We conducted this study to estimate salivary amylase levels in non-insulin dependent diabetes mellitus patients. With the results which we obtained, we wanted to analyze the changes in salivary amylase levels in non diabetic and diabetic individuals and possibility of using salivary amylase as an indicator of increased glucose levels.
Material and Methods
This study was conducted at Sree Balaji Dental College and Hospital in association with Bio-Line Laboratory, Chennai, India. The study samples consisted of 60 individuals who included both males and females. Non-insulin dependent diabetes mellitus patients and the same number of healthy individuals of the age group of 30-60 years were included. All patients were from different socio-economic status.
Ethical Clearance
Ethical clearance was obtained from the institutional ethical committee, Chennai, before the study was started. The nature and purpose of the study were briefly explained to each participating patient/subject and their written consent was obtained.
Inclusion Criteria
Patients diagnosed as diabetic by medical faculty, who had elevated blood glucose levels, were included. The second group consisted of non-diabetic individuals.
Exclusion Criteria
Patients having severe diabetic complications, other systemic illness and those who were under medication for other diseases, were excluded from this study.
Clinical Examination
General and oral examinations of the patients and control subjects were recorded and their case histories were taken.
During the clinical examination, the following elements were analyzed.
Gingival status
Periodontal condition
Xerostomia
Dental caries
Collection of Saliva
Salivary samples were collected in the morning. The diurnal variation of saliva is very low during this time. After making the subjects rinse their mouths thoroughly with water, salivary samples were collected in sterile containers by instructing them to allow saliva to collect naturally in mouth and to expectorate it, into the containers. The samples were immediately taken for biochemical analysis.
Collection of Blood
Antecubital venous blood samples were taken after 12hrs of overnight fasting. The collected samples are used for the estimation of blood glucose and HbA1c levels. The estimation of blood glucose was done by GOD-POD method.
Estimation of salivary amylase activity was determined by the direct substrate method (kinetic enzyme assay). The ability of alpha amylase to catalyze the hydrolysis of starch to maltose is the principle used to estimate amylase. The saliva was collected, it was diluted to 1 in 100 ( 1 part of saliva and 99 parts of saline ) and it was added to the reagent ( ready to use liquid kit ). The sample ( saliva ) reagent was placed in a sample cap and it was analyzed in an automatic analyzer.
Results
The significant differences between the mean scores regarding the age, fasting blood sugar (mg/dl), post prandial blood sugar (mg/dl), HbA1c(%) and salivary amylase (u/l) were analyzed using the inferential statistics of Student’s t–test, after verifying the normality assumption by Q-Q plot technique. The results have been given in [Table/Fig-1].
Test for Mean score analysis w.r.t group of patients
| Group | n | Mean | SD | SE | t | p |
|---|
| Age (yrs) | Diabetes | 33 | 47.21 | 7.817 | 1.36 | 0.412 | 0.682 |
| Non Diabetes | 34 | 46.44 | 7.500 | 1.29 |
| Fasting blood sugar (mg/dl) | Diabetes | 33 | 173.88 | 72.02 | 12.54 | 6.79 | < 0.00** |
| Non Diabetes | 34 | 89.21 | 9.84 | 1.69 |
| Post-prandial blood sugar (mg/dl) | Diabetes | 33 | 247.88 | 86.37 | 15.04 | 3.47 | 0.001** |
| Non Diabetes | 34 | 141.62 | 154.08 | 26.42 |
| HbA1c (%) | Diabetes | 33 | 7.79 | 1.15 | 0.20 | 11.84 | < 0.00** |
| Non Diabetes | 34 | 5.15 | 0.60 | 0.10 |
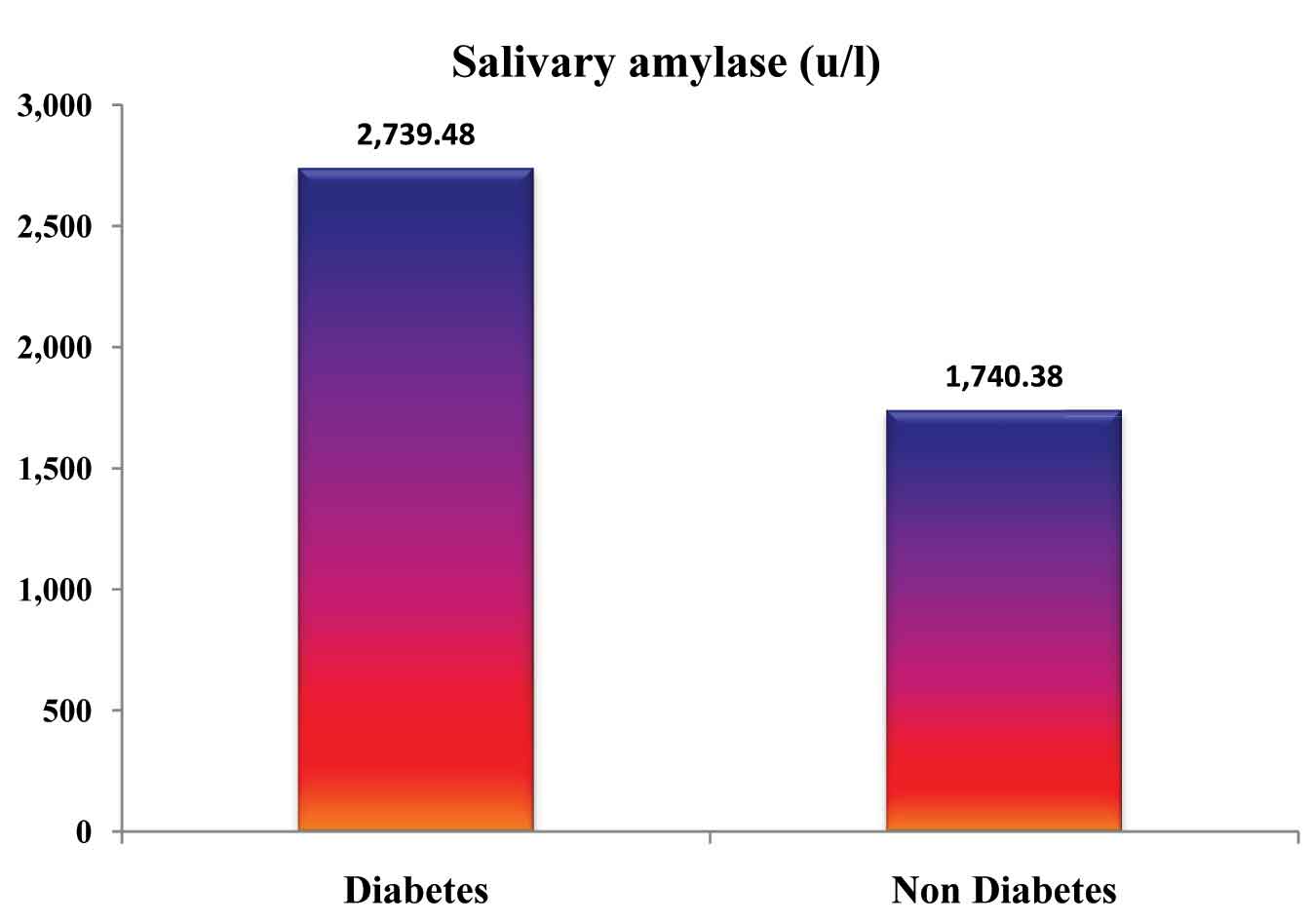
| Salivary amylase (u/l) | Diabetes | 33 | 2,739.48 | 1,525.20 | 265.50 | 3.52 | 0.001** |
| Non Diabetes | 34 | 1,740.38 | 638.51 | 109.50 |
** Highly Significant (Sig. at 1%)
The fasting blood sugar, postprandial blood sugar and HbA1c of the diabetic patients in our study showed highest mean scores and the p value which was obtained was less than 0.05.
The salivary amylase estimation showed highest mean scores among the diabetic patients than among the non-diabetic patients in our study and the p value was less than 0.05 [Table/Fig-2].
Mean score of salivary amylase among diabatic and non-diabatic patients
The selected parameters were estimated and means ± SD of the various parameters in non-insulin dependent diabetic patients are as follows:
Variables Mean (± SD)
Fasting blood glucose 0.970 mg/dl
Post–prandial blood glucose 0.881 mg/dl
Salivary Amylase 0.767 u/l
HbA1C 0.467%
Mean blood glucose in diabetic individuals was significantly higher than that in control group.
Mean salivary amylase in diabetic individuals was significantly higher than that in control group.
Mean HbA1C in diabetic individuals was significantly higher than that in control group.
In diabetic patients, there is a significant linear relationship between blood glucose and salivary amylase.
Discussion
Diabetes is a genetically and clinically heterogeneous group of disorders that share glucose intolerance in common.
The present study was conducted to estimate the salivary amylase levels in non- insulin dependent diabetes mellitus patients and to compare the values with those of normal individuals, to use salivary amylase as a bio-chemical indicator to diagnose diabetes mellitus and also to monitor such patients.
The oral findings of 30 non-insulin dependent diabetic patients revealed 7 patients with poor oral hygiene and halitosis and 12 patients showed periodontitis. Paresthesia, xerostomia and burning sensation were presented in 2 patients and 1 patient had oral Candidiasis. Rest of the patients showed mild to moderate gingivitis.
Xerostomia (dry mouth) occurring in diabetic patients can be multifactorial, either due to infiltration of fat cells into the salivary glands or physical alteration of mucosal cells, subsequent to dehydration caused by polyuria or microvascular disease, local inflammation and irritation in the oral cavity, infections, metabolic disturbances and neuropathy affecting salivary glands and it may also be caused by drug therapy given for diabetes. The finding of xerostomia was consistent with the findings of studies conducted by She-Fen Chaung et al., [3], Busato IM et al., [4], Paul A.Moore et al., [5].
A significant increase in salivary amylase levels among diabetic patient in our study group was consistent with the findings of previous studies done by Prabal Pal et al., [6]. Our study correlated with their study in significance level of p<0.01.
Sathyapriya et al., [7], in their research done on the potential of salivary protein as a biomarker in prognosis of diabetes mellitus, found that mean salivary glucose levels were higher in the uncontrolled and controlled diabetic groups than in the healthy non-diabetic group and that the differences were highly significant.
The salivary amylase levels were significantly higher in controlled diabetics as compared to those in healthy non-diabetics. Our study correlated with their study in significance levels of p<0.05.
Maria Elena lopez et al., [8], in their study done on salivary characteristics of diabetic children, gave the inference that salivary protein and salivary amylase increased in diabetics than in controls.
Prabal Pal et al., [7], in their study done on estimation of salivary glucose, salivary amylase, salivary total protein and periodontal micro flora in saliva of diabetic patients, concluded that salivary amylase caused increased accumulation of plaque in the interdental areas and that it increased concentration of salivary glucose in diabetic individuals. It also favoured proliferation of both aerobic and anaerobic bacteria in the gingival plaque of diabetic individuals.
Scannapieco et al., [9], in their study, showed that increased salivary amylase promoted adhesion of oral Streptococci to hydroxyapatite, thus supporting the role of salivary amylase as a potential factor in Streptococcal adhesion to teeth and in plaque formation.
Decrease in salivary flow rate or oral dryness occurring in diabetes can be multifactorial, either due to infiltration of fat cells into the salivary glands or due to physical alteration of mucosal cells, subsequent to dehydration caused by polyuria or microvascular disease, local inflammation and irritation in the oral cavity, infections, metabolic disturbances and neuropathy affecting salivary glands and it may also be caused by drug therapy given for diabetes.
Arati S. Panchbhai et al., [10], Prabal Pal et al., [7], Conner S. et al., [11], Straka M. [12] and Hanna-Leena Collin [13] had mentioned increased caries activity in diabetic patients, which was also seen in our study.
In our study, the poor glycemic control determined by the HbA1c values also indicated increased salivary glucose and salivary amylase levels.
Conclusion
The present study included critical salivary parameters, namely fasting, post prandial salivary amylase and HbA1c levels, in order to study the effects of diabetes on salivary composition. The study also gave due consideration to the levels of metabolic control, duration and type of diabetes mellitus and gender. In addition, the study focussed on most possible interrelationships among the variables.
Like our study, several studies have confirmed that salivary amylase caused increased accumulation of plaque in the interdental areas. Increased concentration of salivary glucose in diabetic individuals also favoured proliferation of both aerobic and anaerobic bacteria in the gingival plaque of diabetic individuals.
As in various studies quoted previously, our study also showed significant increase in the salivary amylase levels in non-insulin dependent diabetic patients. Thus, our study is one such evidence which has been added to previous studies in supporting the use of salivary amylase estimation as a non-invasive procedure for diagnosing and monitoring the blood glucose levels. The present study had a small sample size, but it made some novel observations which will unquestionably provide a platform for further research.
** Highly Significant (Sig. at 1%)