.53 |
| C-III | 42.70 | 7.05 | 40.25 | 5.11 |
| F Value | | 2.350 | | 1.467 |
| P Value | | .062-NS | | .221-NS |
NS: Non–Significant.
A-B ridge count
The mean a-b ridge count increased in all the study groups as compared to that in the control group and there was no significant difference between the right and left hands [Table/Fig-13].
Average a-b ridge count of right and left hands
| Groups | Right | Left |
|---|
| Mean | S.D. | Mean | S.D. |
|---|
| Ideal | 35.40 | 4.67 | 36.95 | 4.93 |
| C-I | 37.00 | 6.16 | 38.00 | 4.76 |
| C-II D-1 | 40.60 | 4.53 | 40.50 | 4.55 |
| C-II D-2 | 36.60 | 3.98 | 37.80 | 2.90 |
| C-III | 38.20 | 5.06 | 38.00 | 3.99 |
| F Value | | 1.961 | | 1.094 |
| P Value | | .109-NS | | .366-NS |
NS: Non–Significant
Discussion
A proper understanding of dermatoglyphics and dental structures in man can only be obtained “with knowledge on their phylogenetic and ontogenetic histories”. It is known that any factor active during the time period of genetic expression, is bound to affect all structures developing at that time. Dermal ridges and craniofacial structures are both formed during second trimester of intra-uterine life, in around 6-8 weeks. It is hypothecated that hereditary and environmental factors leading to malocclusions may also set off peculiarities in fingerprint patterns. Hence, the deviation from normal occlusions due to extraneous factors at the time of development, should also reflect in the dermal patterns. Based on the above background, this study was undertaken to analyze and compare the dermatoglyphic parameters of individuals with normal occlusions and different malocclusions. The justification for dividing our sample into groups, was that each group was representative of a single class of Angle’s classification of malocclusions. Edward H. Angle introduced the most universally used classification in 1899. The basis of Angle’s classification was his hypothesis that the maxillary first permanent molar was the “key to occlusions” [13].
Kanematsu N et al., [2], in his study on finger and palm prints of 311 children with cleft lip, alveolus and palate, observed lower frequency of whorls and higher frequency of ulnar loop patterns in these patients as compared to the findings in normal children. Kharbanda OP et al., [7] conducted a dermatoglyphic evaluation of twenty five north Indian males with true mandibular prognathism and compared this with the dermatoglyphic findings of individuals with Class I occlusions and craniofacial patterns. They concluded that the craniofacial skeletal Class III pattern was associated with Increase in arches and ulnar loops at the expense of whorls on all digits, except digit II. There was increased frequency of whorls and radial loops. An increased frequency of carpel loops on inter digital area of palms was also seen. Our study indicated that decreased frequency of radial loops, twinned loops and central pocket loops was associated with class III malocclusions. No significant increase in arches in class III malocclusions was found in our study, except on 3rd digit. A study which was conducted by Reddy S Prabhakar A R and Reddy VVS by using dermatoglyphics9 to predict and compare Class I, Class II Div. 1, Div. 2 and Class III malocclusions, revealed that the craniofacial Class II Div1, Class II Div 2 patterns were associated with an increased frequency of arches and ulnar loops and a decreased frequency of whorls. In the present study, there was a significant increase in whorls in class II div I cases, prominently on digit IV in Class III malocclusions. There was an increased frequency of arches and radial loops, with a decreased frequency of ulnar loops. In predicting Class III malocclusions, based on the frequency of arches, the sensitivity values were found to be higher and more reliable than the senstivity values of Class II Div. 1 and Div. 2 malocclusions. M Trehan et al., [10] analyzed and compared the dermatoglyphic parameters of individuals with normal occlusions and various classes of malocclusions. The dermatoglyphic findings revealed that as compared to normal occlusions, Class I and Class III malocclusions were associated with an increased frequency of whorls. Both Class I and Class II Div. 1 malocclusions were associated with an increased frequency of radical loops and arches. In our study also, arches were found at a higher frequency percentage in class I and class II div I malocclusions, which was in accordance with those which were seen in the previous study. This was found to be statistically significant. However, no significant increase in whorls was noted in class III malocclusions in the present study. The previous study was conducted on north Indian population, whereas our sample was derived from the south Indian population. This difference in findings may be attributed to environmental influences. A study which was conducted by Tikare S, Rajesh G and Prasad K W [11] concluded that there was a statistical association between whorl patterns and class 1 and 2 malocclusions (p<0.05). However, no overall statistical association was observed between fingerprint patterns and malocclusions (p>0.05). The present study also noted a significant increase in whorls in class II malocclusions.
Conclusion
Thus, based on our study, it can be concluded that different malocclusions are more prone to have a specific type of ridge pattern. Some of the findings were statistically significant. However, the parameters on the palm exhibited no curious finding as compared to fingers in our study. Though malocclusions based on dermatoglyphics can be predicted with a fair degree of accuracy, it cannot be relied upon as the sole factor. This is due to the fact that numerous other factors such as ethnic and racial variations, congenital, environmental and other local factors can also influence the development of malocclusions. Since an extensive study on ridge patterns was undertaken with several groups, our sample size was restricted. Further studies on each of these groups on large sample sizes, according to their racial and ethnic backgrounds, are warranted.