A Technique Elucidating the Retrieval of an Adhered Cover Screw in a Dental Implant – A Case Report
J. Bhuvaneswarri1, S.C. Chandrasekaran2
1 Senior Lecturer, Department of Periodontics, Sree Balaji Dental College & Hospital, Velachery Main Road, Pallikaranai, Chennai - 600 100. Tamil Nadu, India.
2 Professor & HOD, Department of Periodontics, Sree Balaji Dental College & Hospital, Velachery Main Road, Pallikaranai, Chennai - 600 100, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. J. Bhuvaneswarri, Senior Lecturer, Department of Periodontics, Sree Balaji Dental College & Hospital, Velachery Main Road, Pallikaranai, Chennai - 600 100, Tamil Nadu, India.
Phone: 9962101341, 9994044047,
E-mail: drbhuvana22@gmail.com
Dental implants have become one of the most popular and rapidly growing techniques for replacing missing teeth. While their predictability, functionality, and durability make them an attractive option for patients and clinicians alike, complications can arise at any stage from patient assessment to maintenance of therapy. Failure of dental implants not only occurs due to biological factors, like unsuccessful osseointegration or peri-implantitis but may also occur due to technical complications like, failures of implant-supported restorations relating those from the implant components, and those relating to the prosthesis. Technical problems related to implant components include abutment screw fractures and cover screw fractures. In this case report we have elucidated an adhered cover screw in an implant.
Dental Implant, Cover screw, Implant failure
Case Report
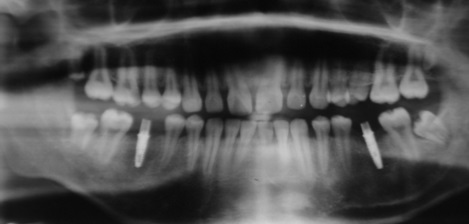
A 20-year-old male patient reported to the Department of Periodontology & Oral Implantology with the complaint of missing teeth in lower back teeth region. On thorough clinical and radiological evaluation of edentulous space in relation to 36 and 46, it was decided place two 2-piece implant* (4.2 x 13 mm) in both the sites [Table/Fig-1 and 2]. [Table/Fig-3] radiograph showing implant in 36 region.

After implant placement in 36
Post-operative radiograph

Surgical Procedure
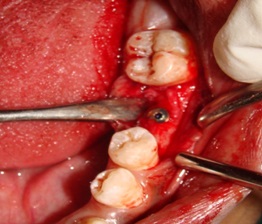
Surgical procedure was planned, after an uneventful healing period of three months. Second stage surgery was performed and abutment was attached to implant in relation to 46 [Table/Fig-4]. Difficulty was encountered in unscrewing the cover screw of implant in relation to 36 with a hex driver (1.22S) and the driver started to slip in the hex slot of the cover screw [Table/Fig-2 and 3]. Decision was made to make a straight slot on the cover screw to engage the straight screw driver (1.22L) [Table/Fig-5]. The slot was made by grooving the cover screw with a diamond tapering fissure bur [Table/Fig-6]. The cover screw was retrieved easily using the straight screw driver [Table/Fig-7]. The retrieved cover screw [Table/Fig-8]. After removal of cover screw [Table/Fig-9]. The abutment was placed in 36 and 46 [Table/Fig-10 and 4] & implant restored to function [Table/Fig-11].
Radiograph showing Abutment fixed in 36,46
Hex driver used to remove the cover screw

Groove is made using a tapering fissure bur



After removal of cover screw



Discussion
The presented situation illustrates some of the complications inherent in the utilization of implant components. The method of perforating the fragment first and achieving retention to unscrew it afterwards was successful.
However, the method is complex and difficult for routine application because the procedure can be time-consuming and involves the risk of damaging the threads inside the implant. The success achieved with the repair system that may be unpredictable and dependent upon the individual situation. The drill guides should be positioned with great care. Screwing out the cover screw was advantageous because the implant threads remained intact. The ultimate aim of a routine recall system is to avoid complications such as screw or abutment fractures. However, their occurrence may represent an early warning sign. For this reason, it is essential not only to retrieve the fractured component but also to determine the reason for failure and to modify it if necessary. Regular recall appointments might prevent further cover screw fractures, as problems could be diagnosed and treated earlier.
Fractured screws generally are challenging to remove. The technique described in this article involves the use of inexpensive instruments commonly found in dental offices. The force required to remove the adhered screw is minimal provided that the screw threads have not been damaged previously.
The primary reason for screw fracture is undetected screw loosening, which can be due to bruxism, an unfavorable superstructure, overloading, or malfunction [1–3]. Therefore, the number, position, dimension, and design of implants, as well as the design of the prosthesis, are critical factors to be considered during the treatment planning phase. To withstand high bending stress, implants should be as long and as wide as possible, used in adequate numbers, and have a position which allows axial loading. Implant components are known to fracture more frequently in the posterior region and in partially dentate patients compared to completely edentulous patients [4–7].
Conclusion
Using the described technique, implant cover screw was successfully removed. Nevertheless, the aim of treatment should be to avoid entrenched of implant cover screw and to use the described repair procedure only in necessary circumstances. This technique can be used only in exceptional clinical situation. Avoiding such clinical situation is prime treatment modality.
*Uniti Implant.
[1]. Williamson Russell T, Robinson Fonda G, Retrieval technique for fractured implant screwsJ Prosthet Dent 2001 86:549-50. [Google Scholar]
[2]. Luterbacher S, Fourmousis I, Lang NP, Bragger U, Fractured prosthetic abutments in osseointegrated implants: a technical complication to cope withClin Oral Implants Res 2000 11:163-70. [Google Scholar]
[3]. Mollersten L, Lockowandt P, Lindén LA, Comparison of strength and failure mode of seven implant systems: an in vitro testJ Prosthet Dent 1997 78:582-91. [Google Scholar]
[4]. Bragger U, Aeschlimann S, Bürgin W, Hammele CH, Lang NP, Biological and technical complications and failures with fixed partial dentures (FDP) on implants and teeth after four to five years of functionClin Oral Implants Res 2001 12:26-34. [Google Scholar]
[5]. Green NT, Machtei EE, Horwitz J, Peled M, Fracture of dental implants: literature review and report of a caseImplant Dent 2002 11:137-43. [Google Scholar]
[6]. Taylor TD, Agar JR, Vogiatzi T, Implant prosthodontics: current perspective and future directionsInt J Oral Maxillofac Implants 2000 15:66-75. [Google Scholar]
[7]. Schenk RK, Buser D, Osseointegration: a realityPeriodontol 2000 1998 17:22-35. [Google Scholar]