Ossicular Injury Caused by A Knitting Needle
Amritpal Singh1, Maninder Kaur2
1 Associate Professor, Radio-diagnosis, Sri Guru Ram Das Institute of Medical Sciences and Research, Amritsar, Punjab, India.
2 Assistant Professor, Microbiology , Sri Guru Ram Das Institute of Medical Sciences and Research, Amritsar, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amritpal Singh, 45-Kashmir Avenue, Amritsar, punjab-143001, India.
Phone: 9815545233,
E-mail: singhbunny1975@gmail.com
Ossicular chain injury is a complication of trauma caused to temporal bone, but rarely, it can also occur due to direct trauma caused to ossicular chain by a penetrating injury. Patients usually suffering from conductive hearing loss and vertigo, although a facial nerve injury is also a possibility. We are describing here a case of young male who presented with a penetrating trauma to the left ear, caused by a metallic knitting needle, that resulted in ossicular chain disruption. The patient suffered from severe vertigo and conductive hearing loss. He was advised complete bed rest and vertin for controlling vertigo, after which he recovered. Computed tomography is the investigation of choice for detecting and characterizing such injuries, for proper management of patients. Penetrating middle ear trauma differs from blunt trauma, as the mechanism of injury is distinct. The injury is usually isolated and an urgent repair may be needed. Hearing results after an immediate or a delayed ossiculoplasty are apparently satisfying, although late cases are assumed to be associated with adhesions or fibrosis.
Ossicular chain injury, Trauma, Computed tomography
Case Report
Ossicular injuries usually occur in association with fractures of the temporal bone, with longitudinal fractures being more commonly associated than transverse fractures. Dislocations of the ossicular chain can also occur without fractures, either due to a penetrating injury or blunt trauma. We are presenting here a case of an ossicular injury which was caused by a metallic knitting needle, when the patient had made an attempt to clean his external ear canal.
A young male presented to E.N.T Department with severe vertigo and conductive hearing loss. Patient’s symptoms started soon after he was trying to clean his ear with a metallic knitting needle and he injured his ear drum. Patient was sent to Radiology Department for a high resolution CT scan of the temporal bone.
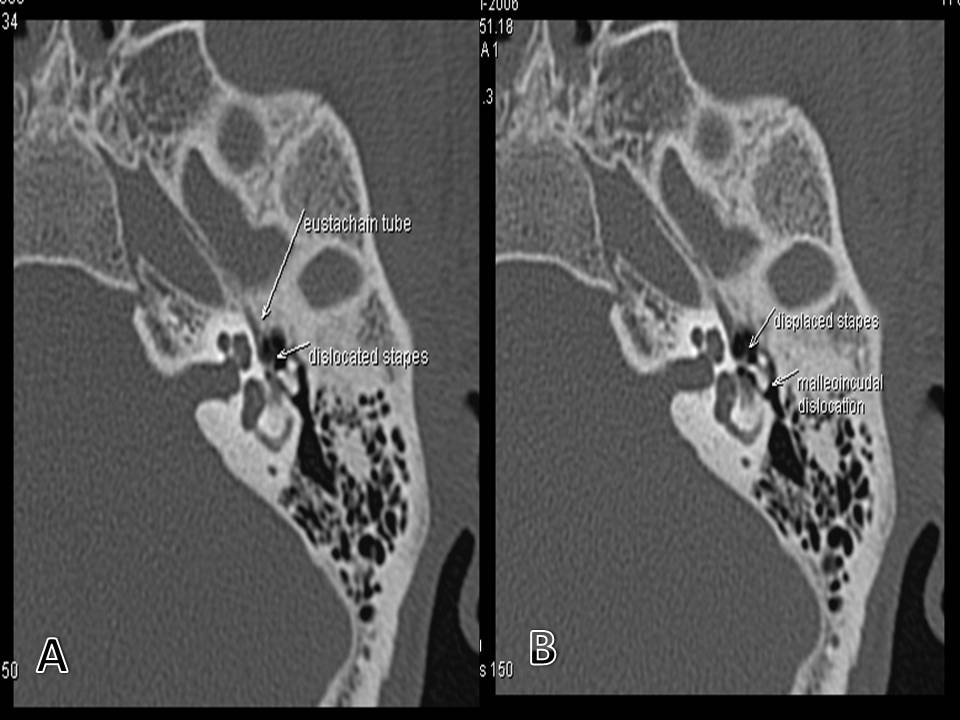
High resolution CT scan revealed a stapediovestibular dislocation with anteriorly displaced stapes foot plate, abutting the opening of eustachian tube (external rotation), along with a malleoincudal dislocation. Although dislocation of stapes can be associated with perilymph fistulas, however, no fluid was seen in the tympanic cavity in this case. Still, a diagnosis of a stapediovestibular and a malleoincudal dislocation associated with perilymph fistula was given, due to complaint of vertigo. To the best of our knowledge, the dislocation of ossicular chain by direct trauma caused by a knitting needle after an ear drum perforation is a rare entity. Patient was given complete bed rest and vertin (betahistdine) for controlling vertigo, after which he recovered.
Discussion
Ossicular injury caused by a metallic knitting needle is very rare, while trauma caused to temporal bone, with or without fractures, is still the main cause of an ossicular injury. Ossicular injury that usually occurs is a dislocation, of which there are five types:
Incudostapedial joint separation
Incudomalleolar joint separation
Dislocation of the incus,
Dislocation of the malleoincudal complex and
A stapediovestibular dislocation.
Fractures of the ossicles are very rare. High resolution computed tomography is investigation of choice for evaluation of ossicular injuries [1–4]. For evaluating ossicular injuries, radiologist should have a thorough knowledge on ossicular anatomy and he/she should be aware of pitfalls [5,2].
(A) shows dislocated left stapes which is dislocated from the oval window & displaced anteriorly & abutting the opening of the eustachian tube along with abnormal angulation b/w malleus & incus. (B) shows dislocated left Incudomalleolar joint
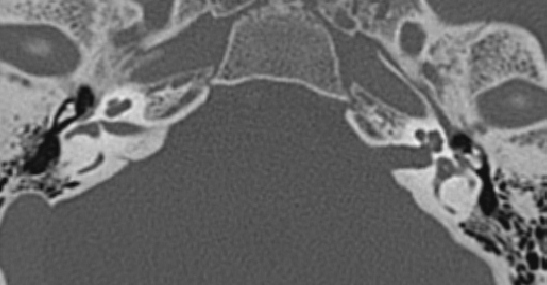
Shows normal icecream-cone configuration of malleus & incus on right side with loss of normal icecream-cone configuration on left side
There are few salient features of the ossicular anatomy which have to be kept in mind. The malleus is well supported by the anterior, lateral and superior mallear ligaments and stapes are supported by annular ligaments, stapes tendon and articulation with incus. The incus which is the heaviest (25 mg) of all ossicles is provided with least support and so, it is most prone to injury.
Malleoincudal complex is seen in epitympanic recess, with a complex resembling ice-cream cone appearance on axial images, with scoop of the ice-cream being the head of malleus and cone being the body and short process of incus. This joint is best seen on axial images, which provides excellent information on incudostapedial joint [1,3].
Axial images provide excellent information about the incudostapedial joint [6]. The head of stapes and lenticular process of incus are seen as separated by a thin incudostapedial joint. Head, crura and foot plates of stapes are also very well seen on thin overlapping axial views. Coronal views through oval window show position of crura inside oval window [1,5,2].
Stapediovestibular dislocations are uncommon, but they are mostly caused by penetrating injuries caused by cotton tipped applicators. There are two types of dislocations i.e. internal dislocation –when stapes is dislocated from oval window and is depressed into the vestibule and external dislocation-when dislocated stapes is located in the tympanic cavity [7,2].
Disruption of the stapediovestibular joint may also cause perilymph fistulas. Imaging diagnosis of perilymph fistulas is very difficult, but it can be suggested in presence of labyrinth fractures, stapes fracture/dislocations /nonvisualization of stapes/unexplained middle ear effusions or pneumolabyrinths [8].
An incudostapedial dislocation is diagnosed as an abnormal cleft between the head of stapes and the long process of the incus and it is best appreciated on axial scans [5].
An incudomalleolar dislocation is seen on axial scans as displacement of head of malleus from the body and short process of the incus. Coronal scans are helpful for detecting minor lateral displacements [2,3].
Dislocation of the incus is associated with separation of the malleoincudal and incudostapedial joints.
A malleoincudal complex dislocation occurs when this joint provides resistance to traumatic forces and when the complex moves into the lower part of the tympanic cavity. This displacement can be outwards, inwards and downwards. It can be associated with an incudostapedial dislocation. Axial and oblique coronals are helpful [2].
This is a brief description of the dislocations of the ossicles, which mostly occur due to trauma caused to temporal bone, but they can also occur without direct trauma being caused to temporal bone, as was demonstrated in our case. Two similar cases of ossicular disruptions caused by penetrating injuries were reported by Neuenschwander MC et al., [9]. The injuries in their cases were caused by cotton tipped swabs and wooden matchsticks. To reduce the associated morbidities, the injuries should be promptly diagnosed. High resolution CT scan of the temporal bone is best for diagnosing them. Importance of CT was also documented by Sertec Y et al., in their study. They also documented that patients with persistent hearing loss should be advised occuloplasty, as results are apparently satisfying in immediate or delayed occuloplasty, although late cases are assumed to be associated with adhesions or fibrosis [4]. So, we should be familiar with this entity, to reach a correct diagnosis and thus improving patient care. Penetrating middle ear trauma differs from blunt trauma, as the mechanism of injury is distinct. The injury is usually isolated and an urgent repair may be needed [9]. We should also discourage people from cleaning their ear canals with keys, pens, hairpins and last but not the least, knitting needles.
[1]. Lourenco MTC, Yeakly JW, Ghorayeb BY, The Y sign of lateral dislocation of incusAm J Otol 1995 16:387-92. [Google Scholar]
[2]. Phillpe M, Francis V, Jean FG, CT appearances of ossicular injuriesRadiographics 1997 17:1445-54. [Google Scholar]
[3]. Zayas JO, Feliciano YZ, Hadley CR, Temporal bone trauma and the role of multidetector CT in the emergency departmentRadiographics 2011 Oct 31(6):1741-55. [Google Scholar]
[4]. Sertac Y, Yusuf H, Hakan B, Traumatic ossicular dislocations: Etiology and ManagementAm J Otolaryngol 2008 Jan 29(1):31-36. [Google Scholar]
[5]. Hasso AN, Ledington JA, Traumatic injuries of the temporal boneOtolaryngol Clin North Am 1988 21:295-316. [Google Scholar]
[6]. Swartz JD, Swartz NG, Korsvik H, Computerised tomographic evaluation of the middle ear & mastoid for post traumatic hearing lossAnn Otol Rhinol laryngol 1985 94:263-66. [Google Scholar]
[7]. Herman P, Guichard JP, Vanden Abbeele T, Traumatic luxation of stapes evidenced by High resolution CTAJNR 1996 17:1242-44. [Google Scholar]
[8]. Weissman JL, Curtin HD, Pneumolabyrinth: A computed tomographic sign of temporal bone fractureAm J Otolaryngol 1992 13:113-14. [Google Scholar]
[9]. Neuenschwander MC, Deutsch ES, Cornetta A, enetrating middle ear trauma: a report of 2 casesEar Nose Throat J 2005 Jan 84(1):32-5. [Google Scholar]