Ponticulus Posticus means “little posterior bridge” in Latin. It is defined as an abnormal small bony bridge which is formed between the posterior portion of the superior articular process and the posterolateral portion of the superior margin of the posterior arch of the atlas [1]. This bony bridge has been called by different names, such as sagittale foramen, atlantal posterior foramen, arcuate foramen, a variant of Kimmerle’s anomaly (Kimmerle, 1930), upper retro-articular foramen, canalis vertebralis, retro-articular vertebral artery ring, retro-articular canal and retrocondilar vertebral artery ring. However, its most accepted name is ’ponticulus posticus’ [1–3].
Its prevalence has been reported to be between 5.14- 37.83% in the Western population. However, no significant difference in prevalence between men and women has been suggested. Previously, authors had studied about this foramen and had mentioned its occurrence in 9.8–25.9% of the general population [4]. Taitz C had mentioned about the presence of partial posterior bridging of atlas in 25.9% and of its complete bridging in 7.9% of the population. This condition had not been a matter of concern for spine surgeons until its surgical significance in the insertion of screws into the lateral mass of the atlas was recently reported. Some spine surgeons have recently reported that it could cause a severe complication such as a vertebral artery injury during insertion of C1 lateral mass screws. At times, the sulcus is bridged by an anomalous ossification and a posterior ponticulus; a lateral ponticulus is occasionally formed. It forms the arcuate foramen that contains the vertebral artery and the suboccipital nerve. It can be a possible cause of posterior circulation ischaemia and cervicogenic headache [1,4,5]. The potential clinical significance of ponticulus posticus is that a majority of patients with this finding are symptomatic. Some studies have determined that patients with ponticulus posticus have no greater chance of experiencing adverse effects from cervical adjustments which are related to the presence of a posticulus posticus. However, symptoms that may be associated with ponticulus posticus include migraine, vertigo, diplopia, shoulder pain, neck pain, which may be caused by the compression of vertebral artery as it passes from the foramen transversum of the Ist cervical vertebra to the foramen magnum of skull [5–7].
Radiographically, Miki et al., have classified ponticulus posticus into three types:
The present study intended to investigate the prevalence of Ponticulus Posticus (PP) in symptomatic and asymptomatic patients of Gulbarga population, to substantiate as to whether ponticulus posticus was the possible cause of chronic tension-type headaches and migraine.
Material and Methods
A sample of 500 patients was selected from the patients in the age group of 5-70 years, who visited the Department of Oral Medicine and Radiology and the study was approved by ethical clearance committee of Al-Badar Rural Dental College and Hospital, Karnataka, India. To the best of our knowledge, this is the first study which has been done in the Karnataka region, India. All the patients who were willing to participate in this study and were ready to undergo radiographic examinations, who were in the age group of 5-70 years, were included in the study. Patients with congenital anomalies (cleft lip and palate, syndromes of craniofacial region and any history of trauma in cervical spine region) were excluded from the study. Written consents were obtained from all the patients and in case of minors, consents were obtained from their parents. All the patients were subjected to digital lateral cephalography done by using Kodak 8000C digital panoramic and lateral cephalometric system. The images were viewed on a flat screen Compaq TFT-LCD monitor with a resolution of 2906 x 2304 pixels in JPEG format with a 24- bit grayscale. Each radiograph was scrutinized for the presence and absence of PP and it was further evaluated for both the partial and complete forms. Images with poor visualization of the posterior arch of atlas due to overlapping of mastoid process or occiput, were excluded. Inter-examiner views of three staff members from the same department (Oral Medicine and Radiology ) were taken. The duration of the study was eight months, from April 2012–November 2012. Patients with either partial or complete form were further studied for symptoms like orofacial pain, headache and diagnosed migraine. In statistical analysis, mean standard deviation and percentage was calculated for all the groups. To test the significance between variables, Chi-square test was done. For the entire test, a p-value of 0.05 was taken as statistically significant.
Results
Out of 500 cases, 266 (53%) were males and 234 (47%) were females. In the study, partial PP was found in 302 patients (60%) among which 158 (52%) were females and 144 (48%) were males. Both variants were found in the age group of 16-45 years, with a mean age of 28 years and SD 27.76 ±10.74 [Table/Fig-1]. In our study, we found two types of bony rings i.e. partial form [Table/Fig-2] and complete form of ponticulus posticus [Table/Fig-3]. A complete variant was observed in 40 (8%) patients, among which 26 (65%) were males and 14 (35%) were females. In 158 (31%) cases, neither a partial nor a complete form of PP was observed. [Table/Fig-4]. In partial PP, 42 patients (14%) were found to be symptomatic. Among these 42 patients, 17 (40%) were males and 25 (60%) were females [Table/Fig-5], whereas in patients with complete form of PP, 32 patients (76%) were found to be symptomatic. Among these 32 patients, 15 (49%) were males and 17 (51%) were females, which showed that the symptoms were almost equally present in both the genders, with a negligible difference in both the variants of PP with a p value of >0.05, which was not significant [Table/Fig-6]. Symptoms were mainly in the form of migraine or tension type headache.
Simple Bar Diagram presenting different forms of Ponticulus Posticus. Absent, Partial & Complete. (No of cases 500)

Partial form of ponticulus posticus which forms an incomplete bony ring

Complete type of ponticulus posticus in which complete bony ring is seen

Multiple Bar Diagrams representing Age wise distribution of different forms of Ponticulus Posticus. (No of 500)

Sex wise comparison in symptomatic and asymptomatic patients in Partial Form of ponticulus posticus.( No of cases 302)

Sex wise comparisons in symptomatic and asymptomatic patients in complete Form of ponticulus posticus. (No of cases 40)

Discussion
Ponticulus posticus is increasingly being observed an important anomaly of the atlas, as the use of lateral mass screws for the fixation of the atlas has become common for the treatment of atlantoaxial instability. However, it can sometimes be a difficult procedure, as the region contains venous plexuses as well as the greater occipital nerve. To avoid these difficulties, some surgeons have recommended that, in the presence of a broad posterior arch of the atlas, the insertion of the screw be started in the dorsal aspect of the posterior arch instead of at the base of the lateral mass, or at the junction of the posterior arch and the lateral mass. A broad dorsal arch of the atlas is the best indication for this modified screw trajectory. However, in patients with ponticulus posticus and resulting arcuate foramen carrying vertebral artery, it can be mistaken for a broad dorsal arch and the surgeon may insert the screw into the ponticulus posticus. This can result in an injury to the vertebral artery, and it can also lead to stroke or even death by thrombosis, embolism, or arterial dissection. In the western population, the prevalence of ponticulus posticus has been reported to be between 5.1-37.8% [1]. It was much less than our study, which may be related to the geographic or ethnic variations involved between the populations.
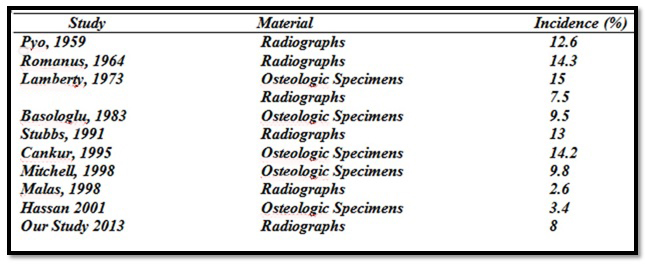
Our study found a slightly higher prevalence of complete form of PP [8%] as compared to that which has been described in the literature. Incidence of Complete Arcuate Foramen, as reported in the Literature, has been given in [Table/Fig-7] [7].
Incidence of complete ponticulus posticus as reported from 1959-2013
Multiple pathological processes related to the presence of the Ponticulus ponticus (Wight et al., Cakmak et al.,) have been reported. Previous studies have suggested that it may be a product of a congenital development (Allen, 1879; Cleland, 1960; von Torklus et al.,) for eg. a genetic trait (Selby et al.,1955), an ossification caused by age (Pyo and Lowman, Epstein, Breathnach, White and Panjabi, 1978), or that it may be the result of external mechanical factors (Taitz and Nathan) [2].
Studies have proposed that the hypothesis of external mechanical factors, such as carrying heavy objects on head, could play a role in the development of these bony bridges. A study which was carried out by Paraskevas G mentioned about the incidence of complete canal for vertebral artery in labourers to the non labourers [8]. But in our study, patients’ occupations were not taken into consideration. Paraskevas G also mentioned that there was a higher occurrence of partial PP in the 5-44 years of age group [7]. But we found a higher incidence in the age group of 16-45 years.
Although the possibility that the calcification of the bony bridge progresses over time was described by Paraskevas G et al., [8], in our study, we found a clear relationship with age, since only 10 cases of children under 15 years of age with partial ossification of the canal were found and none of the cases in this age group had the complete form of ponticulus posticus. Rest of the cases were in the age group of 16-45 years, which suggested that the incidence of these bony rings clearly increased with age.
In our study, we found that complete foramen was significantly more common in males i.e. [65%] than in females [35%] and that partial foramen was common in females i.e. [52%] than in males [48%]. In this aspect, our results corroborated with those of the study carried out by Stubbs DM in 1992. In his study on arcuate foramen, a variability in distribution related to different races and sexes was seen [9].
Taitz and Nathan studied 672 atlas vertebras, among which 25.9% had partial posterior bridges and 7.9% had complete bony bridges. They found that partial bony bridges predominated in younger age groups (10 to 30 years) and that complete bony bridges wee common in the older age groups (30 to 80 years) [10]. This differed from our findings in that both partial and complete bony bridges had higher prevalences among the age groups of 16-45 years and we had found only 10 cases with partial form among patients who were less than 15 years of age and 9 cases with partial form in the age group of 40-60. None of the cases in this age group presented with complete form of PP.
Michell J, in her study on lateral bridges of the atlas, suggested that the foramen was lower in whites than in blacks [11]. However, our study was conducted in Gulbarga population and it was not compared with studies done on any other group of population.
A study was carried out by Ephrosyni Koutsouraki et al., to substantiate Kimmerle’s anomaly as the possible cause of chronic tension-type headaches and neurosensory-type hearing loss, in a patient with a known history of headaches and accompanied unilateral hearing loss. The headaches demonstrated the characteristics of the chronic tension-type headaches. The audiometric investigation concluded the hearing loss to be of the neurosensory type, whereas, the imaging examinations revealed the existence of a partial osseous bridge, that is an incomplete arcuate foramen on the upper surface of atlas. Both the clinical and the radiological findings of this case were indicative of a possible connection between Kimmerle’s anomaly and the manifestation of chronic tension-type headaches and neurosensory-type hearing loss [12]. However, in contradiction to above mentioned study in which they found symptoms only in patients with partial or incomplete forms of PP, in our study, we found that patients with both the forms of ponticulus posticus had symptoms of tension type headache and migraine in the age group of 16-45 years. In our symptomatic group, out of 42 patients who had partial form of PP, 25 were females and 17 were males, while among 31 patients with complete form of ponticulus posticus, 15 were males and 16 were females. This substantiated that among those who had partial form of PP, females showed higher rate of symptoms, while among those with complete form of PP, males had slightly dominated the scene. Our results also indicated that chances of symptoms being present with complete ponticulus posticus were more than in partial form.
Rosalia Leonardi et al., carried out an investigation to determine the prevalence of atlanto-occipital ligament calcification on lateral X-rays of Nevoid Basal Cell Carcinoma Syndrome (NBCCS) patients, aiming to assess the effectiveness of this sign in diagnosis of NBCCS. Here, the patients affected by NBCCS showed an increased prevalence of atlantooccipital ligament calcification than was found in the general population. Although further studies are required to clarify this issue, the calcification of the atlanto-occipital ligament should be considered in addition to the other major criteria for diagnosis of NBCCS [13]. To the best of our knowledge, the presence of atlanto-occipital ligament calcification in patients affected by NBCCS has never been reported.
Association of Ponticulus Posticus with Barre-Lieou syndrome, has also been reported. It represents symptoms of headache, retro-orbital pain, vasomotor disturbance of the face and recurrent disturbances of vision, swallowing and phonation caused by alteration of blood flow within the vertebra. Therefore, foramen arcuate is a potential clinical/surgical significant anatomical variant of the atlas [14]. However, in our study, we never came across any patient who showed these symptoms. The limitation of this study was that the occupation of the patients was not noted and sample size and duration of the study could have been increased.
Conclusion
According to the results of our study, complete form of PP can be considered as a possible cause of chronic tension type of headaches or migraine. Although in our sample size, patients with partial form of PP also complained of vague type of headache, statistical values were not significant to make any comment. However, the fact remains that at least few of our patients with partial form of PP had presented with symptoms. Hence, it will not be wrong to say that any patient with presence of PP of any variant can have atypical type of headaches and hence, presence of such anomalies should be considered as differential diagnosis of chronic orofacial pain. Thus, care must be taken to account for it on lateral cephalograms of orthodontic patients. If any such anomaly is detected or suspected, it must be documented in the patient’s health record and a specialist consultation must be sought. A CT scan can be used to substantiate the size and morphology of the ponticulus, if it is required. Although orthodontists or radiologists are not directly concerned with the management of cervical spine anomalies, they do have an obligation, as healthcare professionals, to take any such findings that may hold importance for the patient, to their logical conclusion, but only if they know the significance, can patients be referred to the best concerned specialist.