Carcinoma Stomach: Unwanted Chemotherapeutic Success: A Case Vignette
Sapam Opendro Singh1, Sumit Sudhir Hadgaonkar1, Khwairakpam Amitkumar Singh2, Adithya GK2, T.Y.Babu Singh2
1 Assistant Professor, Department of General Surgery, RIMS, Lamphelpat,Imphal, Manipur, India.
2 Post Graduate Trainee, Department of General Surgery, RIMS, Lamphelpat,Imphal, Manipur, India.
3 Post Graduate Trainee, Department of General Surgery, RIMS, Lamphelpat,Imphal, Manipur, India.
4 Post Graduate Trainee, Department of General Surgery, RIMS, Lamphelpat,Imphal, Manipur, India.
5 Professor, Department of General Surgery, RIMS, Lamphelpat,Imphal, Manipur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sumit Sudhir Hadgaonkar, Post Graduate Trainee, Department of General Surgery, RIMS, Lamphelpat,Imphal, Manipur, India.
Phone: 8974685042,
E-mail: sumya33@gmail.com
A 45-years-old male, chronic smoker and occasional alcoholic, from Tamenlong district of Manipur was admitted to the department of Surgery, RIMS, Imphal on 19th August, 2011. He was diagnosed as a case of poorly differentiated adenocarcinoma of the stomach located at incissura along the lesser curvature. CT scan of abdomen had revealed para-aortic, aorto-caval and celiac lymphadenopathy. Patient had undergone 5 cycles of neo-adjuvant chemotherapy consisting of 3 weekly course of Oxaloplatin 80mg(D1) + epirubicin 200mg (D1) + Capicitabine 2000mg(D1-D14). After 1 month of chemotherapy, patient then underwent subtotal gastrectomy (modified D2 resection) without any significant peri-operative complication. Surprisingly, the final histopathological report of the resected specimen didnx’t reveal any evidence of malignancy in any sections. Role of chemotherapy in gastric cancers has been an adjunct to surgery and the optimal drugs regimen has not been elucidated so far. Till now, very few cases of carcinoma stomach which show pathological complete response have been reported. Our case is such a rare case of pathological complete response following neoadjuvant chemotherapy.
Adenocarcinoma, Neo-adjuvant chemotherapy, Subtotal gastrectomy, Pathological Complete Response
Case Report
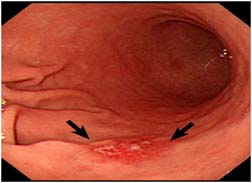
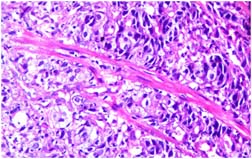
A 45-year-old male presented with sensation of fullness after meals with vomiting since 4 months and anorexia with weight loss since 2 months. Patient was chronic smoker since 25 years and occasionally consumed alcohol.Upper gastrointestinal endoscopy (UGIE) revealed an ulcer at incissura on lesser curvature [Table/Fig-1]. Biopsy reported as poorly differentiated adenocarcinoma [Table/Fig-2]. Ultrasound whole abdomen reported retroperitoneal lymphadenopathy with urinary bladder sludge. Contrast enhanced CT scan (CECT) whole abdomen showed multiple rounded and discrete hypo dense lymph nodes in para aortic, aorto-caval, precaval celiac trunk and gastro hepaticligaments.
Ulcer over lesser curvature (black arrows)
Poorly differentiated adenocarcinoma seen on endoscopic biopsy of the lesion
Patient was given 5 cycles of neo adjuvant chemotherapy (NACT) consisting of Oxaloplatin, epirubicin and Capicitabine (EOX regimen). The regimen included Oxaliplatin 80mg (D1) + Epirubicin 200mg (D1) + Capicitabine 1000mg BD (D1-D14), 3 weekly. There were no adverse effects of chemotherapy reported.
Post NACT all routine blood tests, CECT whole abdomen, barium meal study, chest X-ray, were normal. PET-CT was not done.
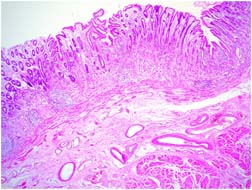
After NACT patient was posted for surgery. Subtotal gastrectomy with Bilroth II anastomosis with modified D2 dissection was done. Final histopathological report of the resected specimen showed well preserved gastric mucosa with moderate lymphoplasmocytic cell infiltrate in lamina propria ,few areas showing a few mucosal glands with focal intestinal metaplasia ,no evidence of malignancy seen [Table/Fig-3]. All dissected lymph nodes showing reactive lymphadenitis without any evidence of malignancy until last follow up patient was not showing any signs of local recurrence.
Mucosa over lesser curvature showing no evidence of malignancy
Discussion
Gastric cancer is the fourth most commonly diagnosed cancer and is the second leading cause of cancer death worldwide [1]. Although survival of patients with gastric cancer after surgery has been improved by early detection and curative surgery, the prognosis of patients with highly advanced gastric cancer is usually very poor [2]. The majority of patients presenting with resectable gastric adenocarcinoma will have locally advanced disease [defined as the penetration ofthe subserosa by the primary tumour (T3), regional nodalinvolvement (N+), or both] for which the chance of cure with surgery alone is poor [3].
Chemotherapy is the treatment of choice for metastatic advanced gastric cancer; however, a standard treatment regimen has not been established. Neoadjuvant chemotherapy for advanced gastric cancer with or without distant metastasis has been reported [4].However pathological complete response rate is still lower than 8%. Anticipated benefits of Neoadjuvant chemotherapy are increase in likelihood of curative resection by downstaging tumour, elimination of micrometastases, improvement of tumour related symptoms, increased overall survival [5].
From endoscopic biopsy which showed poorly differentiated adenocarcinoma and CT scan whole abdomen showing celiac and gastrohepatic node enlargement; locally advanced gastric carcinoma was confirmed in our case. Patient was subjected to EOX regimen of chemotherapy which is widely used for metastatic and advanced gastric cancers.An interim analysis presented at ASCO 2003 reported an interesting response rate of 52% for EOX regimen compared with 31% for ECF, 33% for EOF and 35% for ECX [6].
After 5 cycles of EOX regimen of neoadjuvant chemotherapy, CT whole abdomen and barium meal post chemotherapy were normal. When patient was fit for surgery radical subtotal gastrectomy with modified D2 dissection was done with Bilroth II anastomosis. Aim of surgical resection was to confirm complete response by pathological examination and to provide therapeutic effects of resection if residual cancer cells were present.
Pathologic complete response was defined as fibrosis or fibro-inflammation within an entirely submitted and evaluated gross lesion without microscopic evidence of carcinoma, and histologically negative nodes [4].
Pathological complete response was observed in our case following surgery with no evidence of malignancy in resected stomach specimen and presence of reactive lymphadenitis in all lymph nodes.
Pathological complete response has been reported in metastatic gastric cancers also with incurable factors such as peritoneal dissemination, hepatic metastases [7]. Thus, Can neoadjuvant chemotherapy become the sole cure for locally advanced carcinoma stomach thus avoiding complications of major surgical procedures? Large multicentric randomized trials are needed.
Conclusion
Combination neoadjuvant chemotherapy with EOX regimen showed marked efficacy in treatment with pathological complete response in a case of locally advanced carcinoma stomach.
[1]. Ajani JA, Evolving Chemotherapy for Advanced Gastric CancerThe Oncologist 2005 10(suppl 3):49-58. [Google Scholar]
[2]. Park JM, Chi KC, Unresectable gastric cancer with gastric outlet obstruction and distant metastasis responding to intraperitoneal and folfox chemotherapy after palliative laparoscopic gastrojejunostomy: report of a caseWorld J. Surg. Oncol 2010 8:109 [Google Scholar]
[3]. Yonemura Y, Neoadjuvant treatment of gastric cancer with peritoneal disseminationEur J Surg Oncol 2006 32:661-65. [Google Scholar]
[4]. Fields RC, Recurrence and survival after pathological complete response to preoperative therapy followed by surgery for gastric or gastro oesophagealadenocarcinomaBritish Journal of Cancer 2011 104:1840-47. [Google Scholar]
[5]. Neoadjuvant Approaches for Gastric Cancer12th Annual Western CanadianGastrointestinal Cancer Consensus Conference Sept 17,2010 [Google Scholar]
[6]. Sumpter KA, Randomised, multicentre phase study comparing capecitabine with fluorouracil and Oxaloplatin with cisplatin in patients with advanced oesophagogastric cancer: Confirmation of Dose escalationProc Am Soc Clin Oncol 2003 2:257 [Google Scholar]
[7]. Chakrabandhu B, Complete Response of liver metastatic gastric cancer after FOLFOX-4 chemotherapy regimen followed by salvage gastrectomy: A case reportInternational Journal of Medicine and Medical Sciences Dec 2012 VOL 2(12):278-283. [Google Scholar]