Familial Facial disfigurement in Multiple Familial Trichoepithelioma
Usha Kataria1, Deepti Agarwal2, Dinesh Chhillar3
1 Assistant Professor, Department of Dermatology & Veneral Disease, BPS Govt. Medical College for Women, Khanpur Kalan, Sonepat, Haryana, India.
2 Associate Professor, Department of Pathology, BPS Govt. Medical College for Women, Khanpur Kalan, Sonepat, Haryana, India.
3 Demonstrator, Department of Microbiology, BPS Govt. Medical College for Women, Khanpur Kalan, Sonepat, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepti Agarwal, Associate Professor, BPS Govt. Medical College for Women, Khanpur Kalan, Sonepat, Haryana, India.
Phone: 91-8607566555,
E-mail: deeptiagarwal@rocketmail.com
Trichoepithelioma is an uncommon, benign hamartomatous tumor of the pilosebaceous follicle. Presenting as multiple papules and nodules on face and neck, they pose a significant cosmetic problem in affected individuals. Familial involvement of this dermatosis occurs in an autosomal dominant pattern, the locus being located on chromosome 9p21, which causes multiple facial lesions in family members and their kins. Here, we report a case of multiple familial trichoepithelioma causing considerable disfigurement of the face.
Benign hamartomatous tumor, Pilosebaceous follicle, Locus 9p21, Trichoepithelioma
Case Report
A 35-year-old female patient presented to the skin out-patient department with a history of multiple skin coloured elevated lesions on the face. These papules started to first appear in the childhood and increased in size and number during her adolescence. The lesions were intermittently pruritic and developed slight tenderness after scratching. There was history of similar lesions in her elder brother and her son. A few lesions had started appearing in her daughter who was presently a teenager. The patient denied a family history of any other cutaneous disorder or neoplasms. The patient had been otherwise healthy without any other medical problems, medications or any systemic complains.
General examination revealed moderate built, average nourishment levels and vital signs. On local dermatological examination there were numerous skin coloured, dome shaped papules, present mainly on the face, nose, cheeks and forehead [Table/Fig-1].
Pattern of spread of papular lesions on face,
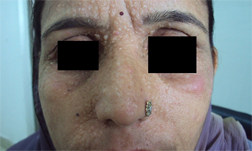
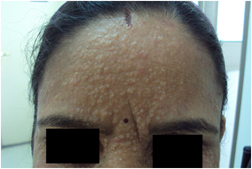
The papules were variable in size, averaging 1-3mm in diameter, of fibroelastic consistency and without any loci of pus. Some of the papules had developed redness, probably due to inflammation following scratching in the itchy areas [Table/Fig-2]. The scalp, neck, trunk, buttocks and extremities were unaffected. Skin appendages were normal.
Papular lesions on forehead with an average size of 1-3mm,
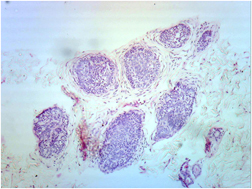
A skin biopsy from the forehead lesion was taken under local anaesthesia and sent for histopathological examination. It revealed nest of small basaloid cells with peripheral pallisading around eosinophilic centre containing amorphous material. These nests are surrounded by fibroblastic tissue [Table/Fig-3]. Microbiological examination of the excised tissue in the region of inflammation was sterile and ruled out any infective etiology.
Nest of small basaloid cells with peripheral pallisading and surrounding fibroblastic tissue
Other routine lab investigations were within normal limits. On the basis of personal and family history, clinical examination, and the histopathology the case was diagnosed as multiple familial trichoepithelioma. The management plan was decided and the patient was kept in regular follow-up to evaluate the results of conservative therapy.
Discussion
Trichoepitheliomas are benign hamartoma of the pilosebaceous follicle, composed of immature islands of basaloid cells. However the name trichoepithelioma is preferred because it indicates that the differentiation of this tumor is directed towards hair structure. They usually appear in childhood or early adolescence and involve limited areas of the body, most commonly the face, scalp or neck and less often the trunk [1,2].
Three types of trichoepitheliomas are known; solitary, multiple and the desmoplastic variety. Multiple hereditary trichoepitheliomas were first described by Brooke and Fordyce in 1892 and are also known as epithelioma adenoids cysticum [3]. When presenting as a lone cutaneous finding, it is called Trichoepithelioma Papulosum Multiplex. Alternatively, they may be associated with other cutaneous findings such as cylindromas, spiradenomas, and milia, also known as Brooke-Spiegler syndrome [4].
Multiple trichoepithelioma occurs in an autosomal dominant inherited genodermatosis, known as multiple familial trichoepithelioma. The annual incidence in US has reported to be between 2.14-2.7 cases per year; with a strong predilection for females [5]. Even though both sexes receive normal genes in an autosomal dominant pattern, lessened chromosomal penetrance theory could support the reason for higher occurrence in females. The gene has been localized on chromosome 9p21 [6]. However, this loss of heterozygosity on chromosome 9p21 is not seen in solitary trichoepithelioma. In addition to this, recent reports have found mutation in cylindromatosis tumor suppressor gene (CYLD), which maps to chromosome 16q12-q13 in most of cases [6]. Mutation in the gene regulating proliferation and differentiation of stem cells of pilosebaceous-apocrine unit could also give rise to combination of adnexal tumours.
Differential diagnosis of trichoepithelioma is basal cell carcinoma, syringoma, eccrine poroma, eccrine nevus, commedonal nevus and other appendeceal tumours. On histopathological examination, presence of horn cysts and tumour islands of basaloid cells are the two major characteristic components of multiple trichoepithelioma. Horn cysts consist of fully keratinized centre surrounded by basophilic cells. These cells lack atypia and mitosis. The keratinization is abrupt and complete as opposed to horn pearls seen in squamous cell carcinoma. The tumour islands of basaloid cells show peripheral palisading with surrounding fibrous stroma. These fibroblasts lack artifactual retraction which is typical of basal cell carcinoma [7].
Treatment of multiple trichoepithelioma relies on variety of ablative techniques like cryotherapy, dermabrasion, electrodissection and radiation therapy with variable results. Apart from treatment failure, literature also suggests the occurrence of facial scarring and further disfigurement following these procedures. Recently, isolated case reports have shown efficacy of high energy pulsed CO2 laser with no recurrence or any noticeable side effect in treating trichoepitheliomas during 12 months follow up, though future trials or case series need to establish the overall safety and efficacy of this therapeutic tool[8].
Conclusion
Multiple trichoepithelioma of familial origin present a significant cosmetic, social and psychological impairment in females due to their presenting age, sex and involvement of exposed areas i.e. head and neck, an aggressive or invasive treatment should only be reserved for limited lesions that are overtly enlarged or a cause of significant disfigurement of face. With the passage of time as most of lesions of multiple trichoepithelioma subside, a wait and watch strategy along with assurance is a more advisable strategy, instead of aggressive ablation techniques.
[1]. Mathur M, Kedia SK, Multiple familial trichoepitheliomaJournal of College of Medical Sciences. Nepal 2010 6(4):64-8. [Google Scholar]
[2]. Bozi E, Katoulis AC. Multiple familial trichoepitheliomas. Orphanet encyclopedia. Apr 2004. 1-3.http://www.orpha.net/datya/patho/GB/uk [Google Scholar]
[3]. Kaur T, Puri1 KJPS, Chahal KS, Budhwar J, Multiple Familial TrichoepitheliomasA case report and review Dec 2012 8(2)(1):1-5. [Google Scholar]
[4]. Patrocinio LG, Damasceno GP, Patrocinio TG, Patrocinio JA, Solitary nasal TrichoepitheliomaRev Bras Otorrinolaringol 2008 74(4):637 [Google Scholar]
[5]. Yiltok SJ, Echejoh SJ, Mohammad AM, Ituen Am, Multiple familial trichoepithelioma, case report and review of literatureNigerian Journal of Clinical Practice Jun 2010 13(2):230-2. [Google Scholar]
[6]. Harada H, Hashimoto K, Ko MS, The gene for multiple trichoepithelioma maps chromosome 9p21J Invest Dermatol 1996 107(1):41-3. [Google Scholar]
[7]. Lee KH, Kim JE, Cho BK, Kim YC, Park CJ, Malignant Transformation of Multiple Familial Trichoepithelioma: Case Report and Literature ReviewActa Derm Venereol 2008 88:43-6. [Google Scholar]
[8]. Ning CC, Sheu HM, Chen YC, Chao SC, Successful treatment of linear trichoepithelioma with CO2 laserDermatol Sinica 2001 19:221-4. [Google Scholar]