Rectus Sternalis muscle, an uncommon anatomical variant of the chest wall musculature, is regularly present in lower animals and is occasionally detected in humans. Although first formal description of this muscle was given by Dupuy in 1726, it was demonstrated a century earlier by Carbollius in 1604. Since then, many cases with Rectus Sternalis muscle have been reported. Yet, this muscle has not gained equal importance as other muscles of thorax. The appearance of this muscle is in the form of superficial vertical strip, which is sternal or parasternal in position. CT and MR imaging are diagnostic when they show the longitudinal extent of the muscle, which lies anterior to the medial margin of the pectoralis major muscle. If clinicians are not aware of its occasional presence, this muscle can be confused with an abnormal mass. In radiotherapy and surgery, lack of knowledge on Rectus Sternalis can cause negative changes in prognosis of patient. Sufficient knowledge on this muscle may help in making a better diagnosis and it can decrease complications.
Cadaveric studies have shown the equal presence of this muscle in approximately 5-8% of both males and females. Variations in its incidence have been reported in different ethnic groups. Rectus Sternalis is twice as often unilateral as it is bilateral [1]. Many authors assumed the Sternalis muscle to be derived from neighbouring muscles, such as pectoralis major [2], rectus abdominis, sternocleidomastoid, panniculus carnosus and external oblique [3].
Cases have been reported by different authors with various names of this muscles i.e. Sternalis, Rectus thoracis, Presternalis, Muscularis sternalis, Parasternalis, Episternalis, etc. Various names create confusions. One universal name “Rectus Sternalis” should be fixed for this muscle, as it is a type of straight muscle which has been placed in close relation to the sternum. An interesting cadaveric study which was done on the details of this muscle has been presented here, to establish the importance of Rectus Sternalis.
Material and Methods
During a time period of three years (2010 to 2013), 30 properly embalmed cadavers were dissected in dissection hall of Anatomy Department, S.M.S. Medical College, Jaipur, Rajasthan. Every year, 10 cadavers were dissected routinely as a part of medical education in this college. For a sample of 30 cadavers, a span of three years was considered for this study. During the dissections of pectoral regions of these cadavers, presence of Rectus Sternalis was carefully observed. This study was conducted on the cadavers who were dissected routinely in the dissection hall.
Among 30 cadavers, a variation was observed in the anterior chest wall musculature, as a vertical strip of muscle in a single cadaver. This variation was studied and it was identified as Rectus Sternalis muscle. Photographs and details of this muscle were taken after cleaning the dissected region.
Results
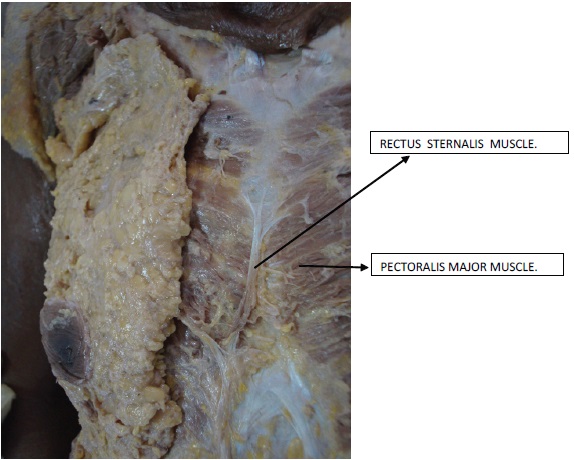
A unilateral, right-sided Sternalis muscle was found in a cadaver during routine dissections of pectoral regions which were done on 30 properly embalmed cadavers of Indian origin [Table/Fig-1]. This was a rare case of Rectus Sternalis. The muscle was found as a unilateral vertical strip which was present parasternally on the right side in the pectoral region. The fibres of this muscle were at right angles to the fibres of pectoralis major. The muscle was superficial to pectoralis major muscle and its fascia. It clearly had three visible parts [Table/Fig-2], 1. tendinous upper part of muscle (insertion), 2. lower fleshy belly of muscle, 3. fibres of Rectus Sternalis which reached upto fascia of external oblique (origin).
Right-sided unilateral Rectus Sternalis
Right-sided unilateral Rectus Sternalis with its different parts.
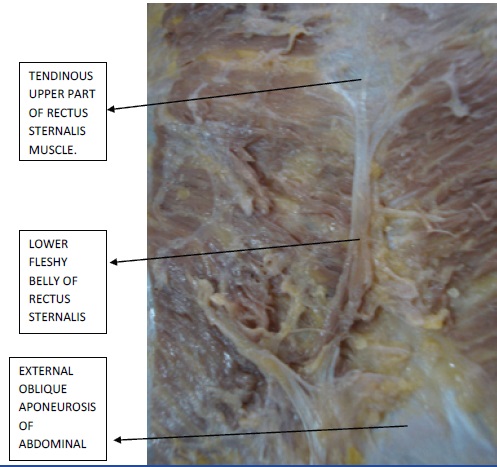
Upper half of the muscle was in the form of 2-3 slips and it was tendinous. These slips reached up to pectoralis major, mainly towards right side. The lower, fleshy and flat ribbon like end was attached to superficial surface of right pectoralis major muscle by fascia, which reached up to the level of xiphisternal joint. This end was 4.2 cm wide and it was very close to the origin of right rectus abdominis muscle and external oblique aponeurosis. Fibres of Rectus Sternalis were not in continuity with fibres of other muscles.
It was difficult to show the innervation source of Rectus Sternalis muscle in this cadaver, as during separation of the lateral margins of muscle, the twigs from the pectoral nerve, which could be easily be confused with the connective tissue, were almost removed or damaged.
Discussion
Rectus Sternalis is one of the important muscles of anterior chest wall musculature. The location of muscle and direction of fibres suggest that this muscle may help in elevating the lower chest wall.
Occurrence of Rectus Sternalis is rare but it is not the rarest and it has racial and regional variations. Sarikcioglu L et al., [4] reported its incidence to be 4-7% in white population, 8.4% in black population, 11% in Asian population, 1% in Taiwanese population and 9.3% in Turkish population. In Indian population, its incidence is 5-8% equal in both genders. Mehta V et al., [5] discussed a more common unilateral occurrence of this muscle and lack of acquaintance of the clinicians with this muscle variant. An incidence of 4–8% has been found earlier in Indian subjects [6,7]. The present study however, reported a lower incidence of 3.3%. Rectus Sternalis is a rare but normal anatomical variant in the anterior chest wall musculature in the cadavers of Indian origin.
Reported size of Rectus Sternalis was different in different cases. In cases with a partial or complete congenital absence of Pectoralis Major muscle, a significant size of Rectus Sternalis has been observed. Muscles were wider at their caudal ends in case reports of Mehta V et al., [5] (2.2 cm) and Kulkarni DU et al., [8] (5.2 cm), these findings are similar to present finding. In present study, upper end of muscle was in the form of 2-3 slips and it was tendinous, while the lower end was wider (4.2 cm) and fleshy.
Although a unilateral Rectus Sternalis was observed in present cadaveric study, bilateral muscles have also been reported by many authors. Its unilateral presence has been reported to be 4.5%, while its bilateral presence has been reported to be 1.7% [9]. Sarikcioglu L et al., [4] reported presence of three Rectus Sternalis muscles in a single cadaver, one on right side and two on left side. According to them, it is a composite type of muscle. Unilateral presence were reported by Mehta V et al., [5] and Kulkarni DU et al., [8] in their case reports.
Origin and insertion of Rectus Sternalis muscle is still a debatable topic. According to some reporters, it originates from sternum or interclavicular region and inserts into either rectus sheath, costal cartilage, or lower ribs. In Gray’s anatomy [10] this muscle is described as a superficial vertical slip, or slips which ascend from lower costal cartilages and the rectus sheath to blend with sternocleidomastoid muscle or to attach to the upper sternum or costal cartilages. In the present cadaveric study, the latter view held stronger, since the muscle had a tendinous upper part and a lower fleshy belly.
There are different views on nerve supply and development of Rectus Sternalis. It may be derived from primitive ventral longitudinal muscle sheet, which also gives rise to rectus abdominis and sternocleidomastoid muscle. This fact is supported by the findings of some studies, that Rectus Sternalis muscle fibres are continuous most of the times with either sternocleidomastoid or rectus abdominis or both. According to Sadler, Rectus Sternalis is a part of a ventral, longitudinal column of muscles which arise at the ventral tips of hypomere [3]. It could be the separated fibres of pectoralis major, as was indicated by its nerve supply from twigs of pectoral nerve. In some cases, muscle was accompanied by a partial deficiency of pectoralis major. In present case report, nerve supply was the twigs from the pectoral nerve. This finding supports the opinion of derivation of Rectus Sternalis muscle from pectoralis major [11].
Rectus Sternalis may represent the remains of ‘panniculus carnosus’[12], which is supported by its position, which is superficial to pectoral fascia and has a nerve supply from anterior cutaneous branches of intercostal nerves [9]. Sarikcioglu L et al., [4] also observed similar findings on nerve supply.
Rectus Sternalis has clinical significance. It can create alterations in ECG. In routine mammography, the superficial location of Rectus Sternalis may be mistaken for a tumour on initial investigation or as a recurrence of a cancer during post-treatment checkups [5,9,13]. This confusion can be cleared by CT and MR imaging. During mastectomy, Rectus Sternalis is a rare muscle which is encountered in the subcutaneous plane. Hence, the knowledge on this muscle is important, for a surgeon to identify it early during the decision making of an appropriate dissection plane. Extension of breast tissue deep to the muscle should not be neglected during surgery. In Radiation therapy, the depth at which internal mammary nodes are irradiated may also vary in the presence of this muscle. Rectus Sternalis can be used as a muscle flap in anterior chest wall, head and neck, and in breast reconstructions [14].
Ideally, to know the incidence of Rectus Sternalis, a cadaveric study should be conducted on a large sample size. For this, dissection of pectoral regions of all cadavers of Indian origin, which are performed at all medical colleges in a defined period of time, should be considered at a time. This task seems to be a difficult one. Alternatively, the results which are obtained from different studies which are conducted on smaller samples, can be considered simultaneously, to draft a single study. For this, smaller studies which are similar to present study should be conducted at different medical colleges in India.
Though present study was a small cadaveric study which was done on 30 cadavers, it provided baseline information on the incidence of Rectus Sternalis among the cadavers of Indian origin. This study can be a reference for other similar studies.
Conclusion
Rectus Sternalis is a rare superficial misplaced muscle tissue, arising from variable sources in a localized region at the anterior thorax, and knowledge on it is important for performance of interventional and diagnostic procedures which are related to this region. Negligence of this muscle can cause negative changes in prognosis of patient. New advances in reconstruction surgery by using Rectus Sternalis muscle flap are possible.