Systemic Sclerosis Presenting with Simultaneous Retinal Vasculitis in One Eye and Optic Neuritis in the other along with Severe Immune Haemolytic Anaemia
Avijit Moulick1, Biswanath Sharma Sarkar2, Anirban Jana3, Pradipta Guha4, Anjan Das5
1 Assistant Professor, Department of Medicine, Calcutta National Medical College, 24 Gorachand Road, Kolkata-700014, India.
2 Assistant Professor, Department of Medicine, Calcutta National Medical College, 24 Gorachand Road, Kolkata-700014, India.
3 Senior Resident, Department of Medicine, Calcutta National Medical College, 24 Gorachand Road, Kolkata-700014, India.
4 Assistant Professor, Department of Medicine, Calcutta National Medical College, 24 Gorachand Road, Kolkata-700014, India.
5 Associate Professor, Department of Pathology, Calcutta National Medical College, 24 Gorachand Road, Kolkata-700014, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Avijit Moulick, Flat 2F, Spandan Apartment. 1/14 Extn Chittaranjan Colony. Kolkata–700032, West Bengal, India.
Phone: 9333656161,
E-mail: dramoulick@gmail.com
Systemic Sclerosis (SSc) is a connective tissue disorder which involves multiple systems in a chronic progressive manner. Micro–angiopathic haemolytic anaemia is a distinguished feature of “scleroderma renal crisis”, which is manifested by severe hypertension, a rapidly progressing renal dysfunction and hyperreninaemia and is seen in patients with an early, diffuse form of the disease. A nervous system involvement is rare, though entrapment neuropathies have been reported. Who presented with a sequential loss of vision in both eyes; due to retinal vasculitis in right eye and optic nerve demyelination in the left eye. She also had severe Coombs’ negative haemolytic anaemia in absence of any renal dysfunction or hypertension. Both the ophthalmologic and the haematologic manifestations are very rare and both responded well to oral prednisolone therapy.
Systemic sclerosis, Retinal vasculitis, Optic neuritis, Autoimmune haemolytic anaemia
Case Report
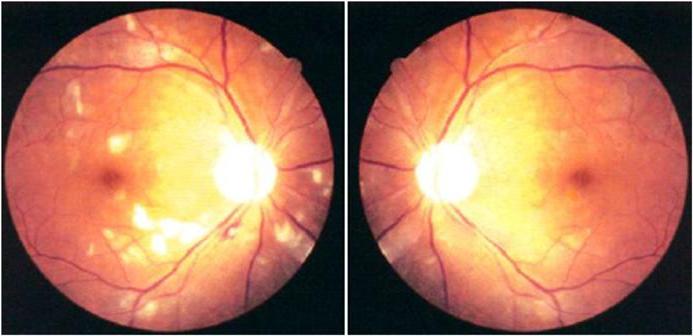
A 40-year–old housewife presented with dimness of vision in both eyes, which she had for 10 days. Dimness of vision started in the right eye, it progressed over two to three days and it then affected her left eye acutely. It was painless and there was no history of red eye, fever, trauma or toxin exposure. She attended eye OPD of a medical college hospital. Her vision was 6/24 in right eye and finger counting at one foot in left eye. Intra-ocular pressure was normal. The anterior chamber was clear. Ophthalmoscopy revealed evidence of retinal vasculitis in her right eye, which was manifested by superficial retinal haemorrhages, cotton wool spots, retinal venous dilatation; and an altered macular reflex in left eye [Table/Fig-1]. A cranial CT (Computed Tomography) scan did not reveal any abnormality. DFA (Digital Fluorescent Angiography) revealed features suggestive of retinal vasculitis …. in right eye and a normal angiogram of left eye. VEP (Visual Evoked Potential) showed features of optic nerve demyelination on left side, which was suggested by a prolonged P100 latency with a normal pattern on right side.
Ophthalmoscopy revealed evidence of retinal vasculitis in her right eye manifested by superficial retinal hemorrhages, cotton wools spot, and retinal venous dilatation
She also complained of a progressive generalized weakness and fatigue over the same period and was referred to medical OPD for evaluation. She had no joint pain or swelling, dysphagia, chest pain, cough, fever or overt blood loss. There was no history of Raynaud’s phenomenon. She had regular menstrual bleeding, with an average duration of three days and a normal flow. There was no significant past illness. She was married and was living with her husband and two sons. She had no history of abortions.
On examination, she was found to have severe pallor and mild jaundice but no lymphadenopathy or hepatosplenomegaly. Her blood pressure was 122/78 mmHg (right arm supine). There was a thick patch of skin below her right eye which she had not noticed earlier [Table/Fig-2]. The cardiac and respiratory system examinations were normal and nervous system did not have any abnormality apart from dimness of vision. Her initial investigation reports are tabulated in [Table/Fig-3].
Thick patch of skin below her right eye

Initial Investigation reports
| Parameter | Values |
|---|
| Hb (g/dl) | 6.1 |
| RBC (mil/cmm) | 2.0 |
| WBC (/cmm) | 16000 |
| DLC | N85L10M1E4B0 |
| Platelet (/cmm) | 280000 |
| PCV(%) | 19 |
| MCV (fl) | 95 |
| MCH (pg) | 30.5 |
| MCHC(%) | 32.1 |
| ESR(mm in 1st hour) | 118 |
| Reticulocyte (%) | 10 |
| Peripheral smear | Normoblasts |
| LDH (125-243 u/l) | 1580 |
| Haptoglobulin(30-200 mg/dl) | <7.56 |
| Postprandial blood glucose (mg/dl) | 101 |
| Bilirubin (mg/dl) | 5.0 |
| Unconjugated bilirubin (mg/dl) | 4.2 |
| ALT / AST (u/l) | 12/22 |
| Alkaline phosphatase(<112 u/l) | 90 |
| Total protein (g/dl) | 6.4 |
| Albumin/globulin (g/dl) | 4.4/2.0 |
| Prothrombin time (C 11sec) | 11.3sec |
| Urea/Creatinine (mg/dl) | 22/0.8 |
| Uric acid (mg/dl) | 5.8 |
| Na/ K (meq/l) | 138/4.1 |
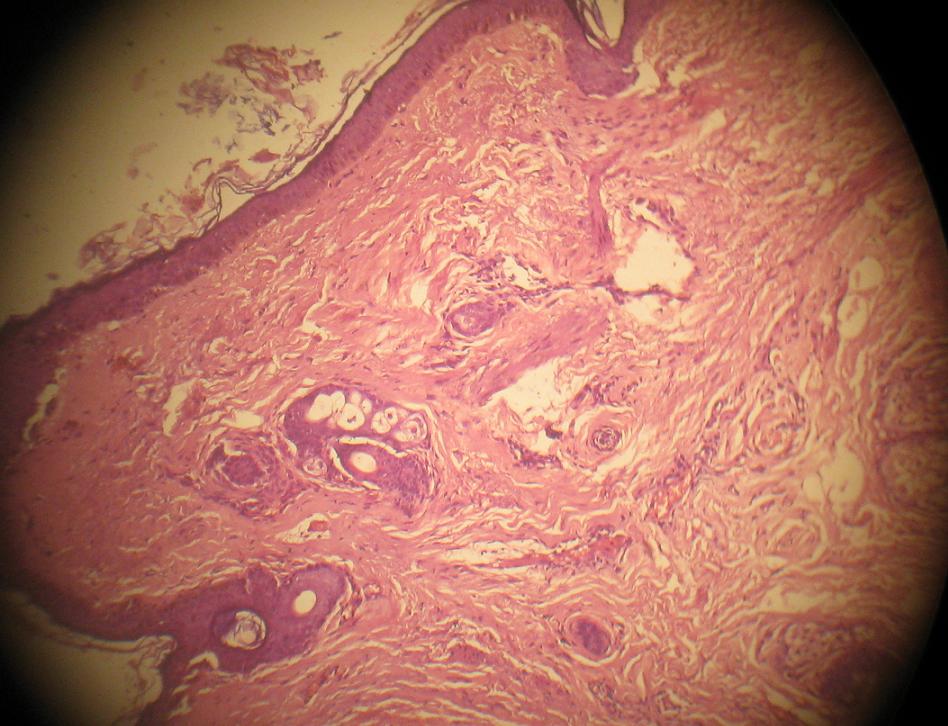
Serum fT4 was 1.5 ng/dl; TSH was 2.88 micro IU/ml. ASO titre and Rheumatoid factor were negative. Urine RE did not reveal any abnormality and urine was negative for bile salts and bile pigments. Blood G-6PD level was 10.2 u/g Hb. Direct agglutination test (Coombs) was negative. Malarial Antigen was negative for both Pl. vivax and Pl. falciparum. Abdominal ultrasound revealed no significant abnormality. X-ray chest was normal. Bone marrow aspiration study did not suggest any pathology. Anti-nuclear antibody was positive on immunofluorescence studies, with a titre of 1:160, with a specled pattern. Anti-ds DNA was negative. Anti-phospholipid antibodies were negative. Anti-centromere antibody was positive. Anti-topoisomerase antibody was negative. pANCA and cANCA were negative. Flow cytometry done for detection of Paroxysmal Nocturnal Haemoglobinuria (PNH) was negative with CD55 -ve RBC 1.59%; CD59 -ve RBC 1.74% (Ref <3%). A CT angiography of cerebral vessels did not reveal any narrowing. A skin biopsy obtained from the thickened area under the right eye showed features of scleroderma, which were manifested by an attenuated epidermis with absence of reti ridges, marked sub-epidermal fibrosis and presence of adnexal structures within dermis (HE stain, 4X) [Table/Fig-4]. A final diagnosis of “limited cutaneous systemic sclerosis with right sided retinal vasculitis, along with left sided demyelinating optic neuropathy and severe Coomb’s negative haemolytic anaemia” was made.
Skin biopsy (HE stain, 4X) shows attenuated epidermis with absence of reti ridges, marked sub-epidermal fibrosis and presence of adnexal structures within epidermis
The patient was put on low dose (1mg/kg body weight) oral prednisolone and folate. Haemolytic anaemia responded well to therapy and her vision improved to 6/12 in both eyes. After 6 weeks, her Hb was 12.4 g/dl; WBCs were 12600/cmm; DLC- N84 L12 M2 E2 B0; Platelets were adequate and there were normocytic normochromic red cells in peripheral blood smear. LDH was 470 u/l(230-460).
Discussion
Systemic sclerosis is a multi-systemic disorder which affects musculoskeletal., gastrointestinal, renal and cardiopulmonary systems [1]. Two sub-types have been described according to pattern of skin involvement as well as laboratory features: limited cutaneous and diffuse cutaneous, with the former slowly involving the skin of distal extremities and face and the latter diffusely affecting the skin of extremities, face and trunk and various organs progressively. Most of the patients with limited type present with long standing Raynaud’s phenomenon and a visceral involvement is insidious. It may lately manifest as pulmonary hypertension [1,2].
It primarily affects the women of childbearing ages. Several genetic and environmental factors have been implicated and the pathogenesis is characterized by vascular injuries, autoimmunity and ultimately, a progressive visceral and vascular fibrosis [1]. Systemic sclerosis usually does not involve the central nervous system, but entrapment neuropathy may be seen [1,3]. Several isolated case reports have demonstrated that vasculitis of the Central Nervous System (CNS) may occur in absence of the relatively common vasculopathy which is associated with renal crisis and severe hypertension [4]. Acute visual loss is an extremely rare condition in systemic sclerosis and autoimmune vasculopathy has been variably attributed as the mechanism behind it [5]. Rarer is the occurrence of optic neuritis in this disorder [6]. Our patient developed sequential loss of vision in both her eyes over a short period, with features of retinal vasculitis in the right eye, as evidenced by characteristic funduscopy and DFA and optic neuritis in the left eye, which was suggested by an abnormal VEP. Normal CT of brain, including orbit and CT angiography of the cerebral vessels, suggested absence of any narrowing that could explain the visual loss. Moreover, there was no evidence of systemic vasculopthy, renal involvement or hypertension. Association of ANCA in vasculitis which is associated with systemic sclerosis is a rare finding and it needs further studies to evaluate its significance, though both c and p ANCA were not detected in this case [7]. Both the eyes achieved a significant improvement of visual acuity over a period of four months of systemic low dose prednisolone therapy.
Mild anaemia of chronic inflammation is common in systemic sclerosis and iron deficiency anaemia as well as megaloblastic anaemia can also develop [8]. Microangiopathic haemolytic anaemia which is caused by fragmentation of RBCs passing through microvessels is a characteristic finding in renal crisis seen in scleroderma [2]. Autoimmune haemolytic anaemia is a rare manifestation in systemic sclerosis and it has been described in several case records [9]. Our patient had severe Coombs’ negative autoimmune haemolytic anaemia without evidence of any renal disorder or hypertension. Anaemia responded very well to systemic corticosteroid therapy and her haemoglobin rose to normal level within three months of taking the therapy. G6PD deficiency and PNH were excluded by appropriate studies. The unique feature of this patient was that bilateral visual loss was caused by two separate and rare pathologies and that one was followed by the other in quick succession. Moreover, the eye manifestation was shortly followed by another rare haematologic disorder and the clinical evidence of limited cutaneous systemic sclerosis was only a thick patch of skin on the cheek. Therefore, physicians should be aware of such an initial manifestation of SSc in absence of florid clinical features of SSc.
Conclusion
Systemic sclerosis is a multi-system disorder that affects several systems in a progressive manner. Rare ophthalmologic and haematologic manifestations can occur in absence of overt dermatologic manifestations that are classic features for making its diagnosis. These disorders responded very well to immunosuppressive (prednisolone) therapy unlike most of the progressive features of the disease.
[1]. Varga John, Systemic Sclerosis (Scleroderma) and Related DisordersIn: Harrison’s Principles of Internal Medicine 2012 Vol II18th edMcGraw-Hill:2757(Longo DL, Kasper DL, Jameson JL et al, eds) [Google Scholar]
[2]. Varga John, Systemic Sclerosis (Scleroderma) and Related DisordersIn: Harrison’s Principles of Internal Medicine 2012 Vol II18th edMcGraw-Hill:2767(Longo DL, Kasper DL, Jameson JL et al, eds) [Google Scholar]
[3]. Varga John, Denton Christopher P, Systemic Sclerosis and the Scleroderma-Spectrum DisordersIn: Kelly’s Textbook of Rheumatology 2009 Vol II8th edSaunders Elsevier:1328-38.(Firestein GS, Budd RC, Harris ED et al, eds) [Google Scholar]
[4]. Gordon RM, Silverstein A, Neurologic manifestations in progressive systemic sclerosisArch Neurol 1970 22:126-33. [Google Scholar]
[5]. Weng-Nga Lao, Man-Lung Yip, Andrew Kui-Man Wong, A Scleroderma Patient with Sudden Loss of Vision in Both Eyes- Case ReportHong Kong Bull Rheum Dis 2008 8:27-32. [Google Scholar]
[6]. Boschi A, Syners B, Lambert M, Bilateral optic neuropathy associated with the crest variant of sclerodermaEur J Ophthalmol 1993 3:219-22. [Google Scholar]
[7]. Liang Kimberly P, Michet Clement J, ANCA-associated vasculitis in scleroderma: a case series of fourteen patientsRheumatology Reports 2011 3(e2):3-8. [Google Scholar]
[8]. Westerman Maxwell P, Martinez Ramon C, Medsger Thomas A, Totten Robert S, Rodnan Gerald P, Anemia and Scleroderma-Frequency, Causes, and Marrow FindingsArch Intern Med 1968 122(1):39-42. [Google Scholar]
[9]. Katsumata Kazuaki, A case of systemic sclerosis complicated by autoimmune hemolytic anemiaModern Rheumatology 2006 16(3):191-95. [Google Scholar]