Congenital Clubfoot (CC) is a malformation characterized by the varus position of the foot, and equine adducted forefoot, which can be fixed or rigid of varying degrees [1–3]. The most reliable treatment should be initiated within the first week of life, but there are some patients who present at hospital in a later stage or neglect treatment at a point. This special category also comprises children with recurrent clubfoot previously treated whose parents did not cooperate properly during aftercare. The difficulty of the treatment in this group of patients is due to stiffness, ossification and mature age of the joints [4–6].
The aim of this study was to present our experience in management of CC in children after walking age. Although CAP (Clubfoot Asesment Protocol) and other classification systems as Piranni or Mannes were reported to be relevant [7–9], we chose to perform the follow-up by using the Dimeglio score [8].
Material and Methods
Selection criteria
We conducted a cross-sectional study at the Clinic of Paediatric Surgery, Târgu- Mureâ, Romania, during January 2009 and May 2012. Processing of the cases was approved by the Ethical Committee of Clinical County Hospital of Targu-Mures, Romania. Written informed consent was obtained from each patient prior to began any research. The study group comprised all consecutive patients with CC, corrected by the same surgical team, who were diagnosed with congenital varus equinus CC, who at their first presentation were ≥ 1.5 years old. Patients who did not accept the proposed treatment or quit treatment before its completion were excluded from the study. Children with associated neurological abnormalities were also excluded. Thus, in the study 31 patients aged between 1.5 and 12 years old were included. Bilateral CC was diagnosed in 10 of the cases; a total of 41 feet were treated.
Management protocol
The study protocol includes the following steps: pre-operative evaluation of the patient using Dimeglio score, orthopedic correction, surgical intervention, follow-up and post-operative evaluation and 6 months post-operatively by using the same score [8]. The Dimeglio score aims four points of reducibility of the foot in different degrees from 0 to 4, the more flexible the position the lower the score. The four target positions are equinus, varus, supination and adductus. Beyond these, there are four possible scores, which are the followings: posterior crease, medial crease, cavus and deviant muscle function. Introduce these points to be awarded one point more. Thus, the maximum score is 20 and the minimum 0, the lower the score is the less the foot is affected, the score 0 representing a perfectly normal feet [8]. According to this score, patients can be classified in four groups, from benign to very severe CC [Table/Fig-1] [8].
The surgical correction of congenital clubfoot in 12-year old boy patient, using the Turco modified procedure - pre-operative (1A), intra-operative (1B) and post-operative view (1Cand 1D)

The focus of the pre-operatively evaluation was also placed on the age of patients and the structure of their bone tissue. Because the study group comprised children over the age of 1.5 years old, first step was to decide if the rigidity of the feet allows the conservative treatment.
In some of the cases, where it was possible, a casting device was applied in the pre-treatment phase; a femoral-cruro-podal plaster device in a position of maximum correction, changed every two weeks, for minimum 3 times, was used. The orthopedic treatment was performed according to the Ponseti method [10,11].
For the subsequently surgical correction, Turco modified procedure [12] was used [Table/Fig-2]. After surgery repeated plasters were performed to maintain the correction, in normal or hypercorrection position during 6 weeks. After 2 and 4 weeks the plaster device was changed. If used the Kirschner wires, they were removed 3 months follow surgery.
The aspect of the adapted Ponseti-Mitchelle orthosis-bar used for the aftercare protocol, in a case with congenital clubfoot.

In order to maintain the post-operatively correction, for minimum 2 years post-operatively, as a method of aftercare, we opted for the Bebax orthosis for a maximum of 13.5cm foot length, then Dennis-Browne orthosis and orthopedic shoes for walking. To improve the outcome, we use a combined orthosis, for children older than 3 years. It was about a combination of a plastic ankle-foot orthosis with a Dennis-Browne bar (adapted Ponseti-Mitchelle orthosis-bar), that was also applied for minimum 2 years post-operatively, respectively during the night, after this period [Table/Fig-3].
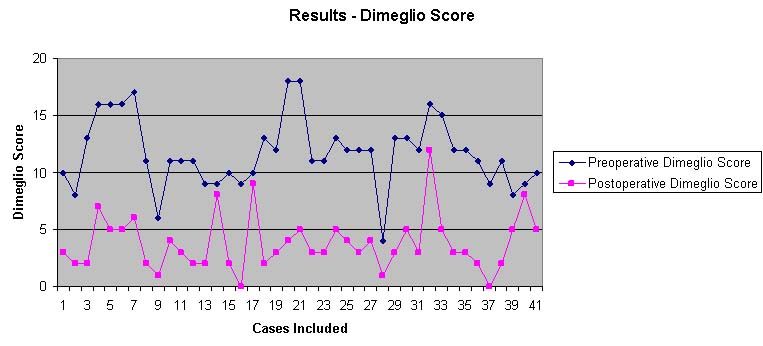
The pre-operatively and post-operatively Dimeglio score in the study group
Statistical Analysis
For data analysis, descriptive elements and inferential statistics were performed, using GraphPad Prism 5 software. Central tendency comparison was performed applying Wilcoxon test for paired data. We fitted a linear regression model with age as an independent variable and pre-operative Dimeglio score as dependent variable. The significant level of 0.05 was used.
Results
Clinicopathological characteristics
The median age of the 31 patients was 4.32±2.04, ranging between 1.5-12 years old. There were 11 (35.48%) girls, with the malformation present in 15 (36.58%) feet; and 20 (64.52%) male patients, with malformation present in 26 (63.42) feet. From the 41 feet comprised in the study, 34 (82.92%) were at their first presentation for orthopedic/surgical correction; the other 7 (17.08) cases were previously treated by other physicians, without success.
Dimeglio score
The average pre-operative Dimeglio score was 11.70±7.43, ranging from 4 to 18; it was not correlated with the age of patients (p=0.35; coefficient of determination r2=0.02246). From the 41 feet, only one was included in first Dimeglio category (benign), the other 40 feet (97.56%) being within categories II-IV, such as follows: 12 feet in category II (moderate), 21 feet in category III (severe) and 7 feet in category IV (very severe), respectively [Table/Fig-4]. Regarding the post-operative Dimeglio score, its average value was 3.80±0.96, ranging between 0 and 12. The average correction score was 7.90±3.45 [Table/Fig-5]. Post-operatively, the classification of CC revealed the following results: 35 feet in first category (benign), 5 feet of category II (moderate), and one foot of category III (severe), without cases included in category IV (very severe). All 6 of the feet (14.63%) with improper post-operative correction (category II/III) were pre-operatively included in the same group (category II/III).
Criteria of the Dimeglio score, used for pre-operatively and post-operatively evaluation (adapted from Dimeglio et al., [8])
| Dimeglio Score | 4 | 3 | 2 | 1 | 0 |
|---|
| Equinus C1 | 90° - 45° plantarflexion | 45° - 20° plantarflexion | 20° - 0° plantarflexion | 0° - 20° dorsalflexion | >20° dorsalflexion |
| Varus C2 | 90° - 45° varus | 45° - 20° varus | 20° - 0° varus | 0° - 20° Valgus | >20° valgus |
| Supination C3 | 90° - 45° supination | 45° - 20° supination | 20° - 0° supination | 0° - 20° pronation | >20° pronation |
| Adductus C4 | 90° - 45° adduction | 45° - 20° adduction | 20° - 0° adduction | 0° - 20° abduction | >20° abduction |
| Posterior Crease C5 | ° | ° | ° | present | absent |
| Medial Crease C6 | ° | ° | ° | present | absent |
| Cavus C7 | ° | ° | ° | present | absent |
| Deviant Muscular Function C8 | ° | ° | ° | present | absent |
| Dimeglio Score | 0-5 | 6-10 | 11-15 | 16-20 | |
| Category | I-Benign | II-Moderate | III-Severe | IV-Very severe | |
Quantification of the average preoperatory and postoperatory Dimeglio score and its criteria
| Parameters | Pre-operator average | Post-operator average | Average correction | p-value |
|---|
| Equinus C1 | 2.17±1.22 | 0.26±0.08 | 1.91±1.14 | <0.001 |
| Varus C2 | 2.24±0.96 | 0.43±0.16 | 1.81±1.05 | <0.001 |
| Supination C3 | 2.17±1.03 | 0.68±0.20 | 1.49±0.78 | <0.001 |
| Adductus C4 | 2.95±1.76 | 1.51±0.79 | 1.44±0.56 | <0.001 |
| Posterior Crease C5 | 0.73±0.21 | 0.09±0.02 | 0.64±0.07 | <0.001 |
| Medial Crease C6 | 0.53±0.11 | 0.12±0.05 | 0.41±0.20 | <0.001 |
| Cavus C7 | 0.60±0.15 | 0.39±0.13 | 0.21±0.05 | <0.001 |
| Deviant Muscular Function C8 | 0.29±0.01 | 0.29±0.08 | 0 | - |
| Dimeglio score | 11.70±7.43 | 3.80±0.96 | 7.90±3.45 | <0.001 |
Discussion
CC is difficult to be managed, especially in children after walking age, due to advanced ossification and maturation of the osteoarticular system [4–6]. In this group of patients the commonest therapy is the surgical correction that is difficult, lasts longer and has far more modest results compared to infants treated in their first weeks of life [11].
In our group of patients, the average correction was 7.90, in line to literature data that revealed an average correction rate from 6.5 to 11, the reported pre-operative and post-operative Dimeglio scores being also between 10.5-14.2 and 0.95-3.5, respectively [13,14]. Comparing our results obtained in children over 1.5 years with the previously published data considering the newborns, a slightly better post-operative Dimeglio score can be observed in the second category, from 3.80 to 0.6-2.4, respectively [15–17].
Although correction is usually proper and significantly improved, independently by the analyzed parameter, it seems that adductus (C4) is higher pre-operatively, compared with equinus (C1), varus (C2), or supination (C3). This is the reason why a special attention should be focused on the treatment that involves adductus correction. Deviant muscle function (C8) remains post-operatively unchanged, in older children; early diagnosis and treatment are mandatory to prevent it instead treat it. The aftercare protocol is also one of the physician-family responsibilities, essential for best correction.
Study Limitations
Quantification of Dimeglio score in a largest number of patients and its comparison with CAP and other classification systems such as as Piranni or Mannes could increase the study complexity. However, further researchers are necessary to evaluate the volume of leg muscles and other parameters for a longer period of time, these being some of the limitations of our study.
Conclusion
In children older than 1.5 years with unfavorable results following the conservative treatment, a proper correction of CC can be obtained by using the soft tissue release as surgical correction, without involving the mature bone. An adapted Ponseti-Mitchelle orthosis-bar can be successfully used post-operatively. However, intrauterine diagnosis and/or evaluation and treatment in first weeks of life are very important for the best results in the field. Dimeglio score can be succesfully used for evaluation, even in children after walking age.