Prevalence of diabetes is rising all over the world. Saudi Arabia has one of the highest prevalence of type 2 diabetes in the world. Nearly one-fourth of adult Saudi population is suffering from type 2 diabetes mellitus. A nationwide, community based study showed that the overall prevalence of Diabetes Mellitus was 23.7% in Kingdom of Saudi Arabia. The prevalence in males and females were 26.2% and 21.5% respectively [1].
Studies have confirmed that increase in diabetes prevalence results from urbanization and socioeconomic development, which are associated with rapid changes in lifestyle [2]. During past few decades, tremendous surge in socioeconomic growth in Saudi Arabia has considerably influenced the lifestyle of Saudis.
Clark et al., have identified that setting appropriate goals, monitoring complications regularly, dietary and exercise modifications, medications, self monitoring of blood glucose and laboratory assessment are required for adequate diabetes care [3].
Compliance is the best way to control diabetes and to prevent its complications. Patient compliance or adherence is defined as the extent to which a person’s behaviour coincides with health related advice [4]. This in turn, requires a high level of knowledge of the disease, its complications and its management among the patients. Educating, motivating and guiding the patient to manage his/her diabetes can go a long way in lowering the burden of diabetes, on health care services.
Personal factors like age, gender, marital status, educational status, smoking status and BMI grades play important role in compliance to diabetes management. This study was conducted to find the compliance of diabetic patients at primary health care centres of Abha, Saudi Arabia, regarding their exercise, diet, medication and follow-up. As a part of a larger study, we identified the personal characteristics which determined the compliance.
Material and Methods
Study setting
This study was conducted in Abha City, which is the capital of Aseer Region, at the southwestern part of KSA. It is situated at 2,200 meters above the sea level. The population of Abha, as per 2004 census, is 3, 52,303 [5].
Study design
Cross sectional study
Study population: Following a simple random sample, 2 PHCCs (Primary Health Care Centres) were selected for carrying out the study. There were 632 registered diabetics in Al Manhal PHCC and there were 585 in Al Kabel PHCC. A total of 406 patients were interviewed.
Inclusion criteria
Type 2 diabetes
Duration of disease of more than one year
Registered at the selected PHCC
Exclusion criteria
Type 1 diabetic patients
Recently diagnosed patients (< 1 year)
Visiting patients who were not registered at the PHCC
Patients who did not agree to participate
Study tool: Interview questionnaire which included questions that covered the subject’s socio-demographic and lifestyle information and self reported compliance information was developed for use in the study.
Study period: May, 2010-April, 2011.
Statistical design: SPSS, version 16.0 was used for data entry and analysis. Descriptive and analytic statistics (Frequency, percentage and Chi–Square test) were applied as required.
Ethical Consideration
Patients were informed about purpose of the study, confidentiality of the data and anonymity. Only those patients who agreed were interviewed.
Results
[Table/Fig-1] describes the study population. Almost three fourths of patients were between 40-60 years age. A majority of patients were Saudi males. Most of the patients were married. A very large number of patients were illiterate, while only few had a university education.
Personal characteristics of study sample
| Variables | n | % |
|---|
| Age groups | | |
| • <40 years | 21 | 5.2 |
| • 40-60years | 286 | 70.4 |
| • >60years | 99 | 24.4 |
| Gender | | |
| • Male | 243 | 59.9 |
| • Female | 163 | 40.1 |
| Nationality | | |
| • Saudi | 371 | 91.4 |
| • Non-Saudi | 35 | 8.6 |
| Marital Status | | |
| • Single | 16 | 3.9 |
| • Married | 390 | 96.1 |
| Educational status | | |
| • Illiterate | 171 | 42.1 |
| • Primary/Intermediate | 92 | 22.7 |
| • Secondary | 83 | 20.4 |
| • University | 60 | 14.8 |
| Smoking status | | |
| • Smoker | 64 | 15.8 |
| • Non-smoker | 342 | 84.2 |
| BMI grades | | |
| • Normal (<25Kg/m2) | 30 | 7.4 |
| • Overweight (25-30 Kg/m2) | 167 | 41.1 |
| • Obese (≥30Kg/m2) | 209 | 51.5 |
[Table/Fig-2] provides information on personal characteristics, vis a vis, the compliance with various aspects of diabetes management. Young patients (age<40) were more compliant with all aspects of management, except medication, with which older patients were more compliant. Low level of compliance to medication in young diabetics may lead to increased risk of complications. Women were significantly more compliant with exercise, while males were significantly more compliant with follow up. Saudi patients were significantly compliant with medication, while non Saudis were more compliant with exercise. Medication and follow up, as advised, were followed by a majority of patients, irrespective of their personal characteristics. Diabetic patients may consider medication and follow up as important aspects of their diabetes management, while ignoring other aspects like diet and exercise. Diet and lifestyle advice was less followed by all patients, although these formed the foundation for diabetes management.
Personal characteristics of diabetic patients and their Compliance. * p < 0.05 (statistically significant)
| Variables | Aspects of Compliance |
|---|
| Diet | Exercise | Medication | Follow up |
|---|
| No (%) | Yes (%) | No (%) | Yes (%) | No (%) | Yes (%) | No (%) | Yes (%) |
| Age groups | | | | | | | | |
| • <40years | 0 (0.0) | 21* (100.0) | 4 (19.0) | 17* (81.0) | 16 (76.2) | 5 (23.8) | 0 (0.0) | 21* (100.0) |
| • 40-60years | 133 (46.5) | 153 (53.5) | 158 (55.2) | 128 (44.8) | 55 (19.2) | 231* (80.8) | 70 (24.5) | 216 (75.5) |
| • >60years | 43 (43.4) | 56 (56.6) | 67 (67.7) | 32 (32.3) | 22 (22.2) | 77 (77.8) | 27 (27.3) | 72 (72.7) |
| Gender | | | | | | | | |
| • Male | 103 (42.4) | 140 (57.6) | 147 (60.5) | 96 (39.5) | 53 (21.8) | 190 (78.2) | 46 (18.9) | 197* (81.1) |
| • Female | 73 (44.8) | 90 (55.2) | 82 (50.3) | 81* (49.7) | 40 (24.5) | 123 (75.5) | 51 (31.3) | 112 (68.7) |
| Nationality | | | | | | | | |
| • Saudi | 157 (42.3) | 214 (57.7) | 216 (58.2) | 15.5 (41.8) | 77 (20.8) | 294* (79.2) | 88 (23.7) | 283 (76.3) |
| • Non-Saudi | 19 (54.3) | 16 (45.7) | 13 (37.1) | 22* (62.9) | 16 (45.7) | 19 (54.3) | 9 (25.7) | 26 (74.3) |
| Marital status | | | | | | | | |
| • Single | 0 (0.0) | 16* (100.0) | 4 (25.0) | 12* (75.0) | 9 (56.2) | 7 (43.8) | 4 (25.0) | 12 (75.0) |
| • Married | 176 (45.1) | 214 (54.9) | 225 (57.7) | 165 (42.3) | 84 (21.5) | 306* (78.5) | 93 ( 23.8) | 297 (76.2) |
| Educational status | | | | | | | | |
| • Illiterate | 83 (48.5) | 88 (51.5) | 102 (59.6) | 69 (40.4) | 39 ( 22.8) | 132 (77.2) | 34 (19.9) | 137 (80.1) |
| • Primary/Inter | 28 (30.4) | 64 (69.6) | 38 (41.3) | 54 (58.7) | 19 (20.7) | 73 (79.3) | 24 (26.1) | 68 (73.9) |
| • Secondary | 46* (55.4) | 37 (44.6) | 61* (73.5) | 22 (26.5) | 23* (27.7) | 60 (72.3) | 27 (32.5) | 56 (67.5) |
| • University | 19 (31.7) | 41 (68.3) | 28 (46.7) | 32 (53.3) | 12 (20.0) | 48 (80.0) | 12 (20.0) | 48 (80.0) |
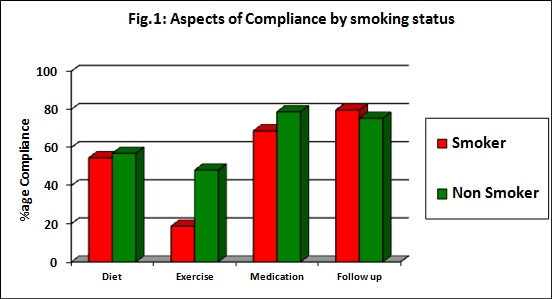
[Table/Fig-3] Smokers were significantly less compliant than non smokers with exercise. There was no significant difference between compliance of smokers and non smokers regarding diet, medication and follow up.
Aspects of compliance by smoking status
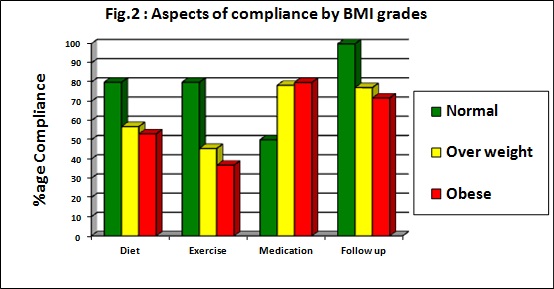
[Table/Fig-4] Patients with normal BMI were significantly more compliant with diet, exercise and follow up.
Aspects of compliance by BMI grades
Discussion
Compliance is the cornerstone of diabetes management. Among the determinants of compliance, personal characteristics are the most important ones. The distribution of study population was similar to those which were reported in other regional studies [6–10].
This study revealed a suboptimal compliance with all aspects, especially with diet and exercise. A study done in Al-Hasa region, Saudi Arabia, indicated that there was a high rate of non-compliance among diabetic patients [7]. Poor compliance regarding diet and exercise has also been found in studies done in UAE [8], Palestine [9], and Egypt [10,11].
The present study revealed that young patients (age<40) were significantly more compliant with appointment and diet, while older patients were more compliant with medication. A similar finding was reported in research done by Gimenes et al., in Brazil [12].
Overall, it was found that diet and lifestyle advice was followed less by all patients. Most of the studies done in the region showed poor dietary compliance. A study done in southwestern Saudi Arabia found that there was a good compliance among less than half of patients who were on dietary regimen [13]. In Qassim, among married and non-obese patients, the percentage of those who were on an unhealthy diet was high [14].
A study done in Egypt showed that more than three quarters of the diabetics adhered poorly to the prescribed diet [10]. Another study done at a primary care level in Egypt found that compliance of diabetic patients with most types of diabetes regimens was low [15]. There has been a change in dietary patterns and lifestyles of middle eastern people over the past few decades, with increased use of convenience foods and sedentary lifestyles.
Gender was found to be a significant determinant of exercise compliance, with women being more compliant. This may be due to increased availability of free time to women. In the Qassim study, a majority of the patients practised physical exercise only up to 2 times per week [14].
A majority of the patients adhered to the medication and follow up as they were advised. Similar results have been reported in studies done in Egypt [10,16]. This finding could indicate that health care professionals may be failing to emphasize the importance of dietary and lifestyle changes along with medication and follow up advice. However, as compared to women, men were significantly more compliant with follow up. Nationality was found to be a significant determinant of compliance. Saudis were more compliant with medication, while non Saudis were more compliant with exercise. This could be due to more availability of resources to Saudis, along with a sedentary lifestyle.
Regarding diet and exercise, single patients were found to be significantly more compliant than married patients. This could be explained by the fact that single patients had less social and family commitments and so, they could find more time for exercise. They could also control their diet better, as they did not face a social compulsion to eat with others. Married patients were more compliant with medication. This could be explained by the social phenomenon of caring for the spouse, and reminding him/her about taking medication. However, as was reported by Beverly and Wray, spousal support was found to be more strongly related to lifestyle changes [17].
Educational status was a significant determinant of compliance. University educated patients had more compliance than other groups. Similar results were reported from around the world [9,10,12,18].
This finding emphasized the fact that level of education played a role in better understanding of the doctors’ advice. This study found that smokers were significantly less compliant with exercise. Studies have shown that smoking increased blood glucose concentrations and that it could increase insulin resistance [19, 20]. The smokers also tended to have higher blood concentrations of glycosylated haemoglobin (HbA1c) than the non-smokers [21, 22]. Health care professionals can provide health education which has been tailored to meet the individual needs of patients. They can help in suitably designing culturally appropriate diets and exercise advice to the patients, like diabetes management in the holy month of Ramadan. As smoking is prohibited during Ramadan, patients can be motivated to quit smoking during this time.
BMI was a significant determinant of compliance. Patients with normal BMI were found to be more compliant with diet, exercise and appointments. Obese patients were found in various studies to be less compliant to diabetes regimen and thus, to fail in reaching the target levels [23].
Weight management strategies like setting short term goals can be taught to the patients for their benefit. Importance of regular exercise and its role in diabetes management, along with weight reduction, should be emphasized for the obese patients.
Limitations and Scope
This study was conducted in an urban area, on patients with type 2 diabetes and thus, it cannot represent the whole diabetic population. Saudi Arabia, being one of the top ten countries for prevalence of diabetes [24], it is essential to study the pattern of compliance among all sections of diabetics, in order to improve diabetes management.
Conclusion
From the study, we conclude that a suboptimal compliance to diabetes management is related to personal factors. Social and lifestyle characteristics may significantly determine compliance. Thus, it is necessary to improve the understanding of these characteristics and to individualize the treatment regimen according to patients’ requirements. Programs to increase patient awareness on diabetes mellitus are essential to improve their understanding of their disease and compliance to advised treatment.