The Foramen Ovale Morphometry of Sphenoid Bone in South Indian Population
Jyothsna Patil1, Naveen Kumar2, Mohandas Rao K.G.3, Swamy Ravindra S.4, Somayaji S N.5, Satheesha Nayak B.6, Sapna Marpalli7, Ashwini L.S.8
1 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
2 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
3 Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
4 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
5 Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
6 Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
7 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
8 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mr. Naveen Kumar, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, Karnataka, India.
Phone: +919880548636, Fax: 91-820-2571905,
E-mail: naveentonse@gmail.com
Background: The foramen ovale is an oval opening in the greater wing of sphenoid bone transmitting the mandibular nerve as its major content. It serves as an important landmark for neurosurgeons in certain procedures as to gain access to trigeminal nerve. Therefore, its topographic position in relation to adjacent bony landmarks provides useful tool during these procedures.
Aim: To analyse the morphometric measurements of the foramen ovale among South Indian population.
Material and Methods: Morphometric analysis was carried out on 104 foramina ovalia of 52 dry human skulls from South India. Following dimensions of foramen ovale were measured: antero-posterior length, transverse width, distance (d1) from tubercle of root of zygoma to the centre of the foramen (CF) and distance (d2) from the midline of the base of the skull to CF.
Results: The mean antero-posterior length was 7.0±2.17mm on right side and 6.8±1.40mm on left side, mean transverse width was 5.0±0.42mm and 4.70±0.91mm on right and left side respectively. Mean d1 was 32.58±1.72mm on right side and 32.75±1.76mm on left side. Mean d2 was 25.83±1.26mm on right side and 25.08±1.31mm on left side.
Conclusion: Regional variations in the morphometric measures may be useful in neurosurgical procedures like administration of anaesthesia involving the mandibular nerve.
Canalis ovalis, Morphometry, Sphenoid bone, Mandibular nerve
Introduction
The foramen ovale is an oval shaped opening, placed obliquely in the base of the skull. It is situated in the greater wing of sphenoid bone, close to the upper end of posterior margin of lateral pterygoid plate, medial to foramen spinosum and lateral to the foramen lacerum [1]. It connects the middle cranial fossa to the infratemporal fossa and transmits the mandibular nerve, accessory meningeal artery, lesser petrosal nerve and emissary vein. Understanding the accurate location & dimensions of foramina ovalia plays a vital role during certain diagnostic procedures like electroencephalographic analysis, microvascular decompression by percutaneous trigeminal rhizotomy and percutaneous biopsy of cavernous sinus tumours [2,3]. Prior knowledge of topography and possible variations in the position of the ovale prevent possible injury to the trigeminal nerve during these approaches.
Thus, marking exact location of foramen ovale by means of various measurements, in relation to structures around the foramen ovale in advance of various intervention procedures, would be helpful beforehand. Information related to regional or ethnic descrepancies in the morphometric analysis of the foramen ovale from the available literature, prompted us to undertake present study. This study can be helpful for the clinicians and surgeons to facilitate the easy localization of the foramen ovale in South Indian population.
Material and Methods
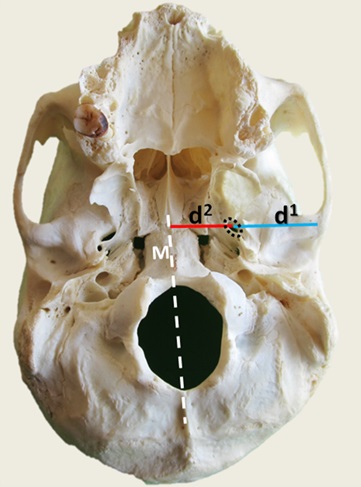
Present study was conducted by examining 104 foramina ovalia using 52 dry adult human skulls of South Indian origin. Skulls which were damaged, fractured or deformed at the surroundings of foramen ovale were excluded from the study. Existence of the foramen ovale was ascertained bilaterally by observing the posterior part of the greater wing of the sphenoid bone along with its normal topographic position. Antero-posterior length and the width of the foramen ovale were measured. Distance from the centre of the foramen ovale (CF) to the tubercle of root of zygoma (d1) and distance from the CF to the midline of the base of the skull (d2) was also measured bilaterally using divider measurement device [Table/Fig-1]. Mean values of these measurements were calculated and compiled. Various measurements between right and left side were analysed statistically, using SPSS (V16) by testing student’s ‘t’ test method and p-value < 0.05 was considered statistically significant.
Basicranium of a skull indicating the different measurements used in the study to analyse the morphometry of the foramen ovale. M- midline of base of skull, d1-Distance from centre of the foramen to the root of the zygoma, d2- Distance from the centre of the foramen ovale to midline of the skull (M). Dotted circle represents the position of foramen ovale
Results
The mean antero-posterior length of foramen ovale was 7.0±2.17mm on right side and 6.8±1.40mm on left side, its mean transverse width was 5.0±0.42mm on right side and 4.70±0.91mm on left side, mean of distance from the CF to the zygomatic arch (d1) was 32.58±1.72mm on right side and 32.75±1.76mm on left side, mean distance from the CF to the mid-line of base of the skull (d2) was 25.83±1.26mm on right side and 25.08±1.31mm on left side [Table/Fig-2]. Though the statistical analysis of morphometric measurements between right and left side was found to be insignificant, the results of both sides marks the evidence of asymmetry in the morphometry of the foramina ovalia.
Showing the detailed results of morphometric measurements of foramen ovale
| Min-Max Value (in mm) | Mean Value (in mm) | Std Deviation (±) |
|---|
| Length (R) | 5.0-11.0 | 7.0 | 2.17 |
| Length (L) | 4.0-10.0 | 6.8 | 1.40 |
| Width (R) | 3.5-5.0 | 5.0 | 0.42 |
| Width (L) | 4.0-6.0 | 4.70 | 0.91 |
| d1 (R) | 29.0-42.0 | 32.58 | 1.72 |
| d1 (L) | 29.0-42.0 | 32.75 | 1.76 |
| d2 (R) | 22.0-28.0 | 25.83 | 1.26 |
| d2 (L) | 22.0-28.0 | 25.08 | 1.31 |
(R- right, L- left, d1 - Distance from the centre of the foramen ovale (CF) to the tubercle of root of zygoma, d2- distance from the CF to the midline of the base of the skull)
Discussion
Numerous studies on the morphometric and developmental aspect of foramen ovale have been done worldwide. Developmental study in Japan showed an average maximal length of foramen ovale to be 7.48 mm and average minimal length to be 4.17 mm. However, authors did not observe any statistical differences between right and left side morphometry [4]. A German study showed length of foramen ovale to be 7.2mm and its width to be 3.7mm in an adult skull [5]. Fluoroscopically-assisted laser targeting of the foramen ovale conducted in New York showed mean length of 6.9mm on right side and 6.8mm on left side. Average width of foramen ovale was 3.4mm on right side and 3.8mm on left side [6]. These findings appear to be low compared to that of other studies reported earlier. In the present study, maximum length of foramen ovale was 9.5mm and minimum length was 5.0mm, with the mean of 7mm. These values are very close to the results of study done by Arun in Nepalese population [7], in which the maximum length of foramen ovale was reported to be 9.8mm and minimum was 2.9mm. Yanagi S. [4] and Lang J et al., [5] in their studies inferred that the average length of foramen ovale was about 7.2mm in adults. This value also confirms our findings. More than 24% of the foramina ovalia studied were with the average length 7.0mm. As far as width of the foramen was concerned, the current study reports the maximum width of foramen ovale as 5mm and the minimum width as 3.5mm, with average width being 5mm. Width of more than 57% of foramina ovalia was within the range of 3.0 - 3.5mm and the rest were either above or below this range.
Length and width of the foramen ovale may be insignificantly higher in males than in females [8]. Bilateral asymmetry of foramen ovalia has been reported by Jain and Jain [9]. Our study revealed the bilateral asymmetry of the foramina ovalia in the size, shape and distance from the midline. Thus, providing another clue to prove that the skulls are bilaterally asymmetrical. Rarely, typical foramen ovale divided into medial and lateral compartments by an oblique bony lamina, apparently continuing with the lateral pterygoid plate. The lateral compartment of which is referred to as oval canal or canalis ovalis [10]. The medial compartment constituted a foramen, which could be regarded as a topographic counterpart to the foramen ovale proper. Foramen ovale with two compartments with the transmission of a part of mandibular nerve in each compartment was observed by Krmpotic [11]. The incidence of division of foramen ovale into compartments was reported to be 4.5% [12].
Variation in the dimension and shape of foramen ovale can be explained on the basis of development. Sphenoid bone develops from both intramembranous and endochondral ossification with the pre-sphenoid and post-sphenoid centres. While both centres contribute to the basisphenoid (body) part and lesser wing, the post-sphenoid centre forms the greater wing and pterygoid process of sphenoid bone. The foramen ovale is situated at the posterior border of greater wing of sphenoid bone [13]. When the mandibular nerve becomes enclosed by the cartilage, the foramen ovale is formed. However, in early stage of embryogenesis (22nd week) this foramen can be demonstrated as a discrete ring-shaped opening in the area of non-ossified cartilagenous part, which in later life (3 years after birth) can be renowned as definitive foramen [4]. The bony overgrowth during its developmental process is often evidenced by the appearance of tubercle, bony spur, and bony plate surrounding the foramen ovale. Thus, the occasional presence of an accessory foramen beside the ovale is probably due to interaction of different parts of membrane bone and the venous plexus from the middle meningeal veins to pterygoid venous plexus [14].
Narrow size of foramen ovale is a common manifestation in the clinical scenario of Paget’s disease or osteopetrosis [15]. Unusual position of foramen ovale and persistence of neighbouring bony structures may manipulate the anatomical organization of the nerves which are transmitted through the foramen. This, often results in the lateral disposition of mandibular nerve resulting in the entrapment of its branches between bony structure and the neighbouring muscles which might lead to neuralgia [11]. FNAC through foramen ovale is done to diagnose squamous cell carcinoma, meningioma and also for deep lesions biopsy [16].
Localizing the exact position of foramen ovale by measuring the distance from the root of the zygoma to its centre becomes vital during penetrating procedures to reach the structures passing through it, as any failure in this may often lead to the injury to the structures in and around the foramen, including haemorrhage in the temporal lobe of the brain [17]. Thus, along with skin markers and image intensifier techniques, these measurements for locating foramen ovale can be used as additional aid for above said surgical invasive procedures [17–19]. However, it should be kept in mind that, these parameters are not similar in all individuals as the location of zygomatic point in Korean population and in population of certain western countries often varies [20].
Conclusion
Morphometric analysis from the current study mostly falls well within the range of other study results pertaining to Asian population. Though, the morphometric measurements of foramen ovale of right and left side are statistically insignificant, the results of both sides mark the evidence of asymmetry in the morphometry of the foramina ovalia in South Indian population. As the morphometric aspects of the foramen ovale vary in different countries and regions, knowledge of specific regional morphometric analysis of foramen ovale becomes necessary to aid in respective clinical and surgical procedures.
(R- right, L- left, d1 - Distance from the centre of the foramen ovale (CF) to the tubercle of root of zygoma, d2- distance from the CF to the midline of the base of the skull)
[1]. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, Gray’s Anatomy: The Anatomical Basis of Clinical Practice 2008 Vol. 119840th ed.LondonElsevier, Churchill Livingstone:415 [Google Scholar]
[2]. Gerber AM, Improved visualization of the foramen ovale for percutaneous approaches to the Gasserian ganglion: Technical noteJ Neurosurg 1994 80:156-59. [Google Scholar]
[3]. Gusmao S, Oliveira M, Tazinaffo U, Honey CR, Percutaneous trigeminal nerve radiofrequency rhizotomy guided by computerized tomography fluoroscopy: Technical noteJ Neurosurg 2003 99:785-86. [Google Scholar]
[4]. Yanagi S, Developmental studies on the foramen rotundum, foramen ovale and foramen spinosum of the human sphenoid boneThe Hokkaido Journal of Medical Science 1987 62(3):485-96. [Google Scholar]
[5]. Lang J, Maier R, Schafhauser O, Postnatal enlargement of the foramina rotundum, ovale and spinosum and their topographical changesAnatomischer Anzeiger 1984 156(5):351-87. [Google Scholar]
[6]. Landl MK, Walter Grand, Trigeminal Neuralgia: Fluoroscopically –Assisted Laser Targeting of the Foramen Ovale: Technical NoteMinrad International Inc 2005 [Google Scholar]
[7]. Arun S K, Some observations of the foramina ovale and spinosum of human sphenoid bone 2006 55:1 [Google Scholar]
[8]. Burdan F, Umlawska W, Dworzanski W, Klepacz R, Szumilo J, Staroslwska E, Anatomical variances and dimensions of the superior orbital fissure and foramen ovale in adultsFolia Morphol 2011 70(4):263-71. [Google Scholar]
[9]. Jain KK, Jain BK, Asymmetry in the skullActa Anat (Basel) 1979 104(3):349-52. [Google Scholar]
[10]. Skrzat J, Walocha J, Srodek R, Nizankowska A, An atypical position of the foramen ovaleFolia Morphol 2006 65(4):396-99. [Google Scholar]
[11]. Krmpotic Nemanic J, Vinter J, Hat J, Jalsovec Mandibular neuralgia due to anatomical variationEur Arch Otorhinolaryngol 1999 256:205-08. [Google Scholar]
[12]. Reymond J, Charuta A, Wysocki J, The morphology and morphometry of the foramina of the greater wing of the human sphenoid boneFolia Morphologica 2005 64(3):188-93. [Google Scholar]
[13]. Lang J, Clinical Anatomy of the Head, Neurocranium, Orbit and Craniocervical Region 1883 BerlinSpringer-Verlag [Google Scholar]
[14]. James TM, Presley R, Steel FL, The foramen ovale and sphenoidal angle in manAnat Embryol (Berl) 1980 160:93-104. [Google Scholar]
[15]. Kim JS, Lee MK, Bae YH, Kim DJ, Trigeminal neuralgia in a patient with osteoporosisJ Korena Neurosurg Soc 1998 27:1147-51. [Google Scholar]
[16]. Desai SD, Hussain SS, Muralidhar P S, Thomas ST, Mavishettar GF, Haseena S, Morphometric analysis of Foramen ovaleJ. Pharm. Sci. & Res 2012 4(7):1870-71. [Google Scholar]
[17]. Rovit RL, Murali R, Jannetta PJ, Percutaneous radio-frequency thermal coagulation of the Gasserian ganglion, Trigeminal Neuralgia 1990 BaltimoreWilliams & Wilkins:109-36. [Google Scholar]
[18]. Nugent GRL, Wilkins RH, Rengachary SS, Trigeminal neuralgia: Treatment by percutaneoud electrocoagulation in Neurosurgery 1996 vol 3ed-2McGraw-Hill:3945-51. [Google Scholar]
[19]. Tew JM, Taha JM, Treatment of trigeminal and other facial neuralgias by percutaneous techniques in Youmans JR (ed 4)Neurological surgery 1996 vol 5PhiladelphiaSaunders:3386-03. [Google Scholar]
[20]. Sung H H, Myung K L, June W P, Jae E L, Chang W C, Dae J K, A morphometric analysis of the foramen ovale and the zygomatic points determined by a computed tomography in patients with idiopathic trigeminal neuralgiaJ. Korean Neurosurg soc 2005 38(3):202-5. [Google Scholar]