Salpingitis Isthmica Nodosa: A Case Report
Parasappa Joteppa Yaranal1, Vijayakumar Hegde1
1 Professor, Department of Pathology, Kannur Medical College, Kannur, Kerala, India.
2 Assistant Professor, Department of Pathology, Kannur Medical College, Kannur, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Parasappa Joteppa Yaranal, Professor, Department of Pathology, Kannur Medical College, Kannur, Kerala–670612, India.
Phone: 094488-24484, 08891988809,
E-mail: pjyaranal@yahoo.co.in
Salpingitis isthmica nodosa places the patient at risk for recurrent ectopic pregnancy or infertility. Hence, we report a case of salpingitis isthmica nodosa which was salpingectomized for pain abdomen in a 46- year old woman.
Salpingectomy, Ectopic pregnancy, Fallopian tube
Case Report
Clinical findings: A 42- year female presented to the gynaecology department with history of G3P2L2 and abdominal pain. She had history of 2- months amenorrhea and urine sample was positive for pregnancy test. On examination tenderness in the right iliac fossa and abdominal ultrasonography showed right fallopian tube mass, suggestive of ectopic pregnancy. Clinically diagnosed as ruptured tubal pregnancy, this patient underwent emergency laprotomy and bilateral salpingectomy. No history of previous surgery or tubectomy.
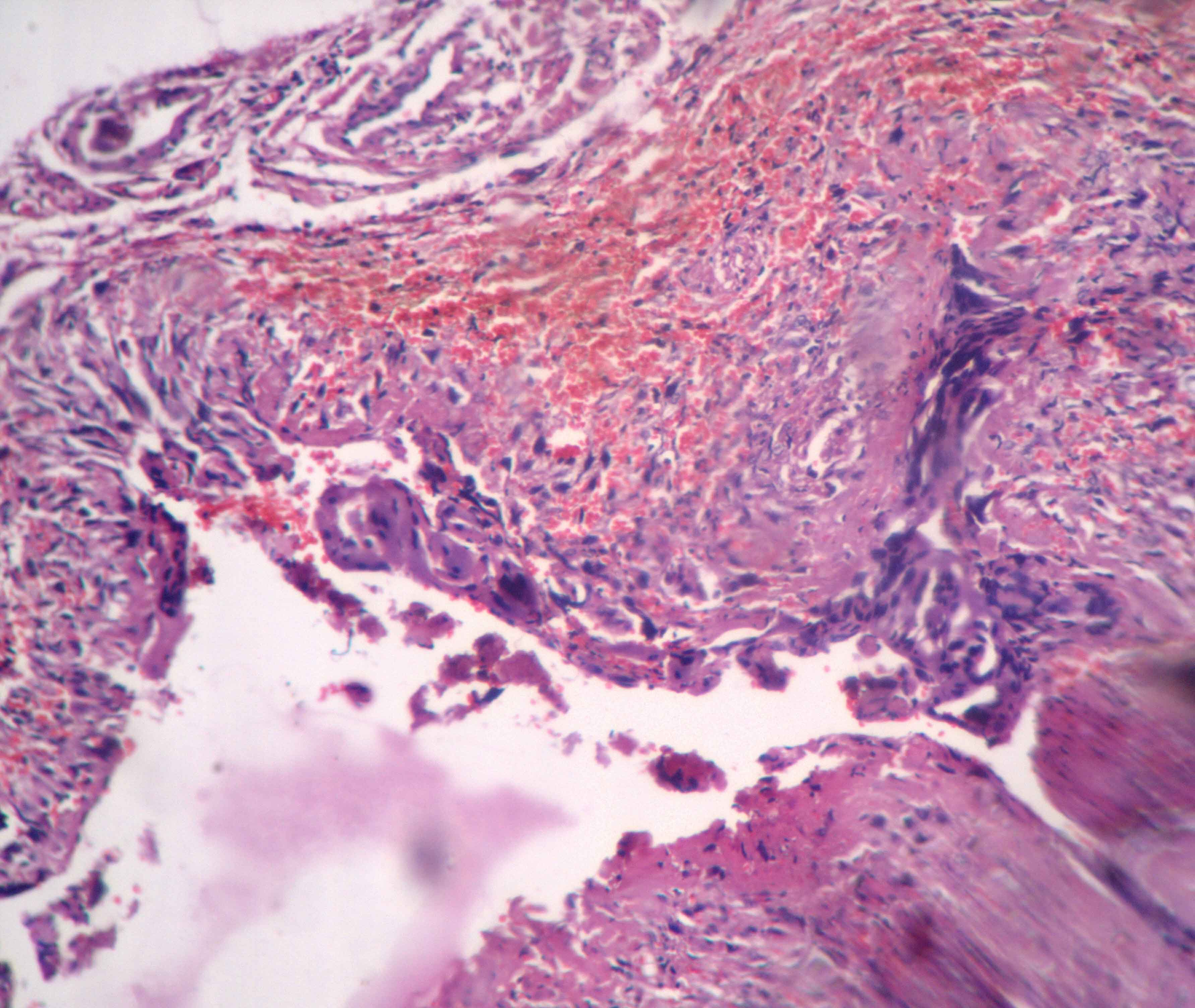
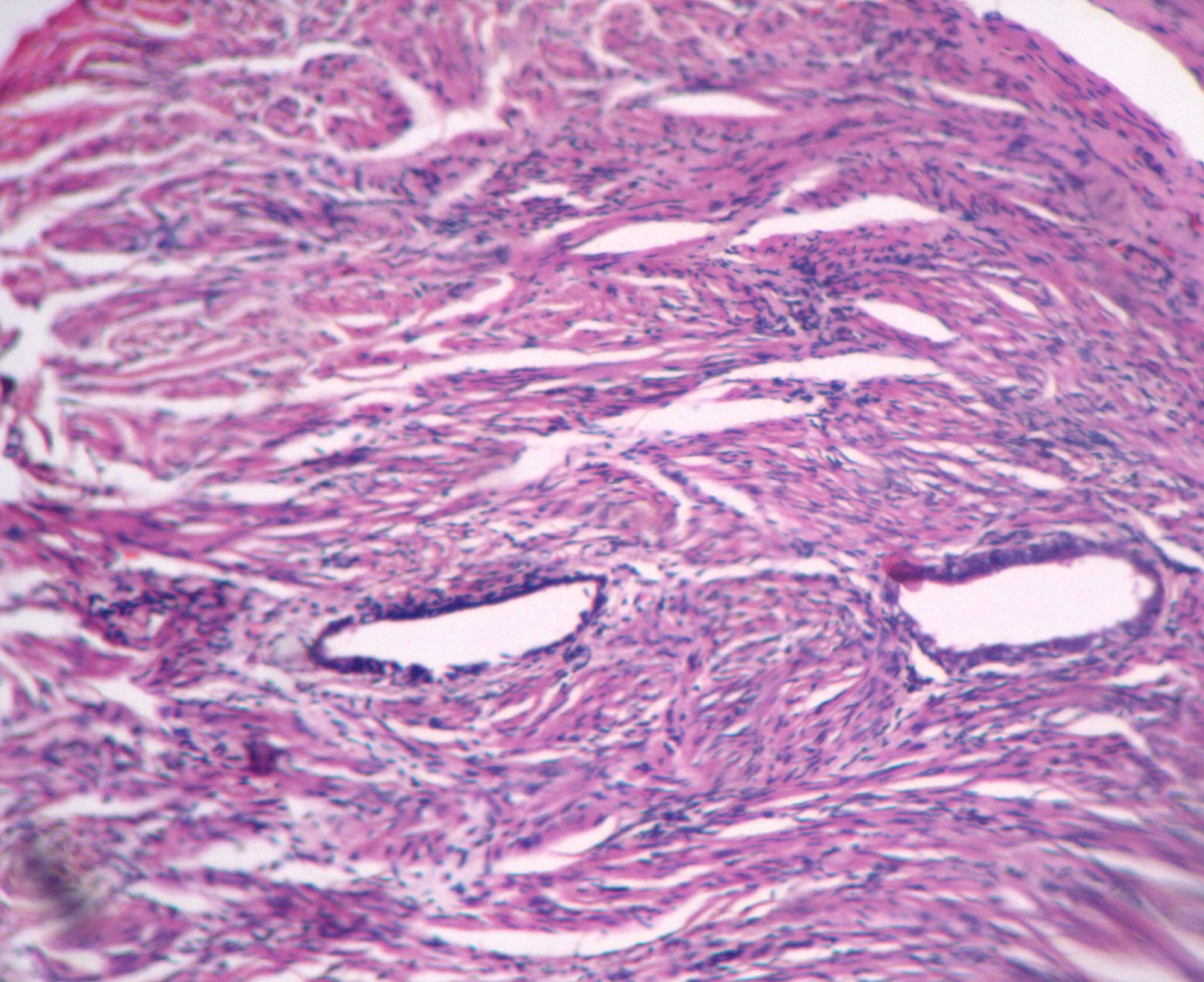
Histopathological findings: Left fallopian tube was 5cms in length and was within normal limits. Right fallopian tube was 7.5cms in length and dilated at distal end with a defect measuring 1x1 cms covered by grey-white exudate. Cut surface showed blood clot with grey brown material in the lumen and wall thickened. The bits were given from the ruptured area and proximal part of the tube. Microscopically distal segment of right fallopian tube showed decidual tissue bits mainly composed of cytotrophoblastic and synctiotiotrophoblstic cells with no chorionic villi [Table/Fig-1]. Proximal (isthmus) portion of tube revealed cystically dilated glands entrapped in hypertrophic muscular layer and the glands were lined by ciliated columnar epithelium [Table/Fig-2]. With these histopathological features, the final diagnosis of isthmic ectopic pregnancy and salpingitis isthmica nodosa was made.
Fallopian tube showing decidual tissue bits with trophoblastic cells. (H & E, x 40)
Cystically dilated glands trapped in the muscular layer (H & E, x 40)
Discussion
Salpingitis Isthmica Nodosa (SIN) is a condition of nodular thickening of the proximal fallopian tube enclosing cystically dilated glands trapped in muscular layer [1,2]. It commonly occurs in the age group of 25 -60 years women with average age at diagnosis being 30 years [1,3]. It is usually bilateral and the patients presents with recurrent ectopic pregnancies and primary infertility [3]. Hysterosalpingography is diagnostic for SIN, shows 2-mm accumulations of contrast medium observed within the diverticula with associated irregularitities in the tubal lumen [1,3,4].
Incidence of SIN in healthy, fertile women ranges from 0.6% to 11%, but it is significantly more common in the setting of ectopic pregnancy and infertility [1].
The aetiology of this condition is unknown. SIN was pathologically first described by Chiari [4] and attributed to be an inflammatory aetiology or adenomyosis-like process [5]. Others proposed congenital Wolffian or mesonephric rests [6], neoplasia [7] or a late result of chronic tubal spasm similar to colonic diverticulosis [8].
The incidence of SIN in the normal population is reported as between 0.6% and 11% [8,9], with the higher incidence in a Jamaican population. It has been associated with ectopic tubal pregnancies with a wide range of incidence (2.8%–57%) [2,8] and in 46% if the isthmic site-specific ectopic pregnancy is considered separately [10]. The association of salpingitis isthmica nodosa (SIN) and isthmic ectopic pregnancy was determined by review of resected tubal segments. SIN was noted in 17 of 37 cases (45.9%) of isthmic ectopic pregnancy. SIN places the patient at risk for recurrent ectopic pregnancy or infertility [11].
Microscopic examination of the tube shows dispersed glands of tubal epithelium surrounded by bands of muscle fibres [10]. On hysterosalpingography, diagnosis of SIN may be confused with tubal endometriosis. However, presence of tubal epithelium lining glands on histopathological examination rules out endometriosis [12].
Conclusion
SIN is significantly associated with the recurrent ectopic pregnancies and infertility; hence, it is important to rule out SIN in such cases.
[1]. Jenkins CS, Williams SR, Schmidt GE, Salpingitis isthmica nodosa: A review of literature, discussion of clinical significance and consideration of patient managementFertil Steril 1993 60:599-607. [Google Scholar]
[2]. Majumdar B, Henderson PH, Semple E, Salpingitis isthmica nodosa: A high risk for tubal pregnancyObstet Gynecol Surv 1983 62:73-78. [Google Scholar]
[3]. Chawla N, Kudesia S, Azad S, Singhal M, Salpingitis isthmica nodosaInd J Pathol Microbiol 2009 52:434-35. [Google Scholar]
[4]. Chiari H, Zur Pathologischen anatomie des EileitZ Heilkd 1887 8:457-64. [Google Scholar]
[5]. Green LK, Kott ML, Histopathologic findings in ectopic tubal pregnancyInt J Gynecol Pathol 1989 8:255-62. [Google Scholar]
[6]. Creasy JL, Clark RL, Cuttino JT, Groff TR, Salpingitis isthmica nodosa: Radiologic and clinical corelatesRadiology 1985 154:597-600. [Google Scholar]
[7]. Bundey JG, Williams JD, Salpingitis isthmica nodosa with tumor formation resembling torsion of an ovarian cystJ Obstet Gynaecol Br Commonw 1963 70:519-22. [Google Scholar]
[8]. Honore LH, Salpingitis isthmica nodosa in female infertility and ectopic tubal pregnancyFertil Steril 1978 29:164-68. [Google Scholar]
[9]. Persaud Y, Etiology of tubal ectopic pregnancyObstet Gynecol 1970 36:257-63. [Google Scholar]
[10]. Wheeler JE, Pathology of the fallopian tubeIn: Pathology of the Female Genital Tract 1982 Berlin Heidelberg New YorkSpringer:403-04. [Google Scholar]
[11]. Homm RJ, Holtz G, Garvin AJ, Isthamic ectopic pregnancy and salpingitis isthmica nodosaFertile Steril 1987 48:756-60. [Google Scholar]
[12]. Karasick S, Karasick D, Schilling J, Salpingitis isthmicanodosa in female infertilityJ Can Assoc Radiol 1985 36:118-21. [Google Scholar]