Mandibular Second Molar with a Single Root and a Single Canal: Case Series
Anna Roy1, Natanasabapathy Velmurugan2, Nandhini Suresh3
1 Senior Lecturer, Deparment of Endodontics, Meenakshi Ammal Dental College and Hospitals, Chennai, India.
2 Professor, Deparment of Endodontics, Meenakshi Ammal Dental College and Hospitals, Chennai, India.
3 Reader, Deparment of Endodontics, Meenakshi Ammal Dental College and Hospitals, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Anna Roy, Senior Lecturer, Meenakshi Ammal Dental College and Hospitals, No.1, Railway Colony, Second Street, Nelson Manickam Road, Chennai–29, India.
Phone: +91-9840095544;
E-mail: annaroy83@gmail.com
The variability of root canal system morphology of multirooted teeth represents a continuous challenge to endodontic diagnosis and therapeutics. This report extends the range of known possible anatomical variations to include teeth with lesser number of root and root canals. Variations of root canal systems need not always be in the form of extra canals. Clinicians should be aware that there is a possibility of existence of fewer number of roots and root canals than the normal root canal anatomy. Thus the aim of this article is to present three cases of endodontically managed mandibular second molars with a single root and root canal.
Mandibular second molar, Root canal morphology, Single canal, Single root
Case Report
In this article, we report three cases of endodontic management of a mandibular second molar with a single conical root and a single canal. In all the three cases, a diagnosis of acute irreversible pulpitis was made and the teeth were endodontically treated. Patient’s informed consent was obtained in each case before executing the treatment plan. The pre operative radiograph revealed a fused conical root [Table/Fig-1A]. Hence, multiple preoperative radiographs in various angulations were taken, that revealed a single root and a single root canal. Standard access cavity was prepared that uncovered a huge canal orifice at the center of the pulp chamber. The canal patency was established with a suitable ISO K file. Working length was determined with the help of electronic apex locater (Root ZX) and confirmed using a radiograph. Cleaning and shaping was done using a step back technique using suitable sized ISO K file. 2.5% sodium hypochlorite solution and saline were used for irrigation and recapitulation. 17% aqueous EDTA solution was used as a final flush. The canals were dried with sterile absorbent points and then coated with AH plus sealer with lentulo-spirals and obturated with gutta-percha using cold lateral compaction technique [Table/Fig-1B & C]. Follow up was done for 1 year and the patients were found to be asymptomatic.
Preoperative radiograph of the left mandibular second molar
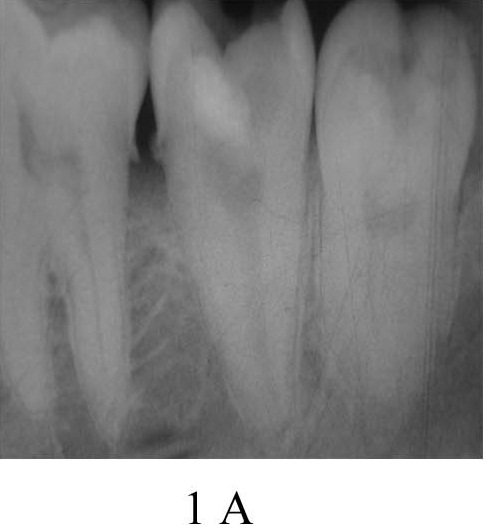
Radiograph with Master cone in position
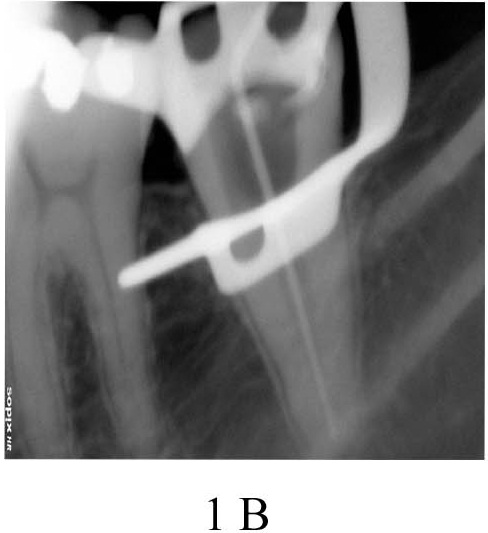
Post obturation radiograph

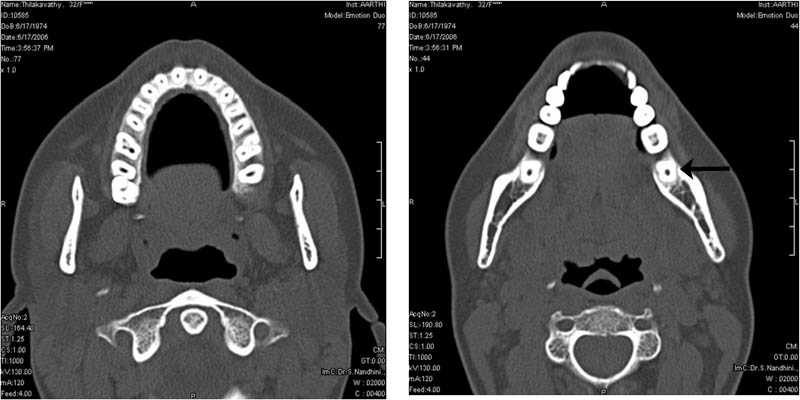
The first case presented a mandibular left second molar. Radiographs of the contralateral and the maxillary second molars also revealed a single fused root. Spiral CT was taken to confirm the radiographic finding, which confirmed the presence of a single root and a single canal in all the four second molars [Table/Fig-2].
Spiral CT Slice showing a single root canal in all the four second molars
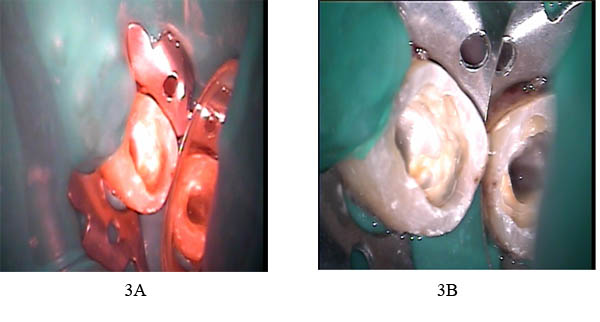
The second case was a mandibular left second molar. Contralateral and the maxillary left second molar were missing as it was extracted due to dental caries. Maxillary right second molar had three roots. The access cavity was viewed under a surgical operating microscope (Seiler, Revelation) under various magnifications (3X, 5X) and this confirmed the presence of only a single wide canal [Table/Fig-3].
View of a single wide canal orifice
The third case was a mandibular right second molar. Radiographs of the contralateral and the maxillary second molars and the panoramic radiograph revealed a single fused root [Table/Fig-4].
OPG showing a single root canal in all the four second molars

Discussion
The variation of root canal morphology, especially in multirooted teeth, is a constant challenge for diagnosis and successful endodontic therapy. Complete knowledge of the root canal anatomy and its most frequent changes is essential, as the non treatment of one canal can lead to endodontic failure. Variations in canal morphology such as extra canals, apical ramifications, apical deltas, or lateral canals are commonly encountered and their incidence and significance have been well documented [1].
It has been observed that the occurrence of abnormal anatomy can occur in any racial groups depending on various factors like age, sex and ethnicity that play a role in determining the pattern of the root canal. Multiple angled radiographs aid in the diagnosis of canal abnormalities. One of the commonest reported variations occurring in the mandibular second molar is the presence of C-shaped canals. Root fusion that becomes a single root, conical or C-shape form, has an incidence of about 21.8 percentage. The other variations include the presence of two or four canals instead of the commonly occurring three canals, supernumerary roots, taurodontism [2], additional or lesser number of canals in one or more of the roots.
Recently, Gopi Krishna et al., reported a case of maxillary first molar with a single root and single root canal which was identified using spiral CT [3].
Some of the common iatrogenic errors during access opening errors are caused during the search for the missing or extra canals. Such iatrogenic errors can be minimised if the clinician has the knowledge of the general location and dimensions of the pulp chamber. Although extra canals are more common, the clinician should be aware of the fact that in certain cases, there is a possibility of fewer canals than the normally presumed canal morphology.
Usually, the mandibular second molars have two mesial canals (MB and ML) and one distal canal similar to the mandibular first molars [4]. However, Slowey et al., reported that the mesial roots of the mandibular second molar has a higher incidence of one canal (14%) wherein they may have a common foramen or may exit separately as two or more foramina [5].
In all the 3 cases, multiple preoperative radiographs were taken and it revealed a single root and a single root canal. In the first case, the presence of a single canal was confirmed using spiral CT. Although CBCT has increased accuracy with higher resolution, reduced scan time and lesser radiation dose, due to its limited availability and medico legal consideration, spiral CT was opted. In the other two cases, access cavity was viewed under a surgical operating microscope revealed a huge canal orifice at the center of the pulp chamber.
Literature search has shown that the presence of a single canal in all four second molars is very rare. Fava et al., [6] reported the presence of one single root and one root canal in all second molars of the same patient, which was confirmed using radiographs recently.
When only one root is present, the root canal system may present with only a single broad root canal or two canals that may or may not join, or a C-shaped canal. Pansiera & Milano [7] studied 102 extracted human mandibular second molars and described six teeth (5.88%) possessing one root and one root canal.
Sabala et al., [8] stated that the more rare the aberration, the more probable that it was bilateral. As bilateral anatomic discrepancies are usually found, the clinician should suspect its presence on the contralateral pair when viewing the initial radiograph.
Conclusion
The anomalies in the root canal morphology need not always be extra canals. It can also be in the form of fused or fewer canals. From a clinical standpoint, when an unusual anatomic form is encountered, multiple angled radiographs of the tooth in concern will reveal more details of the anatomy of the root canal system.
[1]. Jung IY, Seo MA, Fouad AF, Apical anatomy in mesial and mesiobuccal roots of permanent first molarsJ Endod 2005 31:364-8. [Google Scholar]
[2]. Sert S, Bayirli GS, Taurodontism in six molars: a case reportJ Endod 2004 30:601-02. [Google Scholar]
[3]. Gopikrishna V, Bhargavi N, Kandaswamy D, Endodontic management of a maxillary first molar with a single root and a single canal diagnosed with the aid of spiral CT : a case reportJ Endod 2006 32(7):687-91. [Google Scholar]
[4]. Sert S, Bayirli GS, Evaluation of the root canal configuration of the mandibular and maxillary permanent teeth by gender in the Turkish populationJ Endod 2004 30(6):391-8. [Google Scholar]
[5]. Slowey RR, Root canal anatomy. Road map to successful endodonticsDent Clin North Am 1979 23:555-73. [Google Scholar]
[6]. Fava LR, Weinfeld I, Pais CR, Four second molars with single roots and single canals in the same patientInt Endod J 2000 33(2):138-42. [Google Scholar]
[7]. Pansiera AF, Milano NF, Morfologia endodoÃntica dos segundos molares inferioresRevista da Faculdade de Odontologia de Porto Alegre 1995 36:12-14. [Google Scholar]
[8]. Sabala CL, Benenati F, Neas BR, Bilateral root and root canal aberrations in a dental school patient populationJournal of Endodontics 1994 20:38-42. [Google Scholar]