Herpes zoster (shingles) is commonly encountered disorder in general practice, with a cumulative life time incidence of 10-20% [1]. One fifth of the population, mainly elderly people will present with this neurocutaneous infection during their life time.
The characteristic zoster pain is often accompanied by substantial pain, dysasthesia and skin hypersensitivity. The unmet challenge in the management of patients with acute zoster is the alleviation of chronic pain. In many patients pain resolves once the affected area of the skin returns to normal. However some patients continue to experience pain long after the lesions have healed. The pain is commonly called as postherpetic neuralgia, which is by far the most common complication of herpes zoster and is one of the most intractable pain disorders [2,3].
The incidence of PHN increases sharply with increasing age. It is also more severe and persists longer in older than in younger patients. The disorder is clearly the most distressing component of the disease process for both the patients and the physician. Although for many years, acyclovir has been the oral antiviral agent approved for the treatment of patients with acute herpes zoster, its effect on postherpetic neuralgia remains controversial [4,5].
Famciclovir, a new antiviral agent was approved for marketing by the FDA in June 1994 for the management of acute herpes zoster. It is a well absorbed (77% bio available) oral form of penciclovir, with activity against VZV. It selectively gets activated in virus infected cells through phosphorylation to the antiviral compound famciclovir triphosphate.
A potentially clinically important characteristic feature of famciclovir triphosphate is that it persists in virus infected host cells longer than the acyclovir triphosphate. Consistent oral bioavailability, linked to a favorable intracellular halflife of penciclovir triphosphate in cells infected with VZV suggested that famciclovir could offer clinically important advantages in the management of herpes zoster over currently available therapy [6].
Material and Methods
It was a comparative randomized clinical study conducted on the patients, attending outpatient department of Department of Skin and STD, in Kempegowda Instutite of Medical Sciences Hospital, Bengaluru, India, during the period of October 2005 to April 2007.
A comprehensive history was recorded in every patient with reference to their age, sex, prodromal symptoms, past history of chickenpox, family history, history of diabetes, systemic steroid therapy, radiotherapy and previous malignancy. Clinical features at the time of diagnosis, dermatomal distribution and extent of disease were noted.
A detailed general physical and systemic examination was carried out to find any signs of major illness. Routine investigations of blood and urine were done in all patients. Diagnosis was confirmed by Tzanck smear.
Smears were prepared from the floor of the fresh vesicle and were stained with Leishman stain to detect multinucleated giant cells. Biopsy was done in few patients to study the histopathology changes.
Inclusion criteria
Immunocompetent patients over the age of 40 years with uncomplicated herpes zoster, characterized by localized, cutaneous lesions (papules or vesicles) presenting within 72 hours of the onset of the rash.
Exclusion criteria
Patients with complications of herpes zoster, including ocular involvement, severe disseminated infection, motor neuropathies, encephalitis or cerebrovascular complications.
Pregnant or nursing women
Concurrent malignancy receiving chemotherapy
Autoimmune disease under immunosuppressive therapy
HIV sero-positive.
Patients who satisfied the inclusion criteria during the screening visit day were enrolled in the study and were randomized 1:1 ratio to receive either 800mg of acyclovir 5 times daily or famciclovir 250mg thrice daily for a period of 7 days.
Efficacy assessment
Patients were evaluated for pain and healing of the cutaneous lesions on day 7 after initiation of therapy and every week thereafter, for a period of six weeks. The primary variables evaluated at each visit were: the time taken for the full crusting of the lesions, lesions were defined to be fully crusted when all the papules and vesicles in the affected dermatome had resolved and crusts had appeared [7], the time taken for complete healing of the lesion, healing was defined as the first time in which a patient had no papules, vesicles or crusts and after which did not develop them at any later visit [1].
Time taken for loss of acute pain was assessed by visual analogue scale; the visual analogue score 8 was calculated as follows
No pain: score 0
Worst ever felt pain: score 10
Mild pain: score 1, 2, 3
Moderate pain: score 4, 5, 6
Severe pain: score 7, 8, 9
The secondary parameters included: assessing the primary variables in the patients aged above 60 years with each drug and the relative efficacy of each drug in different dermatomes (cranial, cervical, thoracic, and lumbar) in patients aged above 60 years.
Safety assessments
The number and percentage of patients reporting at least one adverse event during the treatment protocol were assessed. Drug related adverse events were defined as those adverse events that were related or possibly related to the study therapy or as being of unknown causality. The frequently reported events were nausea, headache, vomiting and constipation. The complete blood cell count, urinanalysis and serum biochemistry test at baseline and at the end of treatment were mentioned.
Ethics
Cost of investigation (if any) will be borne completely by investigator.
The personal details of the subject will be kept confidential
Statistics
Continuous variables were described by mean, median, standard deviation and range. Categorical data were summarized by counts and percentages.
The following statistical methods were used: Cross tabs, Independent-samples t-test, GLM Univariate test and Median test. All the procedures were done through SPSS for Windows (version 14.0-evaluation version) SPSS Inc New York, 2004.
Crosstabs
The crosstabs procedure forms two-way and multi-way tables and provides a variety of tests and measures of association for two-way tables. The structure of the table and whether categories are ordered determine what test or measure to use. Crosstabs’ statistics and measures of association are computed for two-way tables only.
Independent-Samples t-test
The Independent-samples t-test procedure compares means for two groups of cases. Ideally, for this test, the subjects should be randomly assigned to two groups, so as to know if response is due to the treatment (or lack of treatment) and not due to other factors.
The GLM Univariate test
The GLM Univariate procedure provides regression analysis and analysis of variance for one dependent variable by one or more factors and/or variables. The factor variables divide the population into groups.
Median test
The test for several independent samples procedure compares two or more groups of cases on one variable.
Results
In total 100 patients were enrolled in the study and randomized into acyclovir and famciclovir groups in 1:1 ratio. The overall mean age in group acyclovir was 52.5 years and group famciclovir was 49.64 years, suggesting that both the groups were comparable in respect to their ages as seen in [Table/Fig-1]. Majority of patients (59%) on an average from both groups, were in the age-group of 40-50 years and only 4% in the age-group of above 70 years as seen in [Table/Fig-2].
Mean age in both the groups
| Drug | Mean age | SD | Minimum | Maximum |
|---|
| F | 49.64 | 8.30 | 40 | 75 |
| A | 52.50 | 10.38 | 40 | 80 |
| Total | | 9.46 | 40 | 80 |
Age-group distribution in both the groups
| Age-group | Drug | Total |
|---|
| F | A |
|---|
| 40-50 | Frequency | 35 | 24 | 59 |
| % | 70.0% | 48.0% | 59.0% |
| 51-60 | Frequency | 10 | 15 | 25 |
| % | 20.0% | 30.0% | 25.0% |
| 61-70 | Frequency | 2 | 10 | 12 |
| % | 4.0% | 20.0% | 12.0% |
| 71-80 | Frequency | 3 | 1 | 4 |
| % | 6.0% | 2.0% | 4.0% |
| Total | Frequency | 50 | 50 | 100 |
| % | 100.0% | 100.0% | 100.0% |
The male: female ratio in acyclovir group and famciclovir group was 0.851:1.083, with slightly more number of females in the acyclovir group as shown in [Table/Fig-3].
Gender distribution in both groups
| Gender | Drug | Total |
|---|
| F | A |
|---|
| Male | Frequency | 26 | 23 | 49 |
| % | 52.0% | 46.0% | 49.0% |
| Female | Frequency | 24 | 27 | 51 |
| % | 48.0% | 54.0% | 51.0% |
| Total | Frequency | 50 | 50 | 100 |
| 100.0% | 100.0% | 100.0% |
For the majority of patients in both the groups, the duration of rash at the start of treatment was between 48 and 72 hours.
None of the patients in either group had bilateral involvement of the primary affected region.
The primary variables considered were, time taken for full crusting of the lesion, complete healing and loss of acute pain. Lesions were defined to be fully crusted, when all the papules and vesicles in the affected dermatome had resolved and crusts had appeared. Lesions were defined completely healed, when all the crusts had fallen off with absence of papules and vesicles.
All patients in both treatment groups experienced pain at the time of screening and the distribution of pain intensity was comparable in the two groups. Most patients had moderate pain at the time of screening.
The mean number of days taken for full crusting, complete healing of lesions and acute loss of pain in famciclovir group was 9.1days, 20.4 days and 22.6 days respectively; in acyclovir group was 10 days, 21 days and 23 days and p-values were calculated as seen in [Table/Fig-4]. The time taken for full crusting, complete healing and acute loss of pain in both the groups are more or less similar and the difference is statistically insignificant.
Mean time taken for full crusting, healing and loss of acute pain in both the groups
| Drug | Mean | SD | t | p |
|---|
| Full crusting | F | 9.1000 | 1.3439 | -3.912 | .000 |
| A | 10.0200 | .9792 |
| Healing | F | 20.4600 | 3.5812 | -1.071 | .287 |
| A | 21.1200 | 2.4796 |
| Loss of pain | F | 22.6800 | 4.5957 | -1.179 | .241 |
| 23.8000 | 4.8990 |
The time taken for full crusting in both the groups in patients above 60 years of age was 9 days in famciclovir and 11 days in acyclovir. Time taken for complete healing, was 28 days in famciclovir and 21 days in acyclovir, for acute loss of pain in both the groups was 28 days and and its p-value is seen in [Table/Fig-5].
Patient >60 years- above and below median for time taken for full crusting, complete healing and loss of acute pain in both the groups
| Median | Full crusting | Healing | Loss of pain |
|---|
| F | A | F | A | F | A |
|---|
| Below | 1 | 6 | 4 | 5 | 5 | 11 |
| Above | 4 | 5 | 0 | 0 | 2 | 3 |
| Median value | 10 | 28 | 28 |
| p< | .308 | | 1 |
No clinically significant difference was found in the results of urinalysis, haematology and serum biochemistry at baseline between the treatment groups.
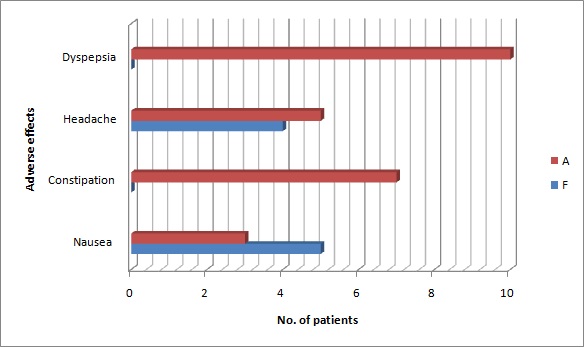
The most common adverse effects reported in both the groups were nausea, headache, constipation and dyspepsia.
Eighty two percent of famciclovir patients had no adverse effects, and the drug was well-tolerated except for 4 patients who had headache and 5 patients who complained of nausea. Adverse effects were slightly higher in acyclovir group with 10 patients having dyspepsia, 7 complaining of constipation, 4 patients of headache and 3 patients of nausea, as seen in [Table/Fig-6].
Adverse effects in both the groups
Discussion
Herpes zoster (shingles) is a commonly encountered disorder in general practice, with cumulative lifetime incidence of 10-20% [1]. One-fifth of the population, mainly elderly people will present with this neurocutaneous infection during their lifetime. Over the years, acyclovir has been the oral antiviral agent approved for the treatment of patients with acute herpes zoster. Its effectiveness in lessening the acute signs and symptoms of herpes zoster has been established but the effects on postherpetic neuralgia are less clearcut. Many placebo controlled trials of acyclovir have failed to draw conclusions about the effect of acyclovir on PHN. Famciclovir is a new member of the guanine nucleoside family of drugs. It is a well-absorbed oral form of penciclovir with a longer half-life, which has recently been approved for the treatment of herpes zoster. Studies have shown that famciclovir, when given three times daily, accelerated the rate of lesion resolution and significantly reduced the duration of PHN.
Complications
Well-marked depressed hyperpigmented or hypopigmented scars on the skin at the sites of eruption were the most common complication noticed in 25% of the patients. Postherpetic neuralgia was the second most common complication noticed in 5% of the cases.
Compare the efficacy and safety of acyclovir and famciclovir in the treatment of herpes zoster
The efficacy and tolerability of a cyclovir in the treatment of herpes zoster is well-established. However, the need to take therapy five times daily is inconvenient for patients and could potentially have an adverse impact on adherence. With the introduction of famciclovir, came the opportunity to administer treatment less frequently (3 times) without compromising the efficacy. The present study was aimed to assess the efficacy and safety of acyclovir and famciclovir in the treatment of acute herpes zoster. At the end of each week the patients were evaluated for the primary endpoints, time taken for full crusting of the lesions, complete healing of the lesion and loss of acute pain. The secondary parameters included: assessing the primary variables in the patients aged above 60 years with each drug, and the relative efficacy of each drug in different dermatomes (cranial, cervical, thoracic, lumbar) in patients aged above 60 years were also considered [Table/Fig-7,8and9]. The median time taken for full crusting of the lesions in both the groups was 10 days, 4 patients in famciclovir and 6 patients in acyclovir group took more than 10 days for full crusting of the lesions. Shen et al., [7] found the median time taken for full crusting was 11 days in the famciclovir group and 10 days in a cyclovir group. According to Shafran et al., [8] the median time for full crusting was 7 days in both the groups. Our findings are in agreement with Shen et al., The median time taken for complete healing of the lesions in both the groups was 21days. 5 patients in famciclovir group and 4 patients in acyclovir group took more than 21 days. The time taken for complete healing of the lesions in the patients above 60 years, belonging to acyclovir group was considerably faster than the famciclovir group. The median time taken for loss of acute pain in both the groups was 21 days. 9 patients in famciclovir group and 17 patients in a cyclovir group to 3 weeks for loss of acute pain.
Herpes zoster involving right T5 dermatome

Herpes zoster involving left V1 dermatome

Herpes zoster involving left T1 and T2 dermatome

The most common adverse effects reported were dyspepsia (10%), headache (9%), nausea (8%) and constipation (7%) in the decreasing order of frequency.
Both the drugs were well-tolerated with no serious adverse effects. Since postherpetic neuralgia increases with increasing age, we studied the effect of these drugs in patients above 60years of age-group, with respect to the dermatome affected, full crusting, complete healing and loss of acute pain. It was observed that the patients above 60 years of age took considerably longer period for complete healing of the lesion and loss of acute pain i.e., 28 days. However, the time taken for full crusting of the lesion remained same as the lesser age-groups. There was no significant difference between the effects of drugs in different dermatomes in these patients.
The most common complication was hypo and hyperpigmented scars in 25% of the patients, majority of them involving V1 branch of trigeminal nerve.
Describing the effectiveness of acyclovir and famciclovir in preventing PHN
Five percent of our study patients had PHN, 2 of famciclovir group and 3 belonging to acyclovir group. All the 5 patients were in the age group 60-80 years, 3 patients were above 70 years and 2 were in 60-70 years of age-group. Since our study did not include a placebo control; no conclusion can be drawn regarding the effect of both the drugs on PHN. Hence, we could not compare our observation regarding the efficacy of each drug in reducing the duration of PHN.
Conclusion
With the introduction of valcyclovir, which also has a convenient dosage. Comparative study between valcyclovir and famciclovir is suggested.