Iodine deficiency disorders (IDD) are a major public health problem all over the world, including India. Its major manifestations are endemic Goitre, mental defects, deaf mutism, still births and miscarriages, weakness and paralysis of muscles as well as lesser degree of physical and mental functions [1]. Globally, 2.2 billion people live in areas with iodine deficiencies, with the risks of resulting complications, while in India; 167 million people are at risk of IDD, 54.4 million people have Goitres, and 8.8 million people have IDD-related mental / motor handicaps [2]. Enlargement of thyroid gland is the common manifestation of the IDD and Goitre prevalence survey is used as diagnostic tool for identifying areas of IDD. Failure to undertake early detection and intervention measure results in secondary disabling conditions [3]. School age children are an especially useful population group for the assessment of IDD, both because of their physiological vulnerability and their accessibility through schools [4].
Though many studies have been conducted worldwide, and in many parts of India, hardly studies have been carried out in the southern interior part of Karnataka, India. In view of this, a study was planned in Chamarajanagar district with the objective to find out the Goitre prevalence in school children aged 6–12 years and to assess the level of iodine in salt at household levels.
Methodology
Selection of study subjects
This Cross Sectional study was conducted in the four taluks of Chamarajanagar district by using the method of Population Proportionate to Size Sampling (PPS) [5]. Informed consent was obtained from the Block Education Officer (BEO) of each taluk and from the headmasters of the schools studied, as the children belonged to the minor age group. With 5% level of significance, power 80%, the prevalence in India 19% [6], effect size 0.019, permissible error 10%, “not equal to” alternative hypothesis and using hypothesis testing technique, the sample size was 3347. However, a total of 3757 children from Chamarajanagar district were studied. Applying Neyman’s allocation technique the taluk wise sample size was derived. A total of 30 villages were selected from the entire district and were distributed to four taluks [7,8]. PPS systematic sampling technique was applied to each taluk in selecting the required number of villages. The survey was done among these villages in children studying in primary schools from 1st to 7th standard in the age group of 6-12 years. Goitre was assessed clinically by physical examination of the thyroid gland and graded as;
Grade 1–Thyroid swelling which is not seen but palpable.
Grade 2–Thyroid swelling which is seen and palpable.
Salt samples were collected from the corresponding houses of every fifth child examined in the school. The iodine content of the salt samples was estimated by using standardized iodine testing kits and expressed as iodine in ppm.
Statistical Analysis
Data regarding the determinants of goitre, grades of goitre and the salt sample results were compiled and analyzed by using appropriate statistical tests. Chi –Square test was used to compare the prevalence with age and sex distribution.
Results
In the present study, a total of 3757 children in the age group of 6 -12 years were studied. The overall prevalence of goitre in Chamarajanagar district was found to be 7.74% [Table/Fig-1].
Taluk wise Prevalence of Goitre in Chamarajanagar District
| Sl. No. | Taluks | Population of school children | Total No of children examined | Grade 1 Goitre | Grade 2 Goitre | Total |
|---|
| No | % | No | % | No | % |
|---|
| 1 | Kollegal | 43164 | 1289 | 25 | 1.93 | 10 | 0.77 | 35 | 2.71 |
| 2 | Chamarajanagar | 34672 | 1136 | 71 | 6.25 | 13 | 1.14 | 84 | 7.39 |
| 3 | Gundlupet | 22108 | 969 | 108 | 11.14 | 49 | 5.05 | 157 | 16.20 |
| 4 | Yelandur | 8593 | 363 | 11 | 3.03 | 4 | 1.1 | 15 | 4.13 |
| Total | 108537 | 3757 | 215 | 5.72 | 76 | 1.99 | 291 | 7.74 |
From [Table/Fig-2] it is observed that Grade 1 goitre is more among females (51.16%) as compared to males (48.84%) though not statistically significant (p-value=0.733). However, with respect to grade 2 goitre the difference is significant (p-value=0.012). The overall prevalence of goitre is also higher among female children which is statistically significant (p-value=0.045).
Sex wise distribution of Goitre cases
| Male | Female | Total | p-value |
|---|
| Grade1 | 105 (48.84%) | 110 (51.16%) | 215 | 0.733 |
| Grade2 | 27(35.53%) | 49 (64.47% ) | 76 | 0.012* |
| Total | 132(45.36%) | 159(54.64%) | 291 | 0.045* |
[Table/Fig-3] shows an increasing trend in the prevalence rates in the higher classes (with increasing age). It is observed that the prevalence of goitre is highest in class 7 students (17.6%) followed by class 6 students (10.9%) and overall it is higher among females (54.63%) as compared to males (45.37%). In class 7 students the prevalence of Grade 2 goitre cases were found to be higher among females as compared to males. This was statistically significant (p=0.039).
Classwise prevalence of Goitre according to Grade and Sex
| Class | Sex | Total Examined | Grade of Goitre | Total Cases | Percentage |
|---|
| Grade I (p-value) | Grade II (p-value) |
| Class I | Male | 274 | 10 | 4 | 14 | 5.1 |
| Female | 263 | 8 | 4 | 12 | 4.6 |
| Total | 537 | 18(0.637) | 8(1.000) | 26 | 4.8 |
| Class II | Male | 269 | 6 | 4 | 10 | 3.7 |
| Female | 251 | 5 | 3 | 8 | 3.2 |
| Total | 520 | 11(0.763) | 7(0.705) | 18 | 3.5 |
| Class III | Male | 229 | 6 | 5 | 11 | 4.8 |
| Female | 249 | 8 | 5 | 13 | 5.2 |
| Total | 478 | 14(0.593) | 10(1.000) | 24 | 5 |
| Class IV | Male | 275 | 8 | 2 | 10 | 3.6 |
| Female | 253 | 10 | 4 | 14 | 5.5 |
| Total | 528 | 18(0.637) | 6(0.414) | 24 | 4.5 |
| Class V | Male | 286 | 14 | 2 | 16 | 5.6 |
| Female | 280 | 18 | 6 | 24 | 8.6 |
| Total | 566 | 32(0.480) | 8(0.157) | 40 | 7.1 |
| Class VI | Male | 297 | 22 | 5 | 27 | 9.1 |
| Female | 291 | 24 | 13 | 37 | 12.7 |
| Total | 588 | 46(0.768) | 18(0.059) | 64 | 10.9 |
| Class VII | Male | 286 | 39 | 5 | 44 | 15.4 |
| Female | 254 | 37 | 14 | 51 | 20.1 |
| Total | 540 | 76(0.819) | 19(0.039) | 95 | 17.6 |
On examining salt for iodization levels, it is noted that overall 28.42% of the salt samples in Chamarajanagar district had iodine level less than 15 PPM with the highest deficiency observed in Gundlupet taluk (41.18%) [Table/Fig-4].
Taluk-wise Salt sample analysis Note: numbers in brackets indicate percentage
| Taluk | 50 PPM | 30 PPM | 15 PPM | < 15 PPM | Total | p-value |
|---|
| Kollegal | 52(20.96) | 85(34.27) | 68(27.41) | 43(17.33) | 248 | 0.733 |
| Chamaraja-nagar | 70(30.70) | 45(19.73) | 42(18.42) | 71(31.14) | 228 | 0.012* |
| Gundlupet | 45(22.05) | 35(17.15) | 40(19.60) | 84(41.18) | 204 | 0.045* |
| Yelandur | 25(31.25) | 26(32.50) | 11(13.75) | 18(22.50) | 80 | 0.045* |
| Total | 192(25.26) | 191(25.13) | 161(21.18) | 216(28.42) | 760 | 0.045* |
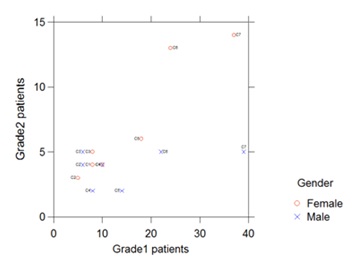
[Table/Fig-5] shows a unique representation of four variables on two dimensional dot plot. It is noticed that in C7, there is insignificance with respect to Grade 1, however Grade 2 shows significance. For C6, there is significance at Grade 2.
Two Dimensional Dot plot for Goitre levels, Class and Gender
Discussion
Our study carried out among 3757 school children in Chamarajanagar district, showed a goitre prevalence of 7.74%. This result was in accordance with studies done in Kottayam, Kerala (9.8%) [9] and Malda, West Bengal (l1.3%) [10].
From [Table/Fig-1] it was observed that the prevalence of goitre varied from 2.63% to 16.20% in different taluks of the district, being highest in Gundlupet taluk (16.20%). The acquired sample size in Chamarajanagar district was marginally higher compared to the estimated sample size. However, due to non-availability of children in certain schools of Kollegal taluk, the sample size was slightly lesser than estimated in spite of multiple visits.
A higher prevalence of goitre was observed in girls. This is consistent with many other studies. A study conducted in Belgaum district of Karnataka, India by Kamat et al., showed higher prevalence of goitre among girls (21.1%) compared to boys (12.8%). Another study done in coastal district of Karnataka by Rao et al., showed similar result, with prevalence of goitre among male children being only 28% compared to 31.2% among female children [11]. A study carried out in Kottayam district of Kerala reported a higher prevalence among girls (21.1%) compared to boys (12.8%). Sahu et al., reported a similar pattern in a study in Orissa: a prevalence of 23.1% in girls and 17.3% in boys [12]. This may be attributed to the genetic predisposition among females to develop thyroid enlargement in response to iodine deficiency.
In terms of the relationship of Goitre prevalence with age, we found that the prevalence was higher in older children: 17.6% in class 7 and 10.9% in class 6, as compared to the younger children (classes 1 to 5) where it ranged from 4.8% to 7.1%. A similar observation was noted in a study by Bhat IA et al., 12.8% in 9 to 12 year old children as against 10.6 % in 6 to 8 year old children [13]. In a study in Kottayam, higher prevalence was noted in higher age group children, being 12.3% in 10-12 year age group as compared to lower age group children. A similar finding was noted in a study conducted in Bhubaneswar [14] which showed a significantly high prevalence of Goitre among 10-12 year age group compared to 6-8 year age group. This may be due to the enhanced requirements for thyroid hormones during puberty. Another contributing factor could be the long standing iodine deficiency manifesting ultimately as enlargement of thyroid gland in older age groups.
[Table/Fig-5] shows a unique representation of four discrete random variables on two dimensional dot plot that supports [Table/Fig-3]. It indicates that there is a risk of conversion of Grade1 to Grade 2 in females as and when age increases. In fact, red points are dense, moving from left bottom to right top corner indicating high positive association among females. However points corresponding to male are also positively associated but scattered. With respect to the school children in total, a cluster is formed at the lower end indicating no association; this is an impact of male children on the total. However, with respect to females the association is very clearly seen from the beginning to the end. Class attribute is considered instead of age alone as this has an impact of age and knowledge together. Classes C6 and C7 are of interest here, as in C7 it is clear that insignificance is seen with respect to Grade 1, however Grade 2 shows significance. In C6, we can observe that for grade 2 near significance has been achieved. These points are supported by chi-square p-values as indicated in [Table/Fig-3].
Analysis of salt samples revealed that 71.58% of the salt samples had adequate iodine content (>15 ppm) and 28.42% of the salt samples had inadequate iodine levels (<15ppm). Similar results were seen in other studies: in a study conducted in Belgaum, 50% of the households used adequate iodized salt, in a study in Delhi, it was observed that 41% of the households consumed adequate iodized salt [15], in a study carried out in Malda, 85.1% of the households used salt with adequate iodine. In NFHS - 3, it was observed that 51% population of the country was using adequate iodized salt (>15 ppm) and in coverage evaluation survey 2009, 71.1 percent of the households in the country were using cooking salt which was iodized at the recommended level of 15 ppm or more [16].
The level of iodized salt consumption in Chamarajanagar district (71.58%) was still lower than the national goal of 90% adequate iodized salt consumption [17]. These findings suggest that sustained information, education and communication efforts are required to accelerate the progress towards reaching the goal of universal iodization of salt in the district of Chamarajanagar.
Conclusion
The prevalence of goitre in our study area was 7.74%, which is marginally above the criteria to define an area as endemic (>5%). This indicates that Chamarajanagar district is in a transition phase from iodine deficient to iodine sufficient. There is a need to further strengthen the implementation strategies of National Iodine Deficiency Disorders Control Program in this district in order to make it free from iodine deficiency.