A Case of Heterotopic Pregnancy with Tubal Rupture
Shraddha K Shetty1, Anil K Shetty2
1 Assistant Professor, Department of Obstetrics and Gynaecology, Kasturba Medical College, Mangalore, Karnataka, India.
2 Associate Professor, Department of Paediatrics, Father Muller Medical College, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shraddha Shetty K, Assistant Professor, Department of Obstetrics and Gynaecology, Kasturba Medical College, Mangalore, Karnataka, India.
Phone: 09886792043,
E-mail: shraddha_k1@rediffmail.com
Heterotopic Pregnancy (HP) is the simultaneous development of an intra-uterine pregnancy and ectopic pregnancy. In natural cycle, it is a very rare event. With the increasing popularity of ovulation induction performed during assisted reproductive techniques, its incidence has significantly increased. However, diagnosis is often delayed because of its rarity and difficulty. Heterotopic pregnancy is an important differential diagnosis to consider in patients with intra-uterine pregnancies presenting with acute abdominal pain and hemoperitoneum. Here we are reporting a case of heterotopic pregnancy in a 26-year-old woman presented with symptoms and signs of ruptured tubal pregnancy with live intra-uterine gestation at 8 weeks of amenorrhea.
Extra–uterine, Heterotopic, Intra-uterine, Rupture, Tubal
Case 1
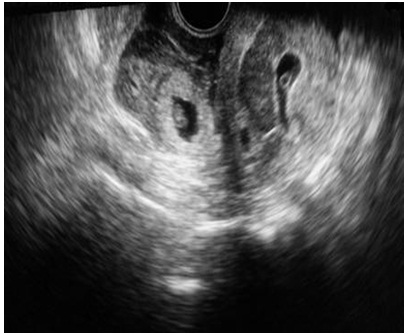
A 26–year–old primigravida presented to the outpatient unit of Lady Goschen Hospital with history of severe abdominal pain of twelve hours duration and bleeding per vagina for one hour. The patient had amenorrhea of eight weeks duration. On examining the patient, she had pallor, tachycardia and a blood pressure of 90/60 mmHg. Abdominal examination revealed diffuse abdominal tenderness and guarding. Transvaginal ultrasound examination revealed the presence of viable intra-uterine pregnancy of eight weeks duration and right sided adnexal mass. There was free fluid in the cul -de-sac suggestive of hemoperitoneum [Table/Fig-1]. Based on these finding a diagnosis of a viable intra-uterine and a ruptured ectopic pregnancy were made. Emergency laparotomy was performed. Intraoperative, there was ruptured right sided tubal pregnancy with hemoperitoneum. Right sided salpingectomy was done. Histopathology confirmed the diagnosis of ectopic pregnancy. Post–operatively patient was given two units of blood transfusion and a repeat ultrasound scan done after two weeks confirmed the viable intra-uterine pregnancy. She was put on progesterone for four weeks. The pregnancy was continued till term. She delivered a healthy female baby following a spontaneous vaginal delivery. Postnatal period was also uneventful [Table/Fig-2].
Ultrasound showing heterotopic pregnancy
Right sided ruptured ectopic

Discussion
Heterotopic pregnancy is a rare entity occurring in 1:30000 pregnancies but its incidence rises as a result of assisted reproductive techniques (ART) to 1:100-1:500 [1].
The incidence of heterotopic/ectopic pregnancy has risen in recent years also due to increased incidence of pelvic inflammatory disease. Most heterotopic/ectopic pregnancies are localized in the fallopian tube and usually it is diagnosed when symptoms develop [2].
There may be an increased risk in patients with previous tubal surgeries [3].
Heterotopic pregnancy can occur in the absence of any predisposing risk factors, and the detection of intra-uterine pregnancy does not exclude the possibility of the simultaneous existence of ectopic pregnancy. Transvaginal ultrasound and assessment of the whole pelvis, even in the presence of intra-uterine pregnancy, can be an important aid in the diagnosis of heterotopic pregnancy [4].
Majority of the reported heterotopic pregnancies are of singleton intra-uterine pregnancies. Triplet and quadruplet heterotopic pregnancies have also been reported, though extremely rare [5]. Intra-uterine gestation with hemorrhagic corpus luteum can simulate heterotopic/ectopic gestation both clinically and on ultrasound [6].
Its treatment is a challenge as serial beta-hCG is not useful in diagnosis or follow-up and medical management with methotrexate is contraindicated with an intra-uterine pregnancy. Heterotopic pregnancies in select cases can be managed expectantly with strict monitoring and serial ultrasounds and the viable intra-uterine pregnancy can be saved [7].
Laparoscopy or laparotomy with minimal manipulation of the uterus should be the standard form of treatment in these patients. Heterotopic pregnancy is possible with natural conception and the survival of the intra-uterine fetus is feasible [8].
Conclusion
Knowledge of the occurrence of heterotopic pregnancy and early transvaginal scan will definitely help in making the diagnosis of HP and thereby reducing the incidence of this fatal condition.
[1]. Michał M, Marian M, Marek M, Ewa WO, Heterotopic pregnancy in the absence of risk factors-diagnostics difficultiesGinekol Pol 2011 Nov 82(11):866-68. [Google Scholar]
[2]. Simsek T, Dogan A, Simsek M, Pestereli E, Heterotopic triplet pregnancy (twin tubal) in a natural cycle with tubal rupture: case report and review of the literatureJ Obstet Gynaecol Res 2008 Aug 34(4 Pt 2):759-62. [Google Scholar]
[3]. Gruber I, Lahodny J, Illmensee K, Losch A, Heterotopic pregnancy: Report of three casesWien KlinWochenschr 2002 114:229-32. [Google Scholar]
[4]. Ljuca D, Hudic I, Hadzimehmedovic A, Acta Clin Croat 2011 Jun 50(2):249-52. [Google Scholar]
[5]. Alsunaidi MI, An unexpected spontaneous triplet heterotopic pregnancySaudi Med J 2005 26:136-38. [Google Scholar]
[6]. Sohail S, Hemorrhagic corpus luteum mimicking heterotopic pregnancyJ Coll Physicians Surg Pak 2005 15:180-81. [Google Scholar]
[7]. Kriplani A, Lunkad AS, Sharma M, Ammini AC, Recurrent ectopic pregnancy with heterotopic pregnancy in a patient of hypo gonadotropic hypogonadism: a case reportJ Reprod Med 2011 May-Jun 56(5-6):274-76. [Google Scholar]
[8]. Varras M, Akrivis C, Hadjopoulos G, Antonion N, Heterotopic pregnancy in natural conception cycle presenting with tubal rupture: a case report and review of literatureEur J Obstet Gynecol Reprod Biol 2003 (106):79-82. [Google Scholar]