Peak Expiratory Flow Rate In Healthy Rural School Going Children (5-16 Years) of Bellur Region For Construction of Nomogram
Manjunath CB1, Kotinatot SC2, Manjunatha Babu3
1 Assistant Professor, Department of Paediatrics, Vydehi Institute of Medical Sciences Whitefield, Bangalore, India.
2 Fellow in Neonatology, AJIMSMangalore, India.
3 AssistantProfessor, Department of Paediatrics, KIMSNarketpally, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manjuanath CB, Department of Paediatrics, Vydehi Institute of Medical Sciences White field Bangalore, Karnataka, India. Ph-08050644372 E-mail : drcbm2008@rediffmail.com
Background: Peak Expiratory Flow Rate (PEFR) recording is an essential measure in the management and evaluation of asthmatic children.It is helpful in monitoring disease progression and response to treatment. The PEFR can be measured by a simple instrument—peak expiratory flow meter.
Aims and Objectives: To construct nomogram of PEFR in healthy rural school going children from Mandya district of Karnataka state, India and to use these nomograms for comparison with that of children with obstructive lung diseases for this region.
Material and Methods: The study was conducted on Healthy rural school going children, both boys and girls between the age group of 5-16 years. For the determination of PEFR we used Mini Wright Peak Flow Meter. At three time measurement, the highest value of PEFR was recorded. Formula for prediction of PEFR was estimated by linear regression analysis after the correlation of PEFR with age and height for both boys and girls.
Results: PEFR was measured in 1028 children aged 5 to 16 years by using Wright’s mini peak flow meter. Prediction equations were derived for PEFR with height in boys and girls. Normograms were plotted based on the observed values of PEFR in the study population. Significant linear correlation was seen of PEFR with height in boys (p<0.001, r=0.7624) and in girls (p<0.001, r=0.8825). Prediction equation for PEFR are -317.43 + 4.40 x height (cm) in boys and – 321.21 + 4.25 x height (cm) in girls.
Conclusion: Reference values of PEFR are affected by regional, environmental and anthropometric factors. Hence, it is necessary to have regional reference values for children. Among different factors affecting PEFR, height correlates better with PEFR than weight and sex. Hence nomograms constructed can be used for this region
PEFR, Height, Children, Regional references
Introduction
Respiratory disorders are major group of illness affecting children especially in India and are the important causes of childhood morbidity and mortality. In particular, obstructive airway diseases rise in children due to environmental pollution and other causes. So, assessment of pulmonary function test in such children is very important. The PEFR is one among the lung function test which is helpful in evaluating obstructive lung diseases especially bronchial asthma. It is also helpful in monitoring the disease progression and response to treatment. The Peak Expiratory Flow Rate (PEFR) is an effort-dependent parameter, emerging from the large airways within about 100-120 msec of the start of forced expiration. It remains at its peak for 10 msec [1]. It is well documented in literature that a wide range of geographical, climatic, anthropometric, nutritional, and socioeconomic conditions of India are associated with regional differences in lung function [2]. Besides anthropometric and socioeconomic factors, altitude is an important determinant of lung function [3].
From various studies we know that, the PEFR affected by age, sex, weight and height (Anthropometry) and also the PEFR varies from urban to rural areas. More over it varies from region to region also. So, it is important to have a normal reference values for each region.Since, the catchment population for treatment to AIMS Bellur hospital consists of children from this region of Karnataka, India and the morbidity due to respiratory conditions are quite high, it was decided to carry out a study to find out their respiratory function in an objective and feasible method to manage and monitor patients with obstructive airway diseases, Asthma in particular.
Material and Methods
The cross- sectional study was carried out at AIMS Bellur on normal healthy school going children in the age range of 5-16 years of Bellur region involving two schools over a period of 6 months. All children from both schools meeting inclusion criteria were enrolled in the study. Permission was obtained from the relevant school authorities. Children of both sexes in the above age range belonging to the rural areas along with their parents were provided with written information on the intension of the survey and requested a written consent from the parents for the participation of each student in the survey. The students of the higher class were, in addition, given a brief talk on the study intended and obtainedrequired permission. The students from less affluent status (most) where parents literacy was poor, the class teacher has given consent as guardian. A detailed history, followed by a thorough clinical examination was done as per the latest guidelines laid down by the American Thoracic Society [4]. These children were then interviewed to rule out the following.
1. History suggestive of cold or any other respiratory disease within the preceding two weeks.
2. Past history of asthma, allergies or chest injuries.
3. Family history of asthma among first degree relatives.
Finally, all children were selected randomly. Age was taken as completed years as on the school records. The anthropometric measurements were taken were weight and height. Weight was taken without foot wear and with school uniform. The weighing machine was put on an absolutely flat surface and was calibrated before taking measurements. Accuracy of the machine was ± 50 grams. Any fraction of weight thus measured was corrected to the nearest kilogram. Children who were found as malnourished as per the Indian Academy of Paediatrics criteria (All grades ofmalnutrition) were excluded from the study. The height of children was measured using stadiometer without footwear and child standing erect with the heel and back against anthropometric rod. The measured height was then corrected to the nearest centimeter. Throughout the study same balance and stadiometer were used.
A new mini-wright peak flow meter (obtained from clement Clarke International Ltd., U.K) was used as instrument. A single instrument was used throughout the study. The instrument with a graduated scale on the surface and a mouth piece. The graduation starts with 60 L/min to 800 L/min with accuracy of 10 L/min. In about 400 children disposable mouthpieces were used and remaining children The mouthpiece was washed and sterilized for each subject [5].
The nose clips were not worn. Before the test was carried out the purpose and technique of measurement were explained to each child. All children were tested in standing position. After a practical demonstration the subject was asked to take deep breath and then blow out as hard as possible, in a short sharp blast through the mouth piece of peak flow meter. The resulting flow rate was read from the dial on the meter. At least 5 readings were taken after several practice trials and the mean of three highest values was recorded in the proforma. Measurement of flow rate was carried out by single observer, so that inter observer variation was eliminated.
Statistical Analysis
The data was analysed separately for boys and girls with respect to age, weight, height and PEFR for all children and statistical diagrams were prepared The predictions equations for PEFR based on the height alone were determined for both sexes and also regression equations for both groups (Boys & Girls) were determined. All the results were subjected to standard statistical evaluation (SPSS Package in software) and regression equation for PEFR was obtained based on height.
Results
One thousand twenty eight helathy children of both sexes between 5-16 years were analysed for PEFR values. There were 571 boys and 437 girls. The PEFR values increased in linear relation to age weight and height. The mean age of the boys was 10.68 ± 3.45 years, mean height was 138.57 ± 15.82cm and mean weight was 31.23±10.56kg. The mean age of the girls was 10.49 + 3.45 years, mean height was 135.45+ 16.14cm and mean weight was 30.18 + 10.96kg. The mean PEFR were 292.85+ and 255.01+77.80 for boys and girls respectively. [Table/Fig-1 and 2] give the PEFR values in relation to height for boys and girls respectively.
| AGE (Years) | N | MEAN HEIGHT (Cms) | S.D. | r | REGRESSION EQUATION FOR PEFR |
|---|
| 5 | 45 | 112.36 | 9.41 | 0.08 | 137.02+0.27x |
| 6 | 46 | 120.74 | 9.78 | 0.11 | 229.38-0.33 x |
| 7 | 47 | 123.98 | 5.36 | 0.35 | -22.12+1.87 x |
| 8 | 48 | 129.06 | 6.37 | 0.31 | -370.41+4.81 x |
| 9 | 50 | 135.30 | 10.58 | 0.08 | 187.45+0.62 x |
| 10 | 48 | 137.00 | 6.90 | 0.47 | -105.59+2.84 x |
| 11 | 46 | 138.33 | 6.57 | 0.47 | -152.42+3.32 x |
| 12 | 51 | 144.27 | 6.99 | 0.49 | -87.78+2.90 x |
| 13 | 53 | 148.93 | 8.37 | 0.40 | -39.83+2.52 x |
| 14 | 51 | 150.00 | 8.72 | 0.38 | -88.08+2.95 x |
| 15 | 54 | 154.00 | 9.14 | 0.48 | -169.61+3.49 x |
| 16 | 52 | 159.08 | 9.48 | 0.73 | -458.09+5.40 x |
| AGE (Years) | N | MEAN HEIGHT (Cms) | S.D. | r | REGRESSION EQUATION FOR PEFR |
|---|
| 5 | 36 | 108.31 | 3.20 | 0.10 | 79.04+0.68x |
| 6 | 35 | 115.20 | 2.81 | 0.08 | 262.13-0.87 x |
| 7 | 37 | 121.43 | 3.78 | 0.21 | 55.32+0.95 x |
| 8 | 39 | 121.64 | 7.49 | 0.24 | 98.16+0.92 x |
| 9 | 39 | 131.33 | 5.81 | 0.50 | -182.18+3.08 x |
| 10 | 33 | 136.33 | 5.07 | 0.29 | -153.19+2.92 x |
| 11 | 35 | 139.60 | 6.31 | 0.48 | -129.15+2.78 x |
| 12 | 40 | 144.30 | 5.93 | 0.51 | -207.59+3.53 x |
| 13 | 35 | 148.60 | 6.88 | 0.70 | -262.94+3.86 x |
| 14 | 37 | 150.97 | 6.66 | 0.41 | -74.67+2.65 x |
| 15 | 33 | 153.70 | 4.97 | 0.45 | -122.96+3.07 x |
| 16 | 38 | 154.92 | 5.48 | 0.38 | -90.96+2.85 x |
The PEFR values increased in linear relation to age, weight and height. The coefficient of correlation obtained for all the three variables was significant (p<0.001). The highest correlation was obtained between PEFR and height (r=0.8825 for girls, r=0.7624 for boys). The regression equation based on height for both sexes were [Table/Fig-3 and 4].
Pefr for various hieghts with regression equation in boys

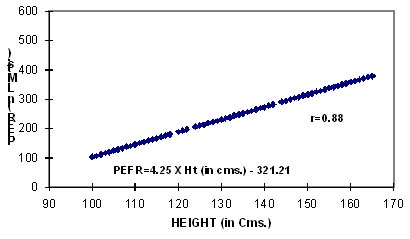
Pefr for various heights with regression equation in girls
Boys: PEFR (L/min) = 4.40 × Ht (cm) – 317.42 L/min.
Girls: PEFR (L/min) = 4.25 × Ht (cm) – 321.21, L/min.
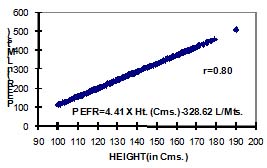
A nomogram has been constructed from the linear regression equation by using PEFR as a dependant variable and height as a independent variable since the difference in PEFR between boys and girls at given height (variability) is only 7-8%. Hence we combined the data for the purpose of nomogram. This can be used for quick estimationof PEFR at any given height [Table/Fig-5]. The regression equation in both sexes based on height is:PEFR= 4.41× Ht (cm) – 328.62 L/min.
Pefr for various heights with regression equation in both sex
Discussion
Assessment of lung functions both qualitatively and quantatively in both healthy and diseased subjects has become important in the field of Respiratory medicine. Measurement of PEFR has gained worldwide importance in clinical practice for evaluation of patients with obstructive and restrictive airway diseases. Particularly following development of simple handy instrument like the miniwright peak flowmeter. In those known to have asthma, such tests are useful in assessing the degree of airway obstruction and the disturbance in gas exchange, in measuring response of the airways obstruction and the disturbance in gas exchange, in measuring response of the airways to inhaled allergens and chemicals or exercise, in assessing the response to therapeutic agents, and in evaluating the long term course of the disease [6,7]. Our aim was to establish normal values of PEFR for healthy rural children of Bellur (Karnataka), as PEFR is a reliable measurement, which can be used routinely and regularly in rural areas for assessment of airway obstruction and prediction formula derived for use in this population [8].
A standardized comparison of predicted PEFR values from the present study for 3 different heights was done with the PEFR values for the same height from 5 previous studies [Table/Fig-6].On comparing our data with previously published values, we found that PEFR meausrements in rural children are comparable with previous studies [Table/Fig-6]. PEFR values increased in linear relation to age, weight and height. Similar to our study results, many other authors have also found a significant positive correlation of PEFR with age, height, and weight, out of which height has been maximally correlated with PEFR [8–16]. It will also be possible to predict PEFR for a given height by calculating it from our equation. We used height for constructing the regression equation for predicting PEFR because it is a convenient measurement and its assessment is accurate, if proper technique is used. Assessment of correct age in rural area in many instances is not possible and accurate weight measurement in field studies may sometimes pose a problem. It has been shown that pulmonary function, especiality lung volume show racial and ethnic differences [17,18]. Within India also, ethnic differences have been shown to account for the variations in the pulmonary functions [17]. Therefore, it is important to establish reference values for this region. The regression equations obtained in the present study can be used to calculate the expected value of PEFR, which can serve as reference value. We would like to state that a data from few villages is not representative of characteristics of a region. Therefore, the findings of the present study should be considered preliminary and call for further studies with a large sample size based on random selection.
Comparison of pefr (l/min) predicted from present study with those studies in caucasian and indian (north and south) urbanand rural children.
| AGE (Years) | Taksande A et. al., 2008 n=1078 | Mohammadzadeh I.2006 Iran n=1050 | Shallu Mittalet. al., 2013, India (Punjab) n=366 | Rajeshsharma et. al., 2001, N. India (Rajasthan Rural) n=303 | Paramesh H et. al., 2002 S. India (Bangalore) | Present study, Karnataka Bellur , Rural n=198 |
|---|
| B | G | B | G | B | G | B | G | Common | | |
| 120 | 212 | 211 | 222 | 216 | 205 | 193 | 199 | 186 | 200 | 210 | 188 |
| 140 | 318 | 317 | 320 | 314 | 286 | 272 | 285 | 273 | 300 | 298 | 273 |
| 160 | 423 | 422 | 415 | 412 | 368 | 350 | 372 | 361 | 400 | 386 | 358 |
Prediction Equations:
Boys : PEFR (L/min) = -317.42 + 4.40 X Height (Cm)
Girls : PEFR (L/min) = -321.21 + 4.25 X Height (Cm)
In conclusion, this study has generated preliminary reference values for PEFR for rural children of Bellur, India.
Prediction Equations:
Boys : PEFR (L/min) = -317.42 + 4.40 X Height (Cm)
Girls : PEFR (L/min) = -321.21 + 4.25 X Height (Cm)
[1]. Dikshit MB, Raje S, Agrawal MJ, Lung functions with spirometry: An Indian perspective-I. Peak expiratory flow ratesIndian J Physiol Pharmacol 2005 49:8-18. [Google Scholar]
[2]. Raju PS, Prasad KV, Ramana YV, Murthy KJ, Pulmonary function tests in Indian girls- prediction equationsIndian J Paediatr 2004 71:893-7. [Google Scholar]
[3]. Gupta S, Mittal S, Kumar A, Singh KD, Peak expiratory flow rate of healthy school children living at high altitudeN Am J Med Sci 2013 Jul 5(7):422-6. [Google Scholar]
[4]. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Standardisation of spirometryEur Respir J 2005 26:319-38. [Google Scholar]
[5]. Agaba PA, Thacher TD, Angyo IA, Agaba EI, Peak expiratory flow rates in healthy Nigerian childrenJ Trop Paediatr 2003 49:157-9. [Google Scholar]
[6]. Chowgule RV, Shetye VM, Parmar JR, Lung function tests in normal Indian childrenIndian Paediatr 1995 32:185-91. [Google Scholar]
[7]. Chessnut MS, Prendergast TJ, Stauffer JL, Lung. In :Current Medical diagnosis & treatment 1999 38th Edn.ConnecticutPrentice – Hall International Inc:260Eds: Tierney LM, McPhee SJ and Papadakis M [Google Scholar]
[8]. Taksande A, Jain M, Vilhekar K, Chaturvedi P, Peak expiratory flow rate of rural school children from Wardha district, Maharashtra in IndiaWorld J Paediatr 2008 Aug 4(3):211-4. [Google Scholar]
[9]. Mohammadzadeh I, Gharagozlou M, Fatemi SA, Normal values of peak expiratory flow rate in children from the town of Babol, IranIran J Allergy Asthma Immunol 2006 5:195-8. [Google Scholar]
[10]. Raju PS, Prasad KV, Ramana YV, Ahmed SK, Murthy KJ, Study on lung function tests and prediction equations in Indian male childrenIndian Paediatr 2003 40:705-11. [Google Scholar]
[11]. Sharma M, Sharma RB, Choudhary R, Peak expiratory flow rates in children of western Rajasthan, 7-14 years of agePak J Physiol 2012 8:45-8. [Google Scholar]
[12]. Mittal Shallu, Gupta Sharat, Kumar Avnish, Singh Kamal Dev, Regression equations for peak expiratory flow in healthy children aged 7 to 14 years from Punjab, IndiaLung India 2013 Jul 30(3):183-6. [Google Scholar]
[13]. Malik SK, Jindal SK, Sharda PK, Banga N, Peak expiratory flow rate of healthy schoolboys from PunjabIndian Paediatr 1981 18:517-21. [Google Scholar]
[14]. Malik SK, Jindal SK, Sharda PK, Banga N, Peak expiratory flow rates of school age girls from Punjab (Second report)Indian Paediatr 1982 19:161-4. [Google Scholar]
[15]. Paramesh H, normal peak expiratory flow rate in urban and rural childrenIndian J Paediatr 2003 70:375-77. [Google Scholar]
[16]. Sharma Rajesh, Jain Anil, Arya Achala, Chowdhary BR, Peak expiratory flow rate of school going rural children aged 5-14 years from Ajmer districtIndian Paediatr 2002 39:75-78. [Google Scholar]
[17]. Vijayan VK, Kappurao KV, Venkatesvan P, Sankaran K, Prabhakar R, Pulmonary function in healthy young adult Indian in MadrasThroax 1990 45:611-15. [Google Scholar]
[18]. Donnelly PM, Young TS, Peat JK, Woolcock AJ, What factors explain racial differences in lung volumes?Eur Respir J 1991 4:829-38. [Google Scholar]