Material and Methods
This study was conducted at Kasturba Medical College Hospital, Mangalore, from 1st June 2011 to 30th of September 2011. The hospital has a tertiary health care facility with a total of 1863 beds and an annual average of 78,175 and 2,29,468 admissions in the inpatient and outpatient sections respectively, in the past 2 years. All volunteering staff members who were working in the hospital units, who were involved in the management of critically ill patients (General Intensive Care Unit, adults), Coronary/cardiac ICU, Nephrology ICU, Neurology ICU, Paediatric ICU, Neonatal ICU, Post-operative ICU) and students (medical and nursing) who were on clinical rotation to the units, were conveniently included in the study. Approval was obtained by the research ethics committee of the institution for carrying out the study. A total of 200 consenting participants were included in the study. They were apprised with the details of the study. The age, sex, designation, MRSA carriage statuses of the individuals and treatment for the same, duration of stay in the critical care unit, the hospital wing to which they belonged to, the type of critical care unit and other relevant information about the consenting participants were obtained in a proforma which was made for this purpose. Swabs from both anterior nares of consenting participants were taken by using sterile cotton swabs which were moistened with sterile physiological saline and were transported to the microbiology laboratory unit of the hospital for bacteriological analysis. The samples were processed within 2 hours after their collection. The swabs were inoculated onto mannitol salt agar (MSA) plates and incubated at 37°C for 18-24 hours.
Any growth was identified as S. aureus by using standard procedures to study colony morphology, microscopic appearance on gram stained smears, catalase test, tube coagulase test and deoxyribonuclease test [14].
The isolated strains of S. aureus were screened for methicillin susceptibility by modified Kirby-Bauer method by using cefoxitin (30 μg) discs on Mueller-Hinton agar (MHA) by using an inoculum density which was equivalent to McFarland’s 0.5 standard (1.5 × 108 CFU/ml) [15]. Isolates which showed inhibition zone sizes of diameter ≤21 mm were considered as MRSA strains [16]. All isolates of S. aureus were also screened for vancomycin susceptibility test by the modified Kirby-Bauer method by using vancomycin discs (30 μg) on MHA which was incubated at 37°C for 24 hours. Isolates with inhibition zone sizes of diameter ≤15 mm were considered as vancomycin resistant. This was confirmed by detection of MIC by employing the broth dilution method [17]. Strains that showed an MIC of more than 4 μg /ml were considered as Vancomycin Resistant Staphylococcus aureus (VRSA).
Antibiotic susceptibility testing for all isolates of S. aureus was also done against other antibiotics like amoxicillin/clavulanic acid (20/10 μg), ciprofloxacin (5 μg) ceftriaxone (30 μg), cotrimoxazole (23.75/1.25 μg), erythromycin (15 μg), gentamicin (10 μg), linezolid (30 μg), penicillin (10 units) and teicoplanin (30 μg) by the modified Kirby-Bauer method. All antibiotic susceptibility tests were conducted by using S. aureus ATCC 25923, MRSA ATCC 29213 and MSSA ATCC 33591 as controls under similar conditions as were used for test strains. All antibiotic discs were procured from HiMedia Laboratories Pvt. Limited, India. Antibiotic sensitivity testing and interpretation of results were done according to CLSI guidelines [18]. Repeat samples were collected from the participants who showed a nasal carriage of MRSA after an interval of 15 days and they were processed in the same manner as has been mentioned above, for confirmation.
Statistical Analysis
A convenient sample technique was used for sample selection. Results were compiled, tabulated and all data were subjected to SPSS, version17.0 software statistical package for analysis. Association was done by using Chi-square test. A p-value of < 0.05 was considered as significant.
Results
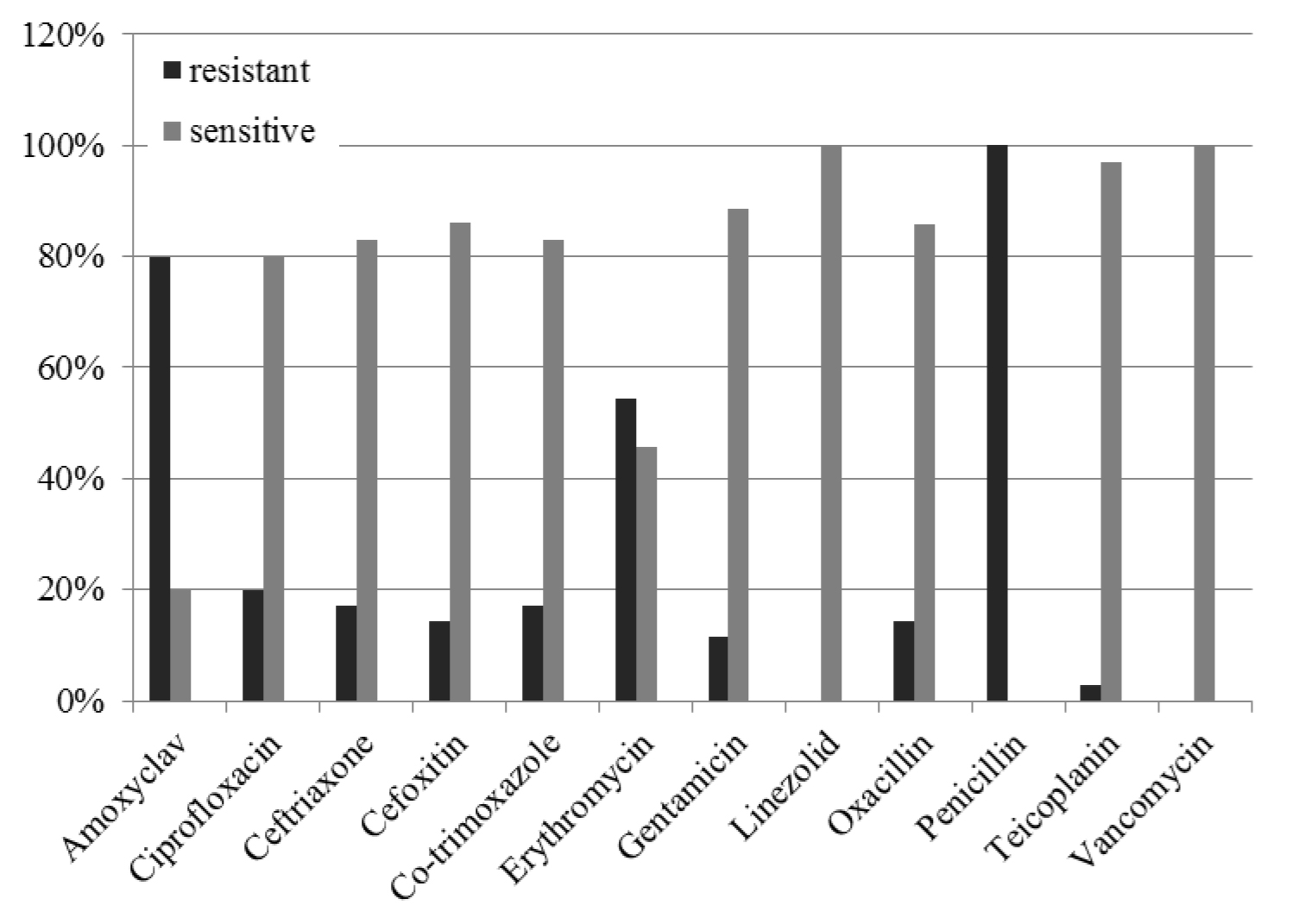
A total of 200 critical unit healthcare workers, whose ages ranged from 20-55 years (mean = 28.6 ± 7.5), were screened for MRSA. Thirty eight (19%) were males and 162 (81%) were females. Number of years of work in critical care units ranged between < 1 year to >5 years (median=0.5417). Staff nurses (110) and doctors (40) constituted a majority of subjects who were screened [Table/Fig-1]. Various species of bacteria, including MRSA, which were isolated from the anterior nares of the participants, have been shown in [Table/Fig-2]. Out of 200 healthcare workers who were screened, 35(17.5%) were positive for nasal carriage of S. aureus. Among these, 5 (14.3%) were MRSA carriers. Coagulase Negative Staphylococci (CoNS) were the predominant isolates (73%). Overall, MRSA nasal carriage rate was 2.5% in our study. Various hospital critical care units which were encompassed in the study, the number of participants which was examined and the type of S.aureus which was isolated, have been provided in [Table/Fig-3]. The distribution of S. aureus and MRSA carriage in relation to profession/cadre has been presented in [Table/Fig-4]. MRSA were isolated only from housekeeping personnel (13.3%) and from nursing staff (2.7%). All five participants from whom MRSA was isolated, were females. The antibiotic susceptibility patterns of S. aureus and MRSA isolates have been shown in [Table/Fig-5 and 6] respectively. While all isolates of S. aureus were resistant to penicillin, resistance to amoxyclav and erythromycin was 80% and 54% respectively. All the 5 isolates of MRSA showed a sensitivity rate of 100% to vancomycin and linezolid, 80% sensitivity to teicoplanin and gentamicin, 40% sensitivity to erythromycin and 20% sensitivity to ciprofloxacin. Further, the Minimum Inhibitory Concentration (MIC) of vancomycin in all the 5 isolates of MRSA was found to be < 2 μg /ml by broth dilution method. Repeat samples which were obtained from the participants confirmed carriage of MRSA and they expressed the same pattern of antibiotic susceptibility like that which was seen in earlier MRSA isolates.
Distribution of Participants
| Parameter | Description |
|---|
| Age in years(mean=28.6300,SD=7.51368) | Frequency (%) |
| <25 | 84(42) |
| 25-35 | 80(40) |
| 35 -45 | 28(14) |
| 45 -55 | 8 (4) |
| Sex distribution | |
| Males | 38(19) |
| Females | 162(81) |
| Number of years in critical care (Median=0.5417) |
| <1 | 129 (64.5) |
| 1 – 5 | 54 (27) |
| >5 | 17(8.5) |
| Designation |
| Doctor | 40(20) |
| Internee | 4 (2) |
| Staff Nurse | 110(55) |
| Hospital auxiliary | 6 (3) |
| Student nurse | 22(11) |
| Housekeeping | 15(7.5) |
| Physiotherapy | 3(1.5) |
Nature of organisms isolated from anterior nares
| Organisms Isolated | Frequency (%) n = 200 |
|---|
| Staphylococcus aureus | 35 (17.5) |
| CONS | 146 (73.0) |
| Others | 10 (5.0) |
| No growth | 9 (4.5) |
Hospital Critical care units related S. aureus & MRSA carriage status
| Critical care units | No. sampled | No. positive for S. aureus | No. positive for MRSA |
|---|
| Gen ICU | 70 | 12 | 2 |
| PICU | 38 | 8 | 1 |
| NICU | 52 | 8 | 1 |
| POST OP | 10 | 1 | 1 |
| CICU | 21 | 5 | 0 |
| NEPHROLOGY ICU | 2 | 1 | 0 |
| NEUROLOGY ICU | 7 | 0 | 0 |
GenICU: Intensive Care Unit (for adults); PICU: Paediatric Intensive Care Unit NICU: Neonatal Intensive Care Unit; CCIU: Cardiac Intensive Care
Profession/cadre related distribution S. aureus and MRSA carriage status
| Designation | No. sampled (%) n=200 | No. positive for S. aureus | No. positive for MRSA |
|---|
| Doctor | 40 (20) | 13 | 0 |
| Internee | 4 (2) | 0 | 0 |
| Staff Nurse | 110 (55) | 15 | 3 |
| Hospital auxiliary | 6 (3) | 0 | 0 |
| Student nurse | 22 (11) | 3 | 0 |
| Housekeeping | 15 (7.5) | 4 | 2 |
| Physiotherapist | 3 (1.5) | 0 | 0 |
Antibiotic susceptibility profile of S. aureus isolates
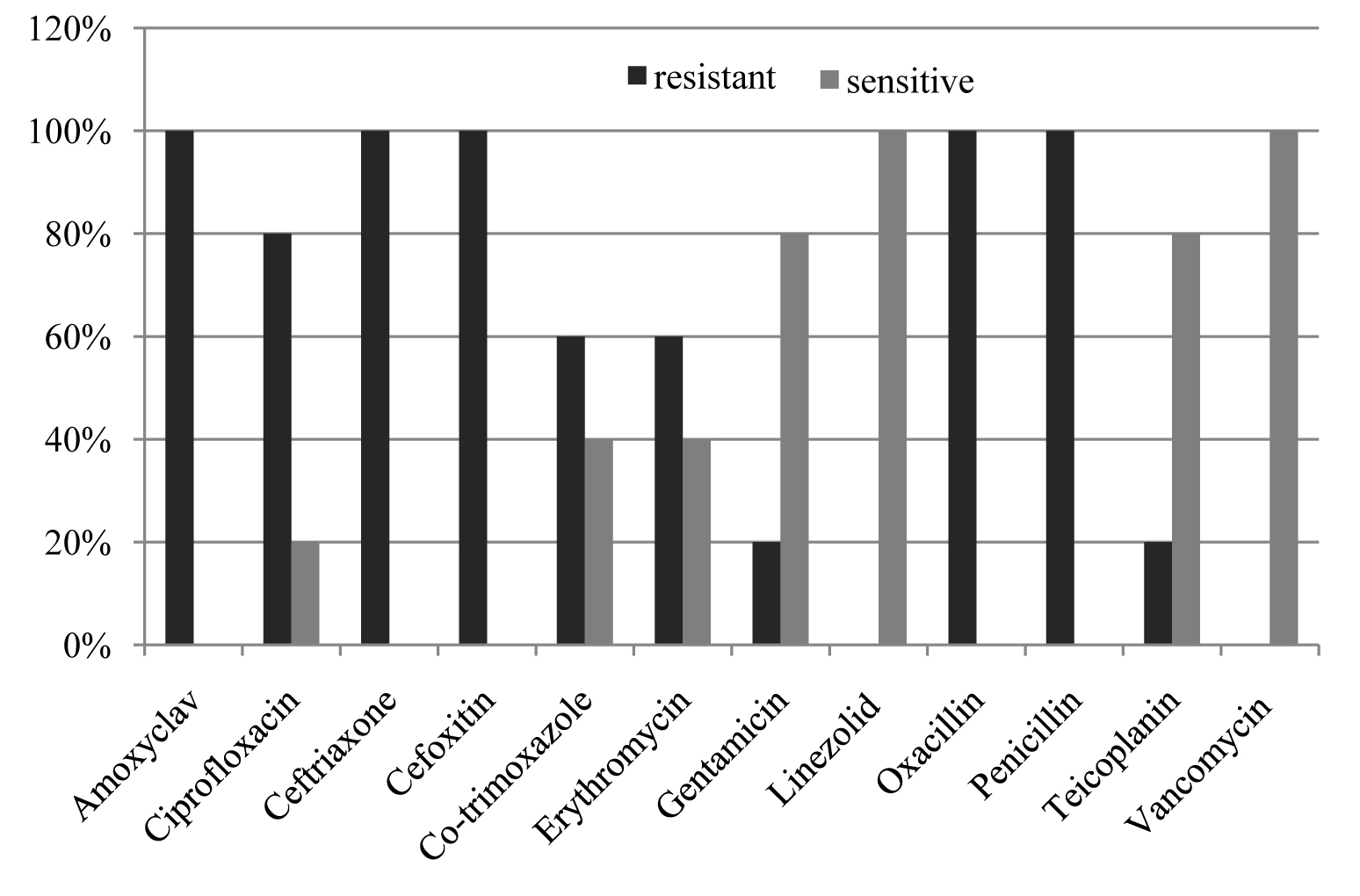
Antibiotic susceptibility profile of MRSA isolates
Discussion
It is necessary to detect the MRSA carriers among health care workers (HCWs) in hospitals, particularly those who work in the critical care areas. These individuals act as a potential source of infection to their patients, causing nosocomial infections and thereby, causing extended stays in the hospital. The best methods which can be used for controlling this, are regular screening of the HCWs and taking the appropriate preventive measures. The prevalence of MRSA varies between institutions and geographic areas. The differences in the study design, such as the sample size and the method which is employed for MRSA detection, may account for the disparity in the carriage rate. Literature search done by Albrich and Harbarth from January 1980 to March, 2006, which involved 127 investigations and screening of 33, 318 health-care participants, revealed that 4.6% of the health care personnel were either infected or colonized with MRSA [13]. They also reported 41 studies which involved 10,589 participants, which revealed a carriage rate of 23.7% of methicillin sensitive S.aureus. Indian studies revealed an MRSA carriage rate of 1.8% from Pondicherry [19], that of 6.6% from Delhi [20] and that of 2% from Madurai [21]. A MRSA carriage of 2% was reported from Nepal [22]. Outside India, a very high MRSA nasal carriage rate of 38.9% was reported from Nigeria [23]. According to the findings of our study, nasal carriage of S. aureus among healthcare workers who were involved in the management of critically ill patients was 17.5%. The S.aureus carriage was particularly high among doctors (32.5%) and housekeeping personnel (26.7%), followed by nursing staff (13.6%) and student nursing trainees (13.6%). However, the MRSA carriage rate among health care personnel who were involved in the critically ill patients was only 2.5%., which was significantly lower than that of 4.6% (p < 0.01) which was reported in a meta-analysis of 127 investigations which was done around the world, which involved screening of 33,318 healthcare workers the world over [13]. Our finding for MRSA was marginally high as compared to the earlier report (1.8%) which was obtained from Pondicherry [19], but it was significantly low as compared to the findings of studies which were carried out in other two parts of India, Assam (11.48%) and Bangalore (10%) respectively [24,25]. We have effectively functioning Hospital Infection Control Committee policies, which may be responsible for absence of MRSA carrier state among doctors, internees, student auxiliary staff, student nursing trainees and physiotherapists. However, we cannot ignore the fact that a high MRSA carriage rate was observed among female housekeeping staff (13.3%), followed by a low carriage rate among female nursing staff (2.7%). Repeated isolation of MRSA from these staff confirmed the findings. This finding cannot be ignored, as according to unpublished data from the medical records of our hospital, the occurrence of hospital acquired MRSA infection was between 22-25%. This underscores not only the need to develop more stringent hospital infection control policies, but also to create awareness among housekeeping and nursing staff by educating them, to eradicate MRSA carriage. Further, such actions would help in the prevention of MRSA transmission to their family members [26,27]. Moreover, the financial burden of handling such nosocomial and community spreads of MRSA infection would be considerable and hence, MRSA has been considered a public health issue with economic consequences [28]. Molecular typing was not conducted on the MRSA strains in our study and therefore, it was not possible to establish as to whether strains were shared in a particular hospital unit or across the units. Therefore, it may be desirable to conduct a molecular typing of MRSA in the epidemiological perspective. All five MRSA isolates were sensitive to both vancomycin and linezolid, though our hospital records documented 8% vancomycin intermediate S. aureus (VISA). They also showed variable susceptibility patterns to other antibiotics such as teicoplanin and gentamicin sensitivity (80%), erythromycin sensitivity (40%) and ciprofloxacin sensitivity (20%). The absence of vancomycin resistance of MRSA, which is compelled by its low toxicity and easy availability, connotes that not only can it be used in eradication of MRSA carrier state of healthcare workers, but also for treatment of cases which result from outbreaks of MRSA infection. Mupirocin is the topical antibiotic of choice for the decolonization of MRSA, as it is very effective for this use [29]. In our study, as the MRSA carriers did not give their consents, we could not try decolonization with mupirocin. Many of the reports on vancomycin resistance, which have been made by private diagnostic laboratories, are based on disc diffusion method. Vancomycin, being a macromolecular antibiotic, doesn’t properly diffuse through the agar. As a result, the reporting on VISA or VRSA, based on the results of disc diffusion alone, may not be acceptable [30]. Agar dilution or broth dilution technique is a more appropriate method for finding the MIC and hence, for determining vancomycin susceptibility. Our MRSA strains were found to be sensitive to vancomycin, both by disc diffusion and broth dilution methods. Mannitol Salt Agar was found to be very useful for the quick identification of S. aureus. However, the option of using oxacillin blood agar for selective isolation of MRSA is always useful. Usage of cefoxitin discs was found to be convenient over that of oxacillin discs for the determination of MRSA.
Conclusion
In our study, nasal carriage of S. aureus among healthcare workers who were involved in the management of critically ill patients was 17.5%. The S.aureus carriage was particularly high among doctors (32.5%) and housekeeping personnel (26.7%). However, the MRSA carriage rate among health care personnel who were involved in the critically ill patients was only 2.5%. We have an effectively functioning Hospital Infection Control Committee, the policies of which may be responsible for absence of MRSA carrier state among doctors, internees, student auxiliary staff, student nursing trainees and physiotherapists. However, we cannot ignore the fact that a high MRSA carriage rate was observed among female housekeeping staff (13.3%), followed by a low carriage rate among female nursing staff (2.7%). This underscores the fact of creating awareness among housekeeping and nursing staff by educating them, to eradicate MRSA carriage.
GenICU: Intensive Care Unit (for adults); PICU: Paediatric Intensive Care Unit NICU: Neonatal Intensive Care Unit; CCIU: Cardiac Intensive Care