It has been estimated that one third of the world population has been infected with toxoplasmosis [4,5]. According to a World Bank report published in 2012, rural population in Egypt was last reported at 57.2%, most of them are working on farms with an increasing number of poor people. A previous study +has shown a 57.9% seroprevalence rate of T. gondii among pregnant women in Egypt [6]. This high seroprevalence rate of T. gondii may be responsible for a significant number of early miscarriages among this population. The aim of the current study was to determine the seroprevalence and risks factors for toxoplasmosis among women with first trimester miscarriage.
Subject and Methods
In this prospective cross-sectional hospital based-study, 76 women with first trimester miscarriage underwent evacuation at Qena University Hospital South Valley University, Egypt from January, 2012 through March, 2013. This study was approved by the Ethics Committee of Qena University Hospital South Valley University, and a written consent was obtained from each participant.
Inclusion Criteria
Women with spontaneous miscarriage at 2-8 weeks gestations. Gestational age was determined by the last menstrual period and was confirmed by ultrasound scan.
Demographic data, including maternal age, parity, duration of marriage and educational level were recorded. Outcomes were assessed included antibody titers for Both IgG/IgM, and the histopathology of the conceptus materials for those with positive titer.
Technique: From all subjects blood was drawn for serological testing. All conceptus materials, of seropositive persons were further processed for Histopathological study.
Serological Detection of Toxoplasma gondii infection
Five ml of venous blood were collected aseptically from each of the study participants. Then serum was separated from the whole blood by centrifugation at 3000 rpm for 5 minute. Sera were isolated and kept in sterile microtubes at -20°C until use for serological examinations. All the collected specimens were tested for IgM and IgG anti-Toxoplasma gondii antibodies by enzyme-linked immunosorbent assay (ELISA) test kit (SeraQuest® TOXOPLASMA) provided from Quest International, Inc. Miami, FL, USA); following the manufacturer’s instruction.
Parasitological Detection of Toxoplasma gondii Infection
The tissue slides were deparaffinized and rehydrated through graded alcohols to water. Then, they were rinse in pH 6.8 buffered distilled water, stained in working Giemsa, overnight and rinsed and dehydrated gradually and cleared, mounted and covered by cover slide.
Histopathology
Samples of miscarriage materials were collected and immersed into 10% neutral buffered formalin for fixation. Samples were dehydrated and embedded in paraffin wax in the usual manner, sectioned (4 μm thick) and stained with hematoxylin and eosin (H&E). Two to three paraffin embedded blocks were prepared for each specimen. Tissues were investigated for toxoplsama schizont, male and female gametes.
Statistical Analysis
The Statistical Package for the Social Sciences for Windows, version 15 (SPSS Inc., Chicago, Illinois) was used to record data and for analyses. The descriptive analyses used included the mean, standard deviation, and frequency distribution. For logistic regression using multivariate analysis, independent variables were added to the model at the same time, whereas in the univariate analysis, each variable was entered separately. The results of the analysis are presented as odds ratios (ORs) and 95% confidence intervals (95% CIs). A p value <0.05 was considered significant.
Results
The total number of cases in this study was 76 patients with first trimester miscarriages (2 to 8 weeks gestations). The study revealed that T. gondii IgG antibodies were detected in 46.1% (n=35) of the samples; of which 27.6% were positive for IgG and 18.4% positive for both IgG and IgM antibodies. Therefore, seropositivity rates of 46.1 % (95% CI: 35.1%, 57.3%), and 18.4% (95% CI: 10.89%, 28.32%) for IgG and IgM, respectively were found. The mean IgG and IgM levels were (16.7714±5.39109 and 8.5714±11.01946) respectively.
The mean maternal ages of the studied women were 26.8158 ± 5.474±409 years, ranged (19 to 36) years. Their mean parities were 2.3684±1.67206, ranged (0 to 5) deliveries.
[Table/Fig-1] shows the selected socio-demographic characteristics of the studied population and the association with serology for toxoplasmosis. The seroprevalence of toxoplasmosis was found to be higher among women less than 25 years of age (42.1%) and lowest among 25-29-year-old (18.4%). Again, the seroprevalence of toxoplasmosis was more among women with secondary education (31.4%), more often multiparous (65.7%) and living in rural areas (65.7%). It was less common among 25-29-year-old women (18.4%) and those with basic education (20.0 %) and those living in urban areas (31%).
Socio-demographic characteristics of the studied women and the association with the prevalence of toxoplasmosis Values are presented as number (percentage)
| Characteristics | Frequency (%) | Serology |
|---|
| Age group (years) | Negative | Positive |
| >25 | 32(24.8) | 16(39.0) | 16(42.1) |
| 25-29 | 14(10.9) | 8(19.5) | 6(18.4) |
| 30 and more | 30(23.3) | 17(41.5) | 13(39.5) |
| Educational level | | | |
| Illiterate | 20(15.5) | 11(26.8) | 9(25.7) |
| Basic | 18(14.0) | 11(26.8) | 7(20.) |
| Secondary | 20(15.5) | 9(22.0) | 11(31.4) |
| University | 18(14.0) | 10(24.4) | 8(22.9) |
| Total number of pregnancies |
| Primi | 16(12.4) | 8(19.5) | 8(22.9) |
| Multi | 49(38.0) | 26(63.4) | 23(65.7) |
| Grand | 11(8.5) | 7(17.1) | 4(11.4) |
| Residence | | |
| Urban | 36(27.9) | 24(58.5) | 12(34.3) |
| Rural | 40(31.0) | 17(41.5) | 23(65.7) |
| Serology of toxoplasma |
| Negative | 41(31.8) | | |
| Positive | 35(27.1) | | |
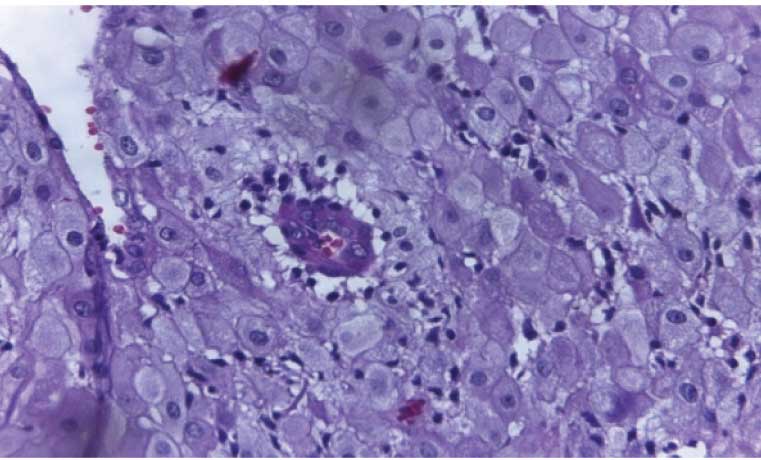
The histological findings in the majority of the conceptus materials of seropositive women revealed areas of focal necrosis with leukocytic infiltrations of the deciduas. Furthermore, deciduas infiltrations with mononuclear cell with vasculitis and perivascular edema were reported in some cases [Table/Fig-2].
The decidua shows a mononuclear cell infiltration with vasculitis and perivascular edema from conceptus material at evacuation in a-33-year-old woman with first trimester abortion complicated with toxoplasmosis (H&E x100)
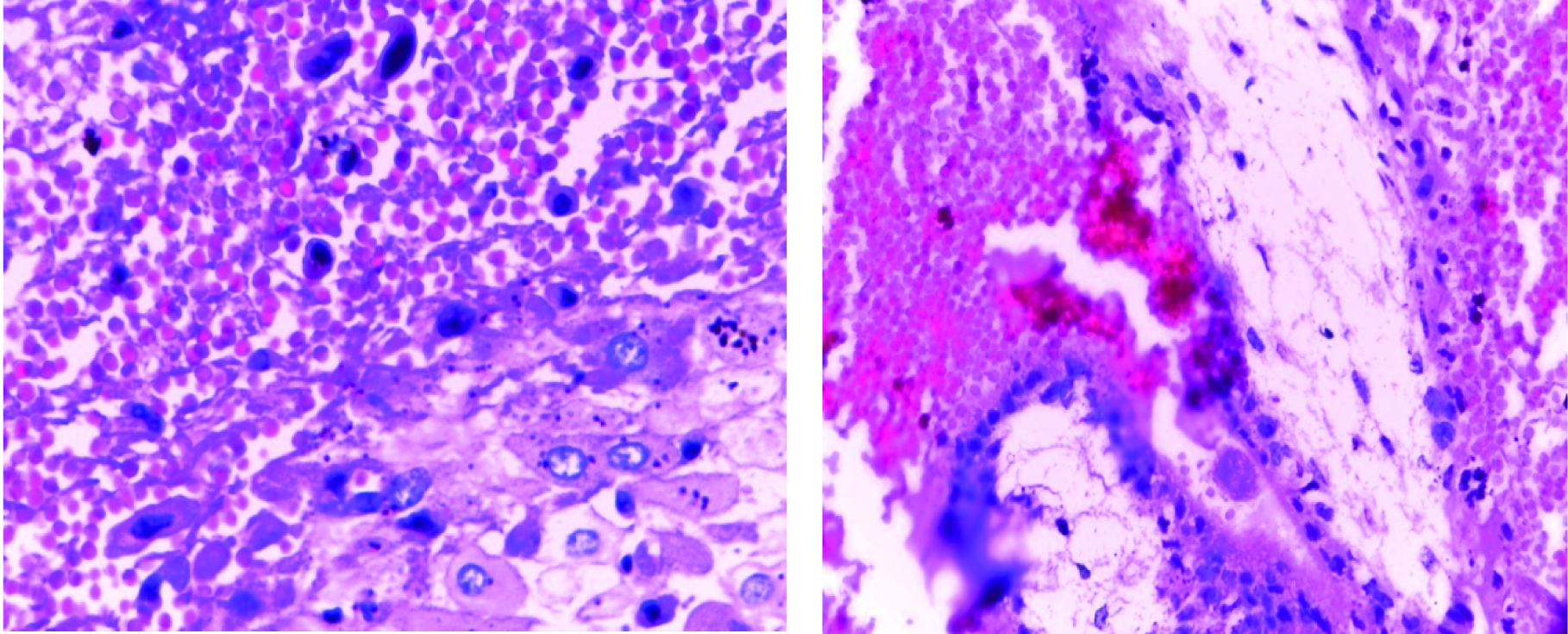
As regard to the parasitological examination of the conceptus material, the tachyzoites and the Toxoplasma cyst were demonstrated in one case [Table/Fig-3].
Banana-tachyzoites: obtained from conceptus material at evacuation in a33-year-old women with first trimester abortion complicated with toxoplasmosis (H&E x100)
Toxoplasma gondii cysts obtained from conceptus material at evacuation in a33-year-old woman with first trimester abortion complicated with toxoplasmosis (H&E x100)
In [Table/Fig-4], univariate and multivariate analysis of sociodemographic characteristics of the studied women showed that there was a significant association between seroprevalence of toxoplasmosis and living in rural areas.
Logistic regression analysis of predictors of T. gondii infection in women with first trimester spontaneous miscarriage
| Variable | Univariate | Multivariate |
|---|
| OR | 95% CI | p-value | OR | 95% CI | p-value |
|---|
| Age group |
| >25 | 1.00* | | | | | |
| 25-29 | 1.308 | 0.481-3.558 | 0.599 | 0.982 | 0.045-1.723 | 0.169 |
| 30 and more | 0.981 | 0.272-3.532 | 0.976 | 0.596 | 0.027-1.892 | 0.170 |
| Parity |
| Primigravida | 1.00* | | | | | |
| multigravida | 1.750 | 0.364-8.424 | 0.485 | 0.991 | 0.635-410.730 | 0.092 |
| grand multiparas | 1.548 | 0.401-5.975 | 0.526 | 0.673 | 0.779-114.403 | 0.078 |
| Residence |
| urban | 1.00* | | | | | |
| rural | 2.706 | 1.063-6.889 | 0.037 | 3.800 | 1.100-10.813 | 0.034 |
| Educational level |
| University | 1.00* | | | | | |
| Illiterate | 1.023 | 0.284-3.681 | 0.973 | 0.637 | 0.147-2.765 | 0.547 |
| Basic | 0.795 | 0.211-3.000 | 0.735 | 0.906 | 0.205-4.009 | 0.896 |
| secondary | 1.528 | 0.424-5.499 | 0.517 | 1.963 | 0.454-8.480 | 0.366 |
Abbreviations: OR, odds ratio; CI, confident interval; p-value was set significant at <0.05
1.00* reference category
Discussion
The diagnosis of toxoplasmosis poses a challenge for health care givers due to the complexity in the interpretation of the results. The diagnosis of toxoplasmosis in human is common done by serologic tests (in which the interpretation should be done meticulously), PCR and histologic demonstration of the parasite [7]. However, biopsy should be used in selective cases because it is an invasive.
In the current study, the seroprevalence of IgG antibodies to T. gondii in women with early spontaneous miscarriage was found to be 46.1%. A similar previous study from Qualyobia governorate reported a seroprevalence of 44.7% among aborted women, which comparable with our findings [6]. However, the seroprevalence found in women with early miscarriage is lower than seropositivity reported recently in other governorates in the country, Menoufia [8] in 67.5% and Gharbia [9] in 52.4% of cases, indicating that infection with toxoplasmosis is on the rise. The 46.1% seropositivity rate is high when compared to Dakahlia (23.85%) [10], and EL Fayoum (30.5%) [11] [Table/Fig-5]. As regards to the nearby countries; the seroprevalence in the current study is comparable to Tunisia [12] in 39.3%, but it is higher compared to seroprevalence of toxoplasmosis in Sudan [13] in 34.1% and Palestine [14] in (27.9%) of cases. However, it is much higher than the 31·0% found in younger women in their reproductive age in Italy [15], and the 15.0% found in women aged 15-44 years in United states [16].
Comparison of sero prevalence of T. gondii in different Governorates of Egypt and some selected countries ELISA, indirect enzyme linked immunosorbent assay; IHAT, indirect hemoagglutination test
| Variables | Seroprevalence of T. gondii |
|---|
| In governorates of Egypt | In other countries |
|---|
| Qualyobia | El Fayoum | Menoufia | Dakahlia | Gharbia | Sudan (Khartoum) | Tunisia (Tunisia) | Palestine Hebron | Palestine | Central Italy | United States |
| Year of study | 2001 | 2006 | 2012 | 1993 | 1997 | 2003 | 1994-2006 | 2005 | 2005 | 2012 | 1988-1994 |
| population | Aborted women | Pregnant and non pregnant | Pregnant women | Different localities | Slaughter | Pregnant women | Population | Rural | Urban | Younger women | Women 15-44 years |
| Sample size | 38 | 88 | 323 | 320 | 162 | 487 | 40,566 | 2005 | 2005 | 13 000 | 17,658 |
| Test used | ELISA | ELISA | ELISA | Dot-ELISA | IHAT | ELISA | ELISA | ELISA | ELISA | ELISA | ELISA |
| IgG % | 44.7% | 30.5% | 67.5% | 23.8% | 52.4% | 34.1% | 47.7% | 21.4% | 21.4% | 31·0% | 15.0% |
| IgM % | 23.7% | 24.2% | 2.8% | - | - | 14.3% | - | - | - | 1·6% | - |
The variations in the seroprevalence rate whether nationally or in nearby countries should be interpreted cautiously since different tests with different sensitivity and specificity were used, along with different population having different susceptibility to infection as evident in [Table/Fig-5]. Moreover, the seroprevalence may be influenced by the study population, age, sample size, study area, number of cat and their infectivity and geographical variation may account for some of the differences in the reported seroprevalence [4, 17].
In the current study, the seroprevalence of IgM for toxoplasmosis was found be 18.4 % ( n=14). It is comparable with most of the governorates in Egypt except for Qualyobia and El Fayoum that reported higher seroprevalence for IgM [Table/Fig-5]. High environmental contamination (97.4%) with T. gondii oocytes from rats [18], in addition to inadequate hygiene, and suitable climatic factors for survival of oocysts might be responsible for this high seropositivity.
In the current study, there were 21(27.7%) patients with (IgG+/ IgM-) results, which indicates infection with the organism at some time, usually old infection, while there were 14(18.4%) patients with (IgG+/IgM+) results, which indicates recent infections. We cannot grantee that it was responsible for pregnancy loss in this study. In pregnancy, it is mandatory to perform additional conclusive tests that must include, IgG avidity test, PCR, IgA and IgE, on individuals with both positive IgG and IgM [19], because Toxoplasma-specific IgM antibodies may be persist as long as 18 months after acute acquired infection [20].
T. gondii infection was 3.8 times greater in individuals who live in rural areas than those in urban areas. Our results were in agreement with El-Gozamy et al., study which was conducted between August 2007 and October 2008 in Egypt, concluded that seropositivity for T. gondii among pregnant women was relatively high in the rural (57.6%) than urban (46.5%) areas [12]. High positivity for toxoplasmosis in rural areas may indicates the life style of the inhabitants which makes them more prone to the infection, again high density of domestic animals in rural areas as well as the favorable environmental conditions for T. gondii oocysts to sporulate. Unwashed food, lack of sanitary water may all contribute to high positivity in rural areas [21]. In the current study, there was no association between an increasing maternal age and seropositivity for T. gondii as reported by others authors [22,23].
In this study, tachyzoites were isolated from the conceptus materials in one case (2.9%) of the 35 seropositive cases. Biopsy is considered the most definitive method of diagnosis for toxoplasmosis because this method may demonstrate the presence of tachyzoites. It has been reported that toxoplasmosis has a significant relation with first trimester miscarriage [24]. The mechanism by which toxoplasmosis induced abortion is either inhibits or triggers the apoptosis with excessive levels of Th1 cytokines, particularly IL-18 and IFN- γ (Nishikawa et al., 2002)[25]. This indicates that toxoplasmosis induce abortion through a chain of immunological reactions, therefore negative biopsy does exclude toxoplasma gondii as a causative agent.
Conclusion
In the current study high seropositivity for toxopalsma gondii was reported (18.4%) indicating potential for abortion and congenital transmission. Women living in rural areas are at higher risks for T. gondii infection. Antenatal screening of pregnant women and educational program about risk for Toxoplasmosis in rural areas is needed.
Abbreviations: OR, odds ratio; CI, confident interval; p-value was set significant at <0.05
1.00* reference category