Accessory Superficial Ulnar Artery: A Case Report
Shweta Solan1
1 Assistant Professor, Department of Anatomy, Kallinga Institute of Medical Sciences, Patia, Bhubaneswar, Orissa, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shweta Solan, Assistant Professor, Department of Anatomy, Kallinga Institute of Medical Sciences, Patia, Bhubaneswar, Orissa, India.
Phone: 09178050207
Variations in the arterial system of the upper limb have been well documented. A thorough knowledge on variations of arteries of upper extremity is necessary during performance of vascular and reconstructive surgeries and also, during evaluation of angiographic images. A case of accessory superficial ulnar artery was reported. The ulnar artery had a high origin from the brachial artery, in the upper third of the arm and it proceeded superficially and lateral to ulnar nerve in forearm, but it had a normal termination in the hand. The brachial artery had a usual course in the arm, but in the cubital fossa, it divided into the radial and deep ulnar arteries. This deep ulnar artery ended by dividing into ulnar recurrent and common interosseous arteries. Knowledge on this variation is important for the radiologists, orthopaedic and plastic surgeons, for appropriate planning of operative procedures involving the arteries of the upper limb.
Ulnar artery, Brachial artery, Common interosseous artery, Upper limb
Introduction
High incidence of variations in the arterial patterns in the upper limb have been the subjects of many anatomical studies. Incidence of major arterial pattern variations, as high as 18.53%, have been reported. Ulnar artery is larger terminal branch of brachial artery, which arises 1cm distal to the flexion crease of the elbow and which reaches the medial side of forearm, midway between wrist and elbow. In forearm, ulnar artery lies deep to superficial flexor group of muscles and lateral to ulnar nerve [1]. The high origin of ulnar artery from brachial artery has been reported in 1.33% of cases (McCormack et al.,). Ulnar artery may arise proximal to the elbow, in which case it lies usually superficial to the forearm flexors (Gabella 1995). Incidence of high origin of ulnar artery ranged from 0.67% (Weathers by) to 9.38% (Devansh) [2].
Case Report
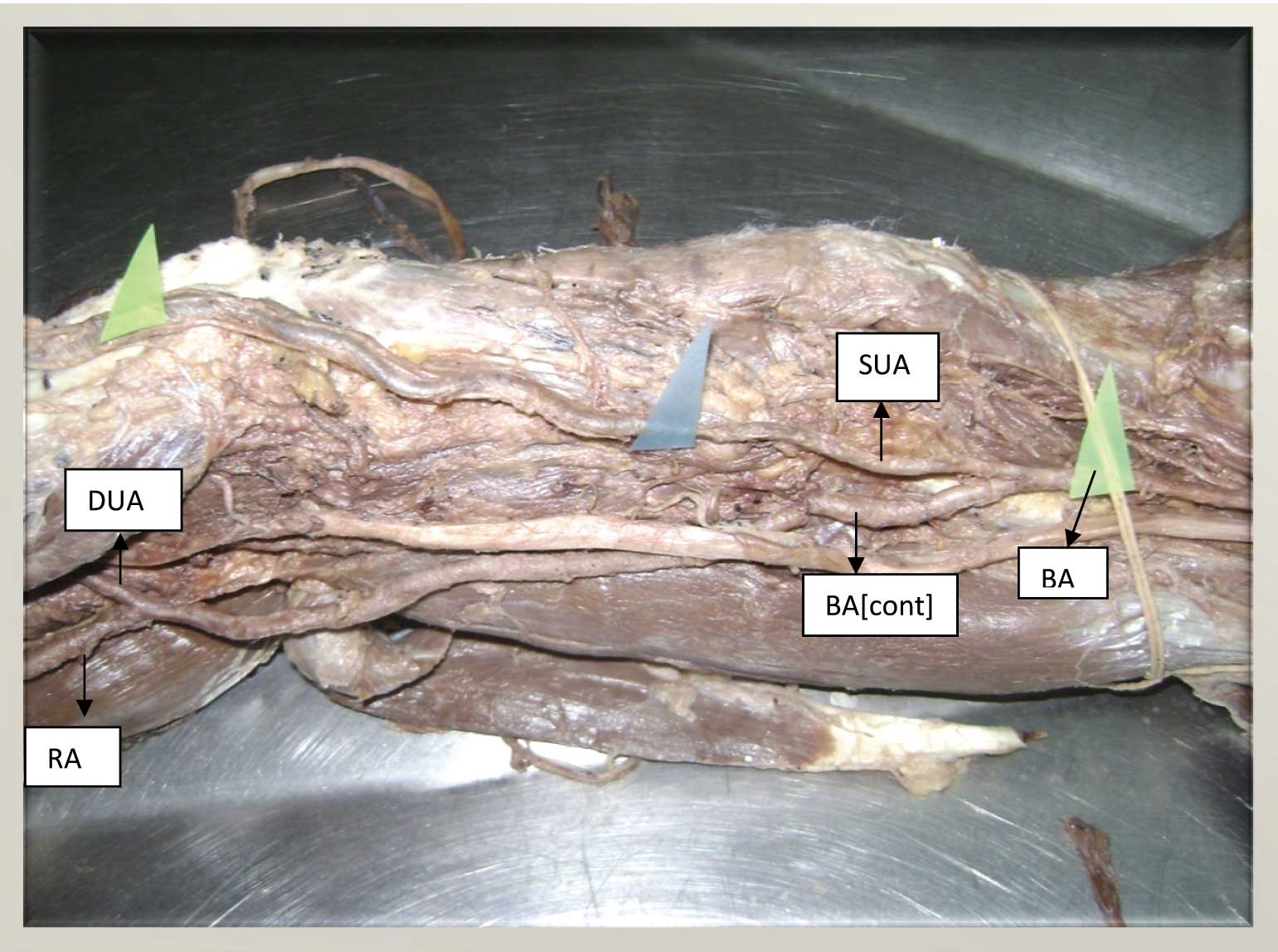
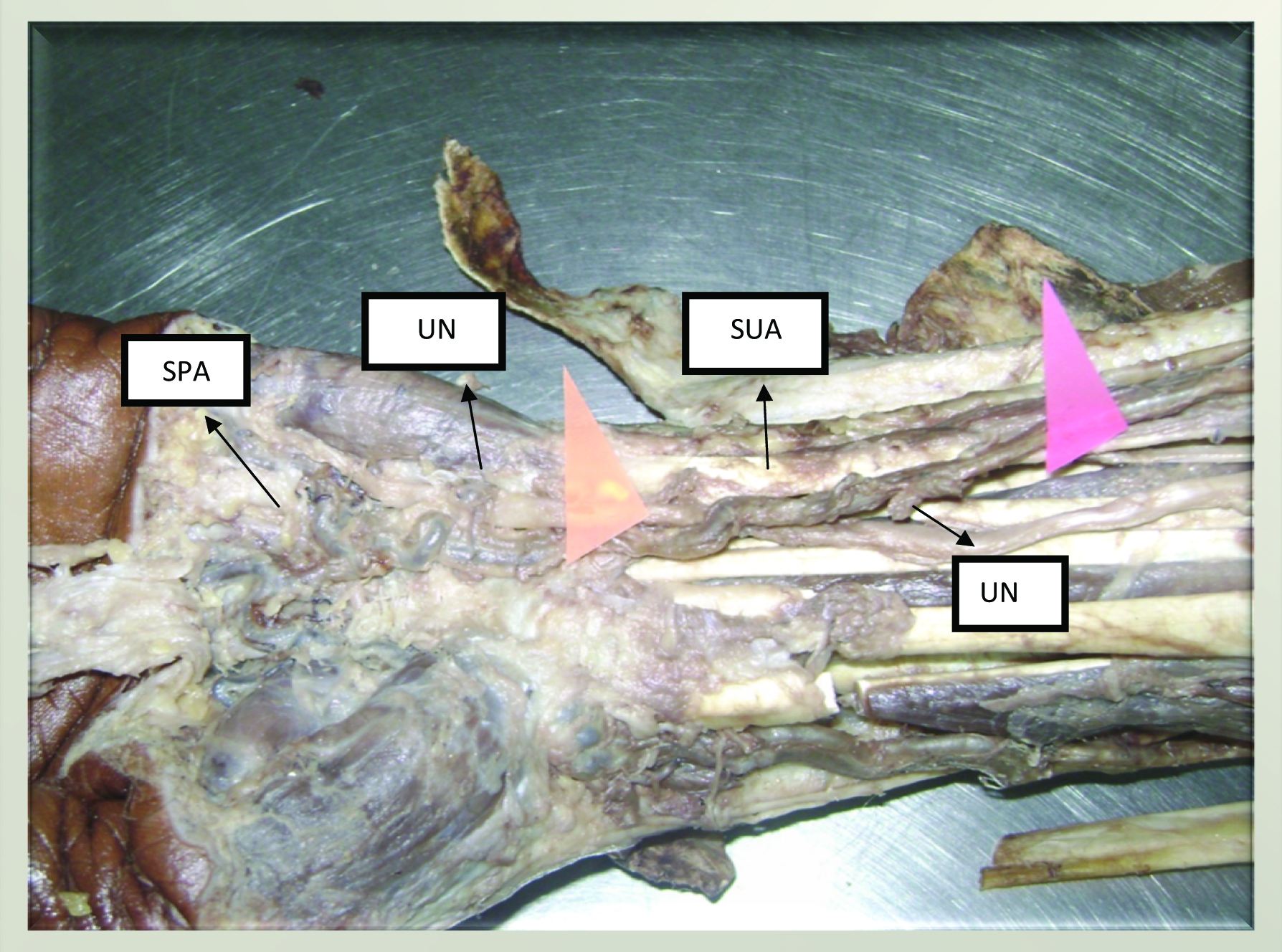
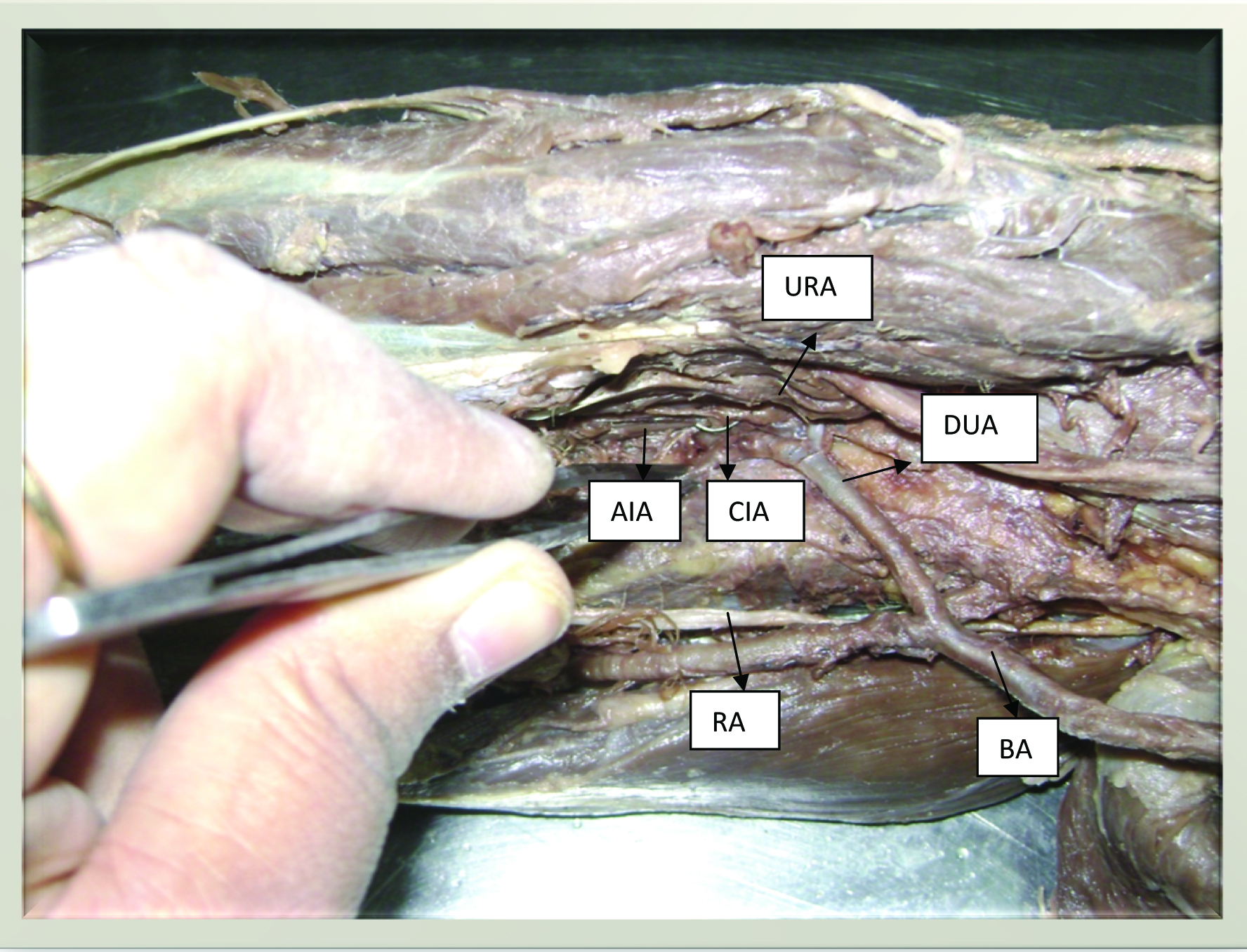
During the routine dissection of an adult male cadaver, 60 years of age, variation in origin and course of ulnar artery was observed. This variation was noted in both the upper limbs. The accessory superficial ulnar artery originated from brachial artery in the proximal one third of the arm and it ran downwards superficially along medial side of forearm [Table/Fig-1]. This ulnar artery was highly tortuous and enlarged. This accessory superficial ulnar artery was found to lie superficial to flexor muscles of forearm. At the wrist, it crossed the ulnar nerve superficially from medial to lateral side and divided into two branches that take part in formation of superficial and deep palmar arches [Table/Fig-2]. The brachial artery had a usual course till the cubital fossa. In the cubital fossa, the brachial artery divided into two branches; a deep ulnar artery and a radial artery [Table/Fig-2]. The radial artery had the usual course and branching pattern. The deep ulnar artery passed deep to flexor muscles of forearm and it divided into ulnar recurrent and common interosseous arteries, which had their usual courses [Table/Fig-3].
Superficial ulnar artery originated from brachial artery in the proximal one third of the arm SUA = superficial ulnar artery; BA = brachial artery; BA cont = brachial artery continued, RA = radial artery; DUA = deep ulnar artery
Superficial ulnar artery crosses the ulnar nerve superficially from medial to lateral side and divides into two branches that take part in formation of superficial and deep palmar arches SUA = superficial ulnar artery; UN = ulnar nerve; SPA = superficial palmar arch
Deep ulnar artery passed deep to flexor muscles of forearm and it divided into ulnar recurrent and common interosseous arteries BA = brachial artery; DUA = deep ulnar artery; RA = radial artery; CIA = common interosseous artery; AIA = anterior interosseous artery; URA = ulnar recurrent artery
Discussion
Anatomic variations in the major arteries of the upper extremities have been reported in 11-24.4% of the individuals [3]. Knowledge on origin, course and distribution of ulnar artery is important, due to its clinical implications. The overall incidence of superficial ulnar artery varies between 0.67% and 9.38%, as reported in the various studies conducted throughout the world. The reported incidence of superficial ulnar artery arising from the axillary artery varies between 0.7% and 2% [3]. The bilateral presence of superficial ulnar artery, with a different origin on each side, is even more rare [4]. High origin of superficial ulnar artery has been reported by Bozer et al., [5]. The present anomaly can be explained on the basis of the persistence of embryological vessels, which may be due to haemodynamic persistence of superficial system over deep system at the origin of ulnar artery. Genetic influences are deemed to be prevalent causes of such variations, although factors like foetal position in utero, first limb movement or unusual musculature cannot be excluded [1]. Co-existence of superficial ulnar artery and aneurysm of the deep palmar arch in the hand was reported by Pulakunta et al., [6]. Shanker et al reported a case with the presence of bilateral superficial ulnar arteries, with an unusual arch in the forearm [7].
A superficial ulnar artery may complicate intravenous drug administration, venipuncture, and percutaneous brachial catheterization. As this artery is mostly superficial, it is more prone to injuries which lead to bleeding and ischaemia [8]. Its superficial course makes it more accessible for cannulation. This artery can complicate surgical procedures like radial artery grafting, for coronary bypass [9].
Knowledge on this variation and complications that can arise due to its presence are of great importance to radiologists, orthopaedic, cardiothoracic and plastic surgeons, for appropriate planning of surgical procedures.
[1]. Standring Susan, Gray’s Anatomy, The Anatomical basis of clinical practice 2008 40th editionLondonElsevier Churchill Livingstone:852-53. [Google Scholar]
[2]. Krishnamurthy A, Kumar M, Nayak SR, Prabhu LV, High origin and superficial course of ulnar artery: a case reportFirat Tip Dergisi 2006 11:66-67. [Google Scholar]
[3]. Uglietta JB, Kadir S, Arteriographic study of variant arterial anatomy ofthe upper extremitiesCardiovasc Intervent Radiol 1989 12:145-48. [Google Scholar]
[4]. Yazar F, Kirici Y, Ozan H, Aldur MM, An unusual variation of the superficial ulnar arterySurg Radiol Anat 1999 21:155-57. [Google Scholar]
[5]. Bozer C, Ulucam E, Kutoglu T, A case of originated high superficial ulnar arteryTrakia Journal of Sciences 2004 2:70-73. [Google Scholar]
[6]. Pulakunta T, Potu BK, Vollala VR, Goranta VR, Thomas H, Co-existence of superficial ulnar artery and aneurysm of the deep palmar arch in the handBratisl Lek Listy 2009 [Google Scholar]
[7]. Shankar N, Veeramani R, Bilateral superficial ulnar arteries with an unusual arch in the forearmInt J AnatVar (IJAV) 2009 2:24-26. [Google Scholar]
[8]. Williams MC RG, Sodha I, Doppler ultrasound diagnosis of a superficial ulnar arteryEur J Ultrasound 2000 12:155-57. [Google Scholar]
[9]. Rodriguez-Neithenfuhr M, Vazquez T, Nearn L, Ferreira B, Sanudo JR, Variation of the arterial pattern in the upper limb revisted: a morphological and statistical study, with arterial review of the literatureJ. Anat 2001 199:547-66. [Google Scholar]