The Volume of the Caudal Space and Sacral Canal in Human Sacrum
Adil Asghar1, Shagufta Naaz2
1 Assistant Professor, Department of Anatomy, HIMSR, Jamia Hamdard, New Delhi-110062, India.
2 Assistant Professor, Department of Anaesthesiology, HIMSR, Jamia Hamdard, New Delhi-110062, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Adil Asghar, Assistant Professor, Department of Anatomy, HIMSR, Jamia Hamdard, New Delhi-110062, India.
Phone: 9911225915, 7838117314,
E-mail: dr_adilasghar2003@yahoo.co.in, dradilasghar2009@gmail.com
Introduction: Caudal block is now- a –days a commonly used procedure for pain management and regional anaesthesia. The optimum volume of drugs required to reach the appropriate level is needed.
Material and Methods: For this, we studied seventy-two human sacra and measured morphometrics like height of canal and transverse diameter. We utilized these measurements for volume estimation of sacral canal and caudal space by forming a simple mathematical formula for volume half-cone.
Results: We observed that mean volumes of sacral canal and caudal space were 38.26 cm3 (23.76-62.78 cm3) and 14.25cm3 (6.67-24 cm3) respectively.Volumes of sacral canal and caudal space had higher values in males than in females.
Conclusion: So, finally, it was concluded that volume of caudal space could be easily calculated this way and it was as reliable as MRI.
Caudal block, Caudal space, Sacral canal
Introduction
The sacrum which has a pyramidal shape, consists of five embryonic fused vertebrae. It is convex dorsally. The coccyx consists of three to five rudimentary vertebral bones and it is triangular, with the base being attached to the sacrum. At the apex of sacram, the V-shaped gap covered by the sacrococcygeal ligament, which is marked dorsally in the midline, is called sacral hiatus. The sacral hiatus is bordered by the sacral cornu laterally. This space is a natural defect in the union of the dorsal midline of the S5 vertebra, where it meets the S4 vertebra (partial defect). Its floor is the vertebral body of S5. It contains the coccygeal nerve and the filum terminale. The sacrum has two sets of foramen – the four posterior sacral foramina and the four anterior sacral foramina. The lateral attachment of the sacrum is the sacroiliac joint, while superiorly, it is attached to the superior articular facet of the L5-S1 facet joints bilaterally, as well as to the L5-S1 disc. The sacral canal extends from the upper border of S1 vertebra to sacral hiatus and sacral hiatus marks the termination of the sacral canal.The sacral canal which is triangular to oval in profile, is located posterior to body of sacrum, which contains the epidural venous plexus, down to the level of S4, epidural fat, roots of sacral nerves and thecal covering in living . The dural and archanoid sheath of spinal cord terminates at the level of S2 vertebra (varies between the lower border of the S1 foramen in adults and the S3 in children.). The part of sacral canal, below the attachment of dural sheath at S2, which is called caudal epidural space or caudal space, is filled with fats, venous plexus, filum terminale and coccygeal nerve. This caudal epidural space is utilized to deliver the local anaesthetic drug for caudal epidural block. The average volume of the sacral epidural canal drops in the geriatric population, for a similar height and gender. The height of the patient, as well as the vertical dimension ofthe sacrum e.g. short sacrum, not only increases the risk of dural puncture, but it also increases chances of cardiac arrest due to excess drug volume, because the drug reaches upto thoracic epidural space [1]. To avoid complications caused by high block, it is necessary to assess available caudal epidural space volume pre-operatively.
Caudal anaesthesia is widely used for intra-operative and post-operative analgesia for a variety of operations and the pain management of chronic backache. Even though caudal anaesthesia has a wide range of clinical applications, it is sometimes hard to determine the anatomical location of the sacral hiatus and the caudal epidural space, especially in adults. The determination of the landmarks by the clinician enables the sacral hiatus to be ascertained and it may increase the success rate of the caudal epidural block [2]. The local anaesthetic drugs which are injected are lidocaine, bupivacaine, etc. For successful block, the amount of the drug is also very important, which is determined by the concentration and volume of drug. The volume of this caudal space in adults is vaguely described as 30-32ml in literature [3].
The increasing use of caudal block provoked us to investigate the anatomy of sacral canal and hiatus, along with the volume of caudal space. The volume of caudal space was estimated by Lanier, by injecting solution and by marking its rise in the vertebral column and thus, volume of sacral canal was estimated [4]. Complications have been reported with injections of high volumes into the epidural space. This increases intraocular pressure with retinal haemorrhage in 45-50 cases [5]. Cyriax, who used high-volume injections utilizing 50 ml of procaine, reported two cases of temporary paraplegia [6].
It has been assumed by clinicians that short statured individuals need less volume of drug in comparison to long stratured ones [7]. Till date, no tool or formulation is available, to assess the approximate volume of caudal space, purely based on bony or surface landmarks. In this study, we tried to formulate the volume of caudal space, based on bony landmarks, so that clinicians could appreciate the volume of this space and adjust the volume of drugs.
Material and Methods
Totally, seventy-seven dry human sacra were collected from the Departments of Anatomy of four medical colleges. Developmentally abnormal sacra, lumbralized sacra and sacralization of the 5th lumbar vertebra were excluded. The rest of sacra (Seventy-two) were analyzed for sex determination by anatomists. These were analyzed to be forty-two female and thirty male sacra. Anatomical measurements were performed on these specimens by an anatomist and an anaesthetist by using a vernier caliper which was accurate to 0.1 mm. Four direct morphometric measurements of the sacral vertebra and hiatus were obtained [Table/Fig-1].The measured parameters were: (1) height of sacral hiatus; (2) distance from the sacral apex to the level of S2 foramina: h (3) distance between the upper border of S1 and sacral apex: H(4) distance between the two superolateral sacral crests (the base of the triangle) at the level of S1: D and below S2: d
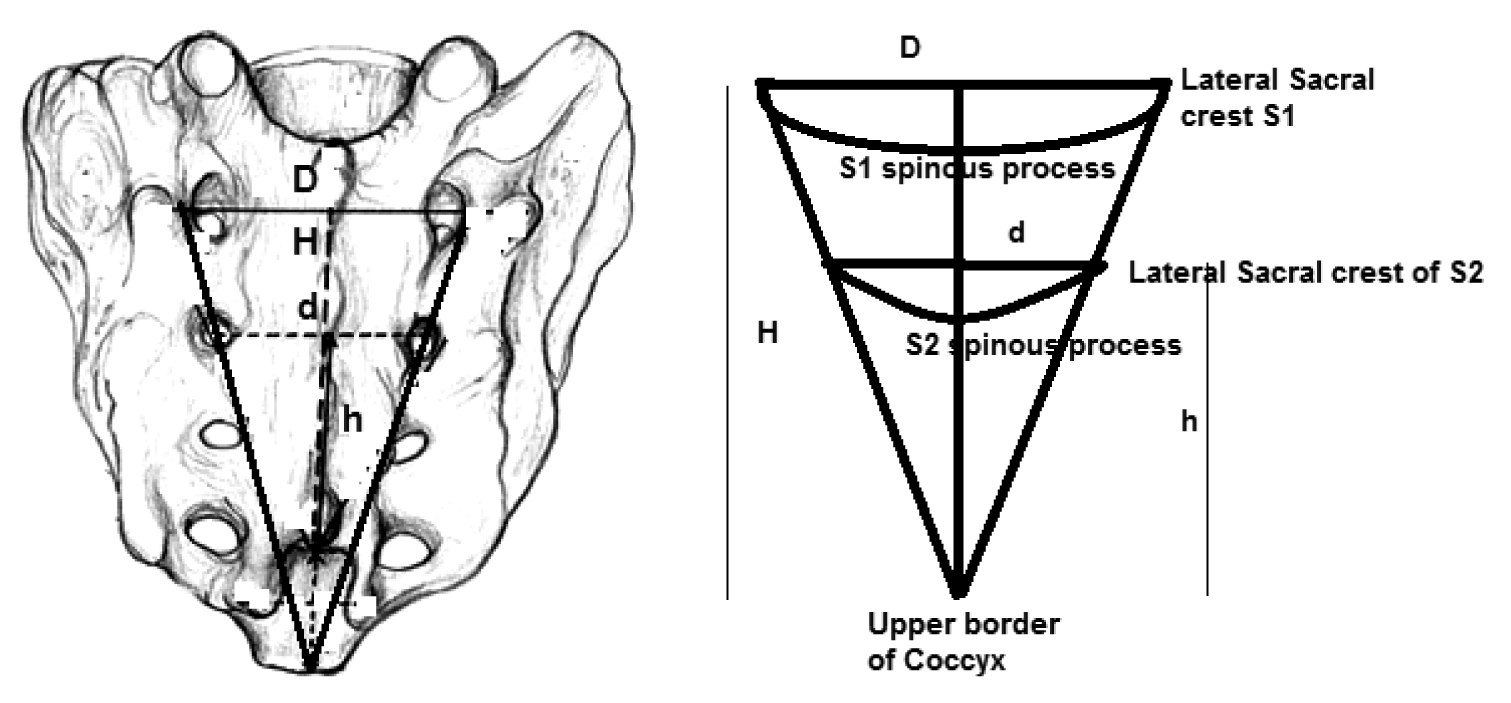
The shape of sacral canal varies from the triangular pyramid to oval half cone. Volume of sacral canal was estimated by applying the mathematical formula of half cone =ϖD2H/24 and volume of caudal space = ϖd2h/24
Statistical Analysis
Data were expressed as mean (SD), median and range. Analyses were performed using Microsoft Excel 2007 software.
Results
The mean volume of sacral canal is 38.26 cm3 (23.76-62.78 cm3) and the mean volume of caudal space is 14.25cm3 (6.67-24 cm3). The mean volume of the sacral canal in male sacrum is 43.06±10.88 cm3, but in females, this value is 34.86±6.86 cm3. There is significantly higher volume of the sacral canal than female (p<0.03827). The mean caudal volume in male sacrum is 16.76±4.29 cm3, whereas this value in females is 12.46±3.52 cm3. Again, the caudal volume is also higher in males than in females (p<0.0134) [Table/Fig-2 and 3].
Descriptive statistics of volume of sacral canal and caudal space respectively
| Descriptive Statistics | Volume of Sacral Canal (Cm3) | Descriptive Statistics | Volume of Caudal Space |
|---|
| Mean | 38.26198462 | Mean | 14.25094931 |
| Standard Error | 1.938966875 | Standard Error | 0.888423253 |
| Median | 37.54247619 | Median | 14.05366667 |
| Mode | NOT APPLICABLE | Mode | NOT APPLICABLE |
| Standard Deviation | 9.498958942 | Standard Deviation | 4.35236729 |
| Sample Variance | 90.23022098 | Sample Variance | 18.94310103 |
| Kurtosis | 0.792494228 | Kurtosis | -0.10837845 |
| Skewness | 0.806103106 | Skewness | 0.390276019 |
| Range | 39.01114286 | Range | 17.5917 |
| Minimum | 23.76785714 | Minimum | 6.67 |
| Maximum | 62.779 | Maximum | 24.2617 |
| Sum | 918.287631 | Sum | 342.0227833 |
| Count | 24 set of 3 (72) | Count | 24 set of 3 (72) |
| Largest(1) | 62.779 | Largest(1) | 24.2617 |
| Smallest(1) | 23.76785714 | Smallest(1) | 6.67 |
| Confidence Level(95.0%) | 4.011058559 | Confidence Level(95.0%) | 1.837843513 |
Discussion
Successful performance of a caudal block requires identification of the sacral hiatus, passage of the needle in hiatus and adequate volume of drug. A detailed knowledge on anatomy, dimension and variations of sacral region is therefore desirable, to increase the reliability and safety of using this technique. The early anatomical study done by Lanier suggested that the volume of the sacral canal using rising of fluid level in vertebral column was slightly more than 30ml (range 12-65ml) [4]. In our case, the volume of sacral canal was 38.26cm3 (ml) (range 23.67-62.78 ml). This showed that there were no differences between fluid injecting technique and morphometric volume estimation. This finding also suggested that there were no major differences in volume of the sacral canal in European and Indian races.
The caudal volume estimated by Crighton and Barry with the help of MRI was 14.4 cm3 (range 9.5-26.6cm3) [8]. In our case, the caudal volume measured by a simple morphometric method was 14.25 cm3 (range 6.67-24.26 cm3). Again, the differences were very minimal. We did not find any more literature for comparing these.
From above findings, we could conclude that the volume of sacral canal or caudal space could be easily calculated through morphometric assessments and by applying formula of volume of half cone. This is a reliable, simple, inexpensive and quick method for assessing the caudal volume.
[1]. Bentley A, OgokeCaudal Epidural Steroid Injections Pain Physician 2000 3(3):305-12. [Google Scholar]
[2]. Senoglu N, Senoglu M, Oksuz H, Gumusalan Y, Yuksel KZ, Zencirci B, Landmarks of the sacral hiatus for caudal epidural block: An anatomical studyBritish Journal of Anaesthesia 2005 95(5):692-95. [Google Scholar]
[3]. Burn JM, Guyer PB, Langlon L, The spread of solutions injected into epidural space. A study using epidurograms in patients of lumbo-sciatic syndromeBritish Journal of Anaesthesia 1973 45:338-44. [Google Scholar]
[4]. Lanier PF, Trotter M, The volume of the sacral canalAmerican Journal of Physical Anthropology 1946 4:227-33. [Google Scholar]
[5]. Evans W, Intrasacral epidural injection in the treatment of sciaticaLancet 1930 2:1225-29. [Google Scholar]
[6]. Cyriax JH, Epidural anesthesia and bedrest in sciaticaBr Med J 1961 1:20-24. [Google Scholar]
[7]. Park WY, Massengale M, Macnamara TE, Age, height and speed of injection as factors determining caudal anaeshtetic level and occurance of severe hypertensionAnaesthesiology 1979 51:81-84. [Google Scholar]
[8]. Crighton IM, Barry BP, Hobbs GJ, A study of anatomy of caudal space using magnetic resonance imaging 1997 78:391-395. [Google Scholar]