Guiding Intellect for Occlusal Errors
Mansi Patel1, Ponnanna A.A.2, Gaurav Tripathi3
1 Post Graduate Student, Department of Prosthodontics, Pacific Dental College, Udaipur, Rajsthan, India.
2 Head of Department, Department of Prosthodontics, Pacific Dental College, Udaipur, Rajsthan, India.
3 Post Graduate Student, Department of Prosthodontics, Pacific Dental College, Udaipur, Rajsthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Gaurav Tripathi, Post Graduate Student Department of Prosthodontics Pacific Dental College Airport Road Udaipur, Rajsthan–313024, India.
Phone: +91-8233860303;
E-mail: dr.gauravtitan23@gmail.com.
Purpose: The purpose of the study is to quantify occlusal errors seen, during the processing of complete denture.
Material and Methods: Maxillary and mandibular complete dentures were fabricated for 30 subjects. Anterior and posterior markings were made on articulator and the distance was measured from these points before and after processing of complete dentures. Occlusal errors following processing of complete dentures was determined by subjecting the values obtained to statistical analysis using paired t-test.
Results: The results indicated the existence of discrepant amount of occlusal errors following processing of complete denture and statistical test applied was paired t-test, p-values obtained are, p=0.00 anterior reference markings and p=0.006 for posterior reference markings (p ≤ 0.001 highly significant).
Conclusion: The processing errors are inevitable. Hence for patient comfort, laboratory remounting is an important procedure that needs to be followed as a regular step after processing of each and every denture.
Occlusal error, lab remounting, acrylic resin, complete denture
Introduction
Complete dentures are prosthetic replacements which are fabricated to restore impaired functions and appearance. Fabrication of complete dentures comprises clinical and laboratory procedures, whose precise execution is of crucial importance for achieving success [1]. Well made dentures enable the patient to have comfort, adequate function, and an appearance that is unanimously accepted. The comfort of well- made dentures is derived from an accurate tissue morphology and adaptation of dentures for proper fit. The occlusion established is a result of the record utilisation and careful attention to laboratory procedures. Complete dentures are designed so that their occlusal surfaces permit both functional and parafunctional movements of mandible and patient’s functional amenity, this occlusion is established at a vertical dimension that will maintain the muscular tonicity indicative of good esthetics [2].
Fabrication of dentures involves many separated but related procedures regardless of the techniques or instruments used for making impression, making jaw relation records, arranging teeth in balanced occlusion and processing the dentures. An error in any one of the procedure contribute to error in the occlusion of complete denture. The inaccuracies of the material and methods used to fabricate dentures at this stage must be recognised and eliminated before the patient wears the denture. These errors can result of:
Technical errors or errors made by the dentist.
Technical errors developed during the laboratory procedures.
Inherent deficiencies of the materials used in the construction of the dentures.
The occlusal errors may result from variety of reasons including change in state of health of temporomandibular joints, inaccurate maxillomandibular relation record made by the dentist, errors in transfer of the maxillomandibular relation records to the articulator, ill-fitting temporary record bases, failure to use facebow and subsequently changing the vertical dimension on the articulator, incorrect arrangement of posterior teeth. However these clinical errors can be avoided by a skillfull dentist. Whereas the error caused during processing of denture is primarily when the denture base material shrinks, when it changes from mouldable to solid form by polymerisation and also from wearing of the finished dentures in the mouth (expansion of the acrylic resin due to water absorption).
Each of these procedure offers the possibility of an undetected error that might not be noted until the denture are placed in patient’s mouth. Failure to correct occlusal errors before the patient wears the denture, results in destruction of residual alveolar ridge as bone in time will remodel to relieve soft tissue subjected to excess pressure caused by occlusal errors. Errors in occlusion can be corrected by clinical remounting and laboratory remounting. Processing error can be eliminated by laboratory remounting. It is a procedure by which the processed dentures are mounted on the articulator to correct occlusal errors resulting from denture processing. Clinical Remount is defined as a procedure where occlusal refinement is carried out on the articulator after remounting the dentures with new records obtained from the patient [3].
In 1972, a survey of dental students and practitioners in Great Britain revealed that routine use of remounting on an articulator and adjusting the occlusion of complete dentures is rare. Only 6.5% of general practitioners usually remounted the dentures to adjust the occlusion [4]. Levin in 1985, conducted a survey of complete denture procedures taught in 32 US and Canadian schools which showed that the majority of schools are teaching the examination of mucosal adaptation of dentures with disclosing paste and the perfection of occlusion at the insertion appointment by clinical remounting records [5].
Firtell in 1987 conducted a study in which he examined thirty patients with complete dentures. Out of them 15 were treated with a clinical remount and other 15 without clinical remount. The occlusal patterns of all dentures were recorded in the patient’s mouths at insertion and again 1 week later by using a photoelastic membrane to provide a permanent record. The presence or absence of soreness was also noted for each patient during the week after insertion. He concluded that clinical remount significantly reduced the incidence of soreness, preserved the occlusal force, and reduced the changes in occlusal patterns of the dentures [6].
Shigli in 2008 concluded a study to identify whether refinement in occlusion was correlated with patient comfort, the number of post-insertion visits and concluded that combination of laboratory and clinical remount procedures with occlusal corrections, enhanced patient comfort, compared to the other groups in which either one or both of the procedures were not performed [7].
Since the processing errors are unavoidable due to the property of the acrylic resin used for fabrication of complete dentures. The purpose of this article is to represent a small study conducted at our institution for revealing the laboratory remount procedure (placing the dentures back into the articulator) as an indispensable part of complete denture fabrication procedures.
Methodology
A cross-sectional study was conducted among 30 patients, aged 50-74 years of complete denture for identifying the effect of laboratory remount procedures on patient’s comfort, who reported to the Department of Prosthodontics, Pacific dental college, Udaipur Rajasthan, India. Approval from the Institution Review Board was obtained prior to the study. Informed consent of subjects was obtained regarding their voluntary participation in the study. Inclusion criteria: adults who were free from any systemic diseases and who provided informed consent. Exclusion criteria: poor residual ridge anatomy, single complete dentures, and temporomandibular joint (TMJ) problems.
Maxillary and mandibular complete dentures were fabricated for 30 subjects (15 women and 15 men) using standardised clinical and laboratory procedures within the institution. Before the flasking procedure was performed markings were made both anteriorly and posteriorly on the articulator and the distance was measured and record was maintained for all 30 subjects [Table/Fig-1].The material used for packing the denture was DPI Heat Cure (Bombay Burmah Trading Corporation, Ltd) and flask used was of Jabbar comp. size no.8, curing cycle was standardized by allowing the flask for bench curing for 45minutes, followed by immersing the flask in cold water, then gradually boiling not less than 30 minutes. Total time for curing the denture was 1 hour. After the denture processed and before insertion the dentures were subjected to laboratory remounting (i.e. the dentures were placed on the articulator on their original plaster mountings using the key (index) in the base of the cast [Table/Fig-2] and the distance was measured again from markings previously made before processing both anteriorly (point A) and posteriorly (point B) [Table/Fig-3]. The readings obtained before and after processing were compared for all 30 subjects and evaluated [Table/Fig-4]. It was noted that there was a distinct variation in the vertical dimension following processing of complete dentures.
key index at base of cast
Distance between posterior markings before processing
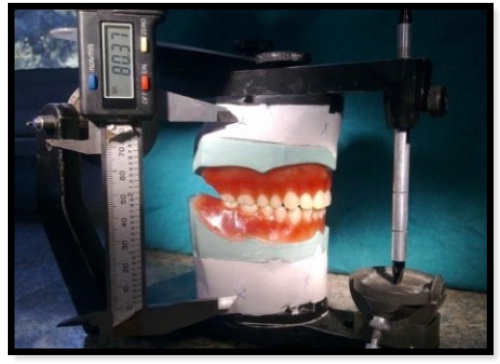
Distance between posterior markings after processing

Errors measured for Laboratory Remounting Procedure
| Sr. No. | Anterior Reference Marking (pt. A) | Posterior Reference Marking (pt. B) |
|---|
| Before Processing | After Processing | Before Processing | After Processing |
|---|
| 1. | 77 mm | 80 mm | 74 mm | 77 mm |
| 2. | 70 mm | 74 mm | 73 mm | 77 mm |
| 3. | 74 mm | 77 mm | 71 mm | 73 mm |
| 4. | 70 mm | 75 mm | 75 mm | 78 mm |
| 5. | 64 mm | 67 mm | 66 mm | 68 mm |
| 6. | 76 mm | 77 mm | 76 mm | 78 mm |
| 7. | 74 mm | 76 mm | 79 mm | 81.5 mm |
| 8. | 73 mm | 75.5 mm | 72 mm | 75 mm |
| 9. | 76 mm | 79 mm | 75 mm | 78 mm |
| 10. | 74 mm | 78 mm | 76 mm | 79 mm |
| 11. | 77 mm | 79 mm | 77 mm | 80 mm |
| 12. | 67 mm | 70 mm | 72 mm | 75 mm |
| 13. | 61.5 mm | 65 mm | 70.5 mm | 72 mm |
| 14. | 68.5 mm | 71 mm | 69 mm | 70 mm |
| 15. | 76 mm | 78 mm | 78 mm | 81 mm |
| 16. | 65 mm | 68 mm | 68 mm | 72 mm |
| 17. | 70 mm | 73 mm | 72 mm | 75 mm |
| 18. | 75 mm | 78 mm | 74 mm | 77 mm |
| 19. | 76 mm | 78 mm | 73 mm | 76 mm |
| 20. | 70 mm | 73 mm | 73 mm | 76 mm |
| 21. | 71 mm | 74 mm | 74 mm | 77 mm |
| 22. | 68 mm | 71 mm | 65 mm | 68 mm |
| 23. | 74 mm | 77 mm | 70 mm | 73 mm |
| 24. | 79 mm | 81 mm | 88 mm | 91 mm |
| 25. | 74 mm | 77 mm | 91 mm | 73 mm |
| 26. | 75 mm | 75 mm | 80 mm | 84 mm |
| 27. | 76 mm | 79 mm | 79 mm | 82 mm |
| 28. | 75 mm | 77 mm | 73 mm | 75.5 mm |
| 29. | 74 mm | 76 mm | 72 mm | 73 mm |
| 30. | 76 mm | 78.5 mm | 79 mm | 82 mm |
The occlusal errors resulted after processing was corrected by selective grinding procedure. It is a procedure of refining occluding surfaces through the use of abrasive materials. Its advantages are (1) Preserves the desired tooth morphology, (2) Type of occlusion. The errors were detected using 100 micron articulating paper. The markings obtained were discriminated as (a) Proper contact – Single dark spot on tooth, (b) Light contact – Faint smudge left on teeth, (c) Premature contact – white spots surrounded by carbon rings or ‘donuts’.
The Sequence for correction of occlusal errors followed was: (i) Restore centric occlusion, (ii) Correct working and balancing occlusion, (iii) Correct protrusive occlusion. Initially contact between heels was check to ensure that increase in vertical dimension is not due to overlying thick denture base resin in these areas. Incisors must be out of occlusion.
For restoring the centric occlusion the teeth are lightly tapped together on articulating paper. In the centric occlusion there are three types of occlusal errors in contact position and each can be corrected by specific grinding:
Any pair of antagonist teeth can be too long and thus hold other teeth out of contact. For correcting this error fossae on teeth are deepened by grinding, so that teeth can occlude each other.
The lower and upper teeth can be placed almost edge-to-edge. For correcting this error cusp inclines are grinded. Buccal inclines of the upper teeth and lingual inclines of the lower teeth are grinded. Central fossae become broader, and by grinding on the palatal side the maxillary palatal cusp is made narrower, and the mandibular buccal cusp is narrowed by grinding on the buccal side.
The upper teeth can be positioned too bucally in relation to the lower teeth. For correcting this error the maxillary lingual cusp is narrowed by broadening the central fossae, and the mandibular buccal cusp is grinded bucally by broadening the central fossae. Actually, the palatal cusp is grinded in the palatal direction and the mandibular buccal cusp in the buccal direction so that teeth can enter each other.
Reduce the teeth until the incisal pin touches the incisal guide table and uniform contact exists on all posterior teeth. Anterior teeth should not touch in centric occlusion [3].
Working side Occlusal Errors and their Correction
On the working side there are six types of occlusal errors. It’s a rule that the centric holding cusps are not grinded. These are: Maxillary lingual cusps and Mandibular buccal cusps. These cusps are essential to maintain the recorded vertical dimension.
If interferences exists in the working side reduce either the “Maxillary buccal cusps lingual inclines or the Mandibular lingual cusps buccal inclines.” This is called B.U.L.L. rule
The maxillary buccal cusp and the mandibular lingual cusp are too long. For correcting this error the length of the cusp is reduced by grinding in order to change the incline extending from the central fossae to the cusp tip. The central fossae are not deepened, but the maxillary buccal cusps and the mandibular lingual cusps are reduced so that the other tooth is in contact in this position.
The buccal cusps are in contact, but the lingual are not. For correcting this error the maxillary buccal cusps are ground from the central fossae to the cusp tip in order to reduce the cusp and to change the lingual cusp incline to become less steep.
The lingual cusps are in contact, whereas the buccal are not. For correcting this error the mandibular lingual cusps are reduced by grinding their buccal incline. The maxillary palatal cusp is not reduced, and the central fossae is not deepened.
The maxillary buccal or palatal cusps are positioned more mesially from their intercuspal position. This error can occur together with any of these three errors already described. For its correction the mesial inclines of the maxillary buccal cusps are ground distally as if they were narrowed, and the distal inclines of the mandibular cusps are ground forwards. In this way the same cusp incline is obtained.
The maxillary buccal or lingual cusps are positioned more distally from their intercuspal position. This error can also occur together with buccolingual errors. For its correction grinding is performed on the maxillary cusps distally and on the mandibular cusps mesially.
The teeth on the working side can be out of contact. The cause of this error is an intense contact on the non–working side.
Non-working side Occlusal Errors and their Correction
The contact on the non–working side is so intense that teeth on the working side are out of contact. For correcting this error pathways are ground over the mandibular buccal cusp in order to reduce the incline of the part of the cusp that prevents tooth contacts on the working side. Each interfering cusp is preserved as much as possible. Grinding is not performed on the lingual cusps that can be included in this contact.
Protrusive Contacts and their Correction
If the anterior teeth have heavy contact with no contact on the posterior teeth.
Correction: Grind the labial surface of the lower anterior and the palatal surface of the upper anterior.
If heavy posterior contact exists with no anterior contact
Correction: reduce the distal inclines of the maxillary cusps and the mesial inclines of the mandibular cusps.
Results
After processing, the dentures along with the cast were mounted back to the articulator. Distance was measured from the points A (Anterior marking) and B (posterior marking) before and after processing and measurements obtained were evaluated using paired t-test. The values obtained are listed in [Table/Fig-4] for 30 complete denture patients.
The mean and standard deviation for dentures before and after processing for anterior reference markings are 72.53mm, 75.23mm and 4.28mm, 3.97mm respectively. For posterior reference marking the mean and standard deviation obtained before and after processing is 74.48mm, 76.56mm and 5.53mm, 4.85mm respectively. The mean difference and p-value for complete dentures before and after processing is illustrated in [Table/Fig-5]. Here p-value obtained for anterior and posterior reference markings, before and after processing are 0.000 and 0.006 respectively, indicating highly significant results thus elucidating marked discrepancy following processing of complete dentures.
Mean difference and p-value for complete denture before and after processing
| Sr. No. | Before and After processing difference | Mean difference | p-value |
|---|
| 1 | Anterior reference point | -2.7000 | .000* |
| 2 | Posterior reference point | -2.0833 | .006* |
*p ≤ 0.001 (highly significant)
Discussion
There are some factors pertaining to the functional harmony of the complete dentures, the most important of which are the occlusal surfaces. Therefore, if the occlusal contacts are not even through the entire arch, the main goals of the prosthetic therapy will not be achieved [2]. In the present study, significant results was evaluated following processing of complete denture showing distinct occlusal errors. As processing errors are unavoidable, therefore it is necessary to correct these errors prior to insertion of dentures. However correction of occlusal errors directly in the patient’s mouth is not accepted, due to mobility of dentures on the soft tissue which obscure the errors and articulating paper will not mark efficiently, unwillingness of patients to cooperate, resulting in incorrect representation of occlusal relationships in maximum intercuspation and excursive mandibular tooth guided movements.
Shigli conducted a study for 30 complete denture subjects and concluded that the combination of laboratory and clinical remount procedures with occlusal corrections decreased tissue irritation, pain during mastication, discomfort during swallowing and mastication, and number of post-insertion [7]. The present study results shows distinct alteration in vertical dimension which need to be corrected before insertion which was done by the laboratory remounting. Advantage of laboratory remounting includes, easily spotted errors on articulator rather than in the patient’s mouth and maintains desired tooth morphology.
Controversies still exist for the correction of occlusal errors. Few authors suggest use of a laboratory remount to remove gross interferences in centric occlusion and recapture the original occlusal vertical dimension and then use of a clinical remount from interocclusal records made in the patient’s mouth. Many authors believe that this procedure should be accomplished before the patient had the opportunity to wear the dentures [8,9]. Woelfel presented different opinion. He did not recommend correcting occlusal discrepancies at the laboratory remounting stage, because “remounting from the mouth will encompass all errors. The occlusal processing error may counteract the dentist’s error in obtaining centric relation and vertical dimension from the patient. He recommended modification of teeth only once by the dentist during the seating appointment [10]. However this results is contradictory to the observations of the Firtell who concluded laboratory and clinical remount procedure essential for patient’s comfort [6].
Limitations of study include small sample size, frequent post-insertion appointments to analyse the results of the remount procedures on the hard and soft tissues were not considered. Errors caused might be because of processing shrinkage, curing cycle, material, technique used.
Conclusion
Processing errors are an inevitable part and hence for patient’s comfort, Laboratory Remounting is imperative step need to be followed after processing of each and every complete denture.
*p ≤ 0.001 (highly significant)
[1]. Badel T, Complete denture remountingActa Stomat Croat 2001 35:381-87. [Google Scholar]
[2]. Boucher’s Prosthodontic treatment for edentulous patient 1980 ed 8St Louis, CVMosby Co:9-13. [Google Scholar]
[3]. Boucher’s Prosthodontic treatment for edentulous patient 1980 ed 9St Louis, CVMosby Co:458-78. [Google Scholar]
[4]. Silverstein JB, Time and methods used for complete denture construction by dental students and general dental practitioners in Great Britain in 1972J Dent 1978 6:196-200. [Google Scholar]
[5]. Levin B, Results of a survey of complete denture procedures taught in American and Canadian dental schoolsJ Prosthet Dent 1985 54:302-06. [Google Scholar]
[6]. Firtell DN, The effect of clinical remount procedures on the comfort and success of complete denturesJ Prosthet Dent 1987 57:53-57. [Google Scholar]
[7]. Shigli M, The effect of remount procedures on patient comfort for complete denture treatmentJ Prosthet Dent 2008 99:66-72. [Google Scholar]
[8]. Basker RM, Prosthetic treatment of edentulous patient 1976 LondonMacMillan Press Ltd:156-61. [Google Scholar]
[9]. Sharry JJ, Complete Denture Prosthodontics 1968 ed 2New YorkMcGraw-Hill Book Co:266-67. [Google Scholar]
[10]. Woelfel JB, Processing complete denturesDent Clin North Am 1977 2:329-36. [Google Scholar]