Greater Omental Pancake Tumour due to Metastasis of Ovarian Cancer – A Cadaveric Study
Prashant A. Bhusari1, Karan B. Khairnar2
1 Associate Professor & Head, Department of Anatomy, MVPS, Dr. Vasantrao Pawar Medical College, Adgaon, Nasik-03, Maharashtra, India.
2 Assistant Professor, Department of Anatomy, MVPS, Dr. Vasantrao Pawar Medical College, Adgaon, Nasik-03, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prashant A. Bhusari, Associate Professor & Head, Department of Anatomy, MVPS, Dr. Vasantrao Pawar Medical College, Adgaon, Nasik-03, Maharashtra, India.
Phone: 09604963162, 09604963162,
E-mail: drprashantbhusari@rediffmail.com
Cancer of ovary is the one of the common of all gynecological tumors and is the leading cause of death among women. A unique attempt is made to trace masses & its causes found in an abdomen of female cadaver during routine anatomy dissection.
The mass was thick, hard and somewhat nodular in the region of greater omentum, After dissecting the pelvic cavity, it was found that both the ovaries were bulky, nodular & hard. Whole abdominal cavity was dissected & found that liver also involved by metastasis.
Case suggests that there is the development of metastatic omental mass from grade IV ovarian cancer. Primary human omental adipocytes promote homing, migration and invasion of ovarian cancer cells. Adipokines like interleukin-8 (IL-8) mediate these activities.
Cadaver, Greater omentum, Metastasis, Ovarian cancer ligament
Case Report
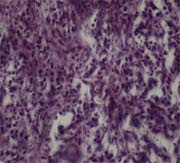
During routine dissection of an abdomen on a female cadaver, large mass was noted covering the whole intestine occupying the major portion of abdominal cavity, extending from greater curvature of stomach into the pelvis. According to history & death certificate, it was seen that patient was suffering from advanced ovarian cancer. It was found that both the ovaries were bulky, nodular & hard [Table/Fig-1 & 2]. The abdominal mass was thick, hard and somewhat nodular in the region of greater omentum, partially adherent to the intestine [Table/Fig-3 & 4]. Whole abdominal cavity was dissected & found that liver also involved by metastasis [Table/Fig-5 & 6]. Microscopic study of the omental mass also reveals the metastatic growth [Table/Fig-7].Histopathological study of omental mass [Table/Fig-7] shows tumour composed of nests & islands of malignant cells infiltrating the connective tissue & stroma. The cells possess large pleomorphic hyperchromatic nuclei &, inconspicuous nucleoli. Frequent mitotic activity & mild to moderate inflammatory infiltrate is noted. Primary human omental adipocytes promote homing; migration and invasion of ovarian cancer cells, and adipokines including interleukin-8 (IL-8) mediate these activities.

showing greater omental pancake tumour

Showing liver metastasis.

Showing histopathology of omental mass
Clinical Presentation
The most common presentations of solid omental tumors included abdominal discomfort, abdominal mass and abdominal distention. Abdominal pain was exacerbated in the supine position and eased by standing upright. Nausea and weight loss sometimes occurs.
Discussion
Ovarian cancer (Ov Ca) has the highest mortality rate of all gynecological tumors and is the fifth leading cause of cancer death among US women [1]. It is predominantly confined within the abdominal cavity and, unlike breast, colon, or lung cancer, rarely metastasizes hematogenously. Once an ovarian epithelial cell undergoes neoplastic transformation, it freely disseminates throughout the peritoneal cavity, carried by peritoneal fluid that facilitates attachment to peritoneum and omentum.The peritoneum is the most common metastatic site (80%) for Ovarian Ca cells [2] followed by liver metastasis (54%), isolated omental mets (46%) [3]. A role for MMPs (matrix metalloprotease pumps) in Ovarian Cancer development has been postulated based upon the observation that several members of the MMP family are upregulated during Ovarian Ca neoplastic progression [4]. Within the peritoneal cavity, omental tissue is a common site for metastatic disease arising from intraperitoneal tumors; however, it is unknown why this tissue is so favorable for metastatic tumor growth [5].
Ovarian cancer is the most lethal gynaecologic malignancy [5,6]. Despite considerable efforts directed at early detection, no cost-effective screening tests have been developed [7]. Thus, the search for tumor markers capable of early detection of ovarian carcinoma is of profound importance and represents one of the most urgent subjects in the study of ovarian cancer. Paley PJ et al., demonstrated that in stage I, the five-year survival rate was about 67%, in stage III and IV, it was about 10% while in total of all stages, it was almost 30%. These data establish the role of anatomo-clinical stage as important prognostic factor in determining the survival [8].
Ovarian epithelial cancers disseminate primarily by surface shedding and by lymphatic spread, while haematogenous dissemination is uncommon. Spread occurs mainly by continuity. At the time of diagnosis, bone or brain metastases are never present and distribution of metastases is not related to the histology or grading of the tumour [9]. At its origin is a rather benign small tumor at the base of the appendix which blocks the passage. Jelly accumulates in the appendix which eventually bursts, releasing jelly and tumor cells in the abdominal cavity. These tumor cells continue to produce jelly, which results in a swollen abdomen and sticking together of parts of the small bowel with obstruction.Our data establishes the role of anatomo-clinical stage as important prognostic factor in determining the survival.
Conclusion
From above all findings, case demonstrates the development of metastatic omental mass from an occult ovarian cancer. It is suggestive of grade IV Ovarian Carcinoma. Ovarian cancer is caused by changes in cancer-related genes. Some biological factors, such as genetic abnormalities, DNA ploidy, steroid receptors, affect the natural history of ovarian cancer. New chemotherapeutic agents have significantly improved the five-year survival rate. Surgical management like, cytodeductive surgery & exploratory laparotomy is the first line treatment in all ovarian cancers patients followed by chemotherapy. Furthermore, genetic testing and risk-reducing oophorectomy should also be considered in the cases with a strong family history for ovarian cancer. Such promising case can be used as an adjunct to the already existing research on ovarian cancer.Further validation using larger data sets warranted to prove the molecular and the biological properties of such carcinomas.
[1]. Cannistra SA, Cancer of the ovaryN Engl J Med 2004 351:2519-2529.2004 [Google Scholar]
[2]. Doig T, Monaghan H, Sampling the omentum in ovarian neoplasia: when one block is enoughInt J Gynecol Cancer 2006 16:36-40. [Google Scholar]
[3]. Platz CE, Benda JA, Female genital tract cancerCancer 1995 75:270-94. [Google Scholar]
[4]. Egeblad M, Werb Z, New functions for the matrix metalloproteinases in cancer progressionNat Rev Cancer 2002 2:161-174. [Google Scholar]
[5]. Gerber Scott A, Rybalko Viktoriya Y, Bigelow Chad E, Lugade Amit A, Foster Thomas H, Frelinger John G, Lord Edith M, preferential attachment of peritoneal tumor metastases to omental immune aggregates and possible role of a unique vascular microenvironment in metastatic survival and growthThe American Journal of Pathology 2006 169(5):1739-52. [Google Scholar]
[6]. Banks E, Beral V, Reeves G, The epidemiology of epithelial ovarian cancer: a reviewInt J Gynecol Cancer 1997 7:425-38. [Google Scholar]
[7]. Ozols RF, Rubin SC, Thomas GB, Robboy SJ, Epithelial ovarian cancer. In: Hoskins WJ, Perez CA, Young RC, (eds)Principles and practice of gynecologic oncology 2000 3rd edPhiladelphiaLippincott, Williams, and Wilkins:981-1057. [Google Scholar]
[8]. Paley PJ, Ovarian cancer screening: are we making any progress?Curr Opin Oncol 2001 13:399-402. [Google Scholar]
[9]. Pickel H, Lahousen M, Girardi F, Tamussino H, Stettner H, Intraperitoneal and retroperitoneal spread of ovarian cancer. In: Sharp CF, Mason WP, Leake R. (eds)Ovarian Cancer: Biologic and Therapeutic challenges 1990 LondonChapman and Hall [Google Scholar]