A Mini Accessory Liver Lobe in the Fissure for Ligamentum Teres and Its Clinical Significance: A Case Report
Satheesha B. Nayak1, Naveen Kumar2, Srinivasa Rao Sirasanagandla3, Surekha D. Shetty4
1 Professor and Head, Department of Anatomy, Melaka Manipal Medical college, Manipal University, Madhav Nagar, Manipal, Karnataka, India.
2 Lecturer, Department of Anatomy, Melaka Manipal Medical College, Manipal University, Madhav Nagar, Manipal, Karnataka, India.
3 Lecturer, Department of Anatomy, Melaka Manipal Medical College, Manipal University, Madhav Nagar, Manipal, Karnataka, India.
4 Lecturer, Department of Anatomy, Melaka Manipal Medical College, Manipal University, Madhav Nagar, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satheesha B. Nayak, Professor and Head, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus) International Centre for Health Sciences Manipal University, Madhav Nagar-576 104, Manipal, Udupi, Karnataka, India.
Phone: +91 9844009059,
E-mail: nayaksathish@gmail.com
The liver can present a number of congenital anomalies. More common among them are the irregularities of the shape and the number of lobules. The less common variations include the presence of accessory lobes or accessory livers. The accessory lobes may be attached to the liver through a mesentery or a bridge of the hepatic tissue and they are usually asymptomatic. An accessory liver lobe is a very rare occurrence and when it exists, it becomes clinically important because of its rarity. We are reporting here the presence of a very small accessory liver lobe and have discussed its clinical relevance. We observed a mini liver lobe which was situated in the posterior part of the fissure for ligamentum teres. It was triangular in shape and about one inch in width. It was attached to the left anatomical lobe of the liver through a vascular pedicle which contained the branches of hepatic artery and portal vein and hepatic duct. Histological sectioning revealed the normal liver architecture in the accessory lobe. The knowledge of this accessory lobe could be of use to surgeons and radiologists.
Liver, Accessory lobe, Variation, Hepatic
Case Report
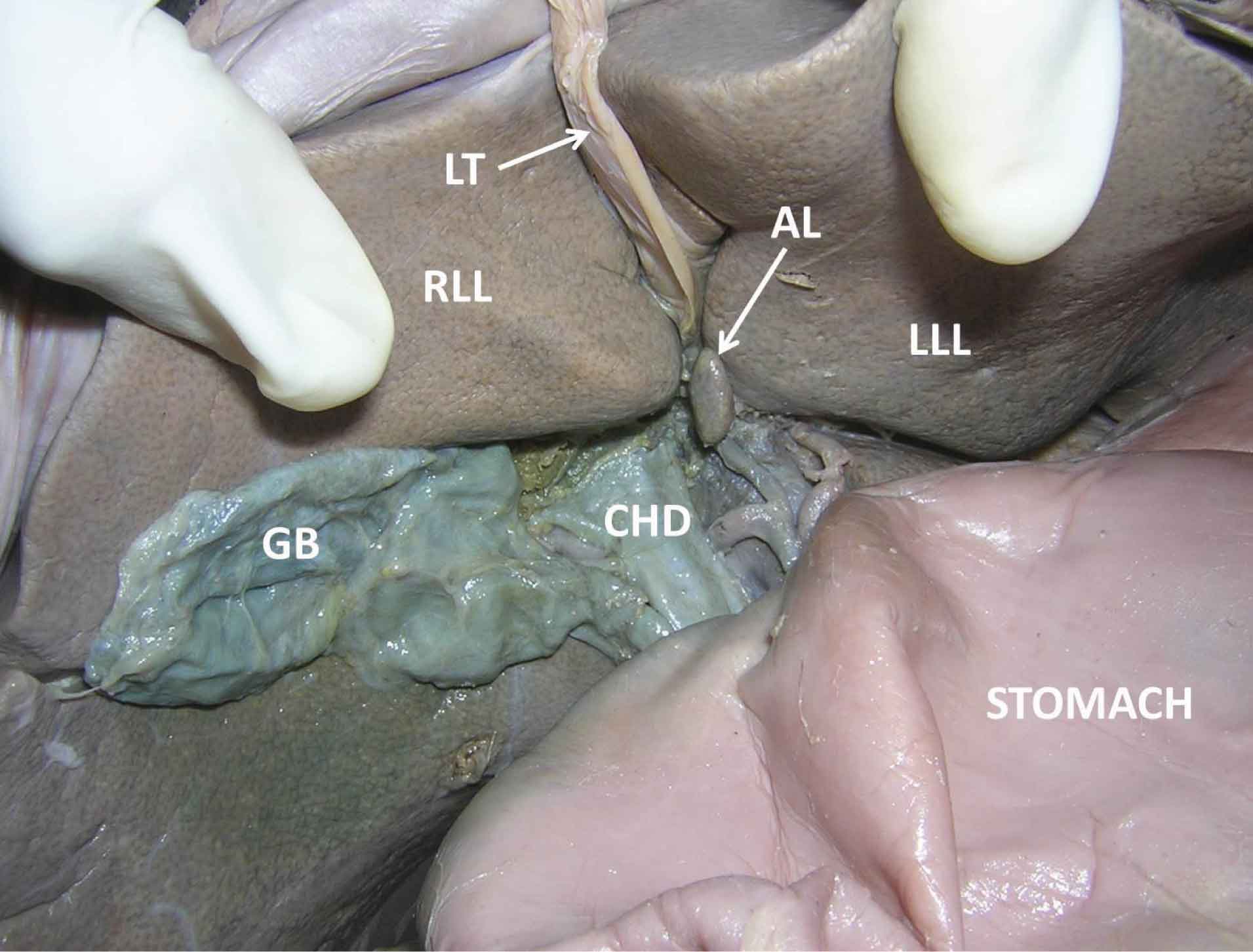
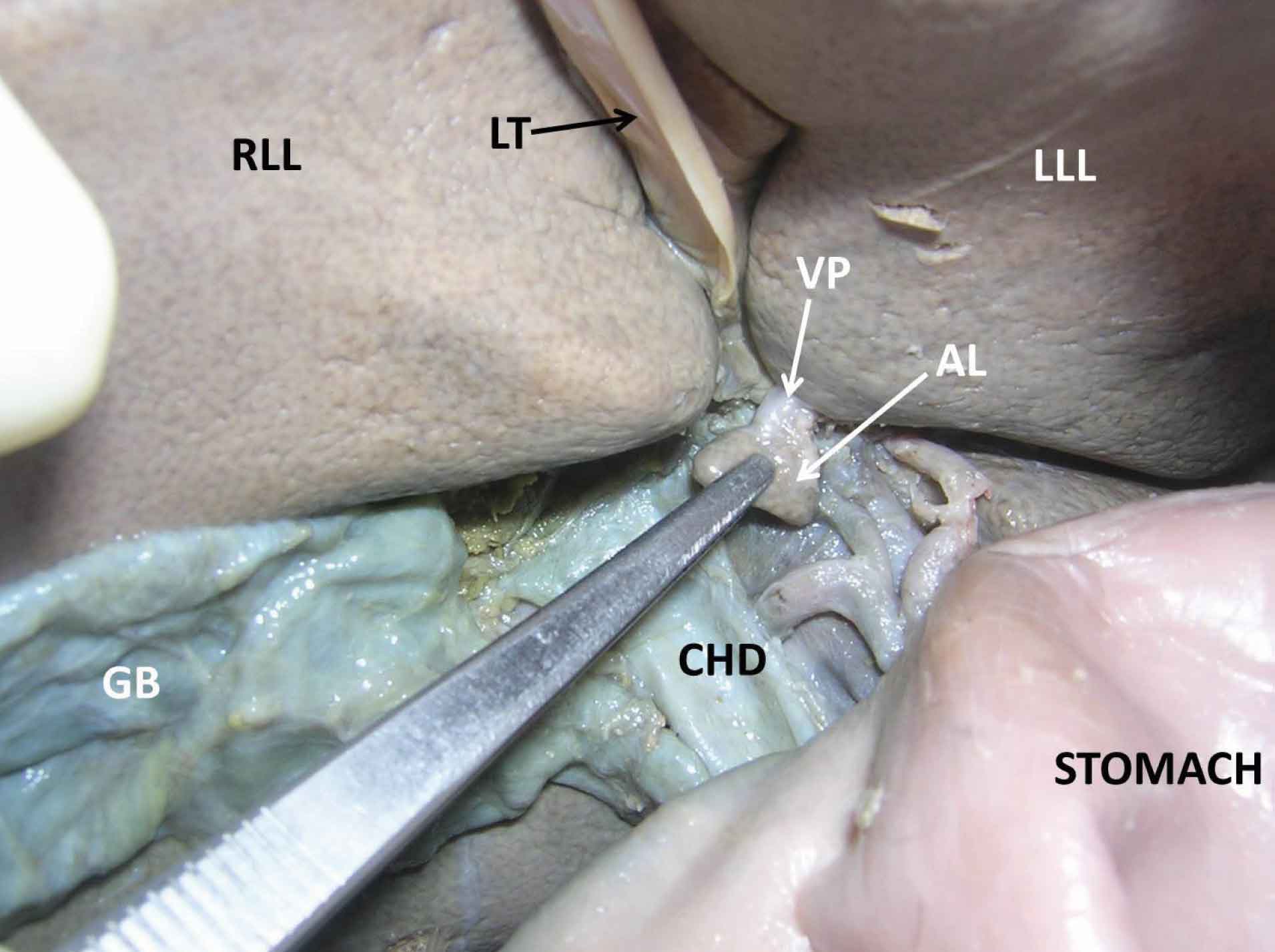
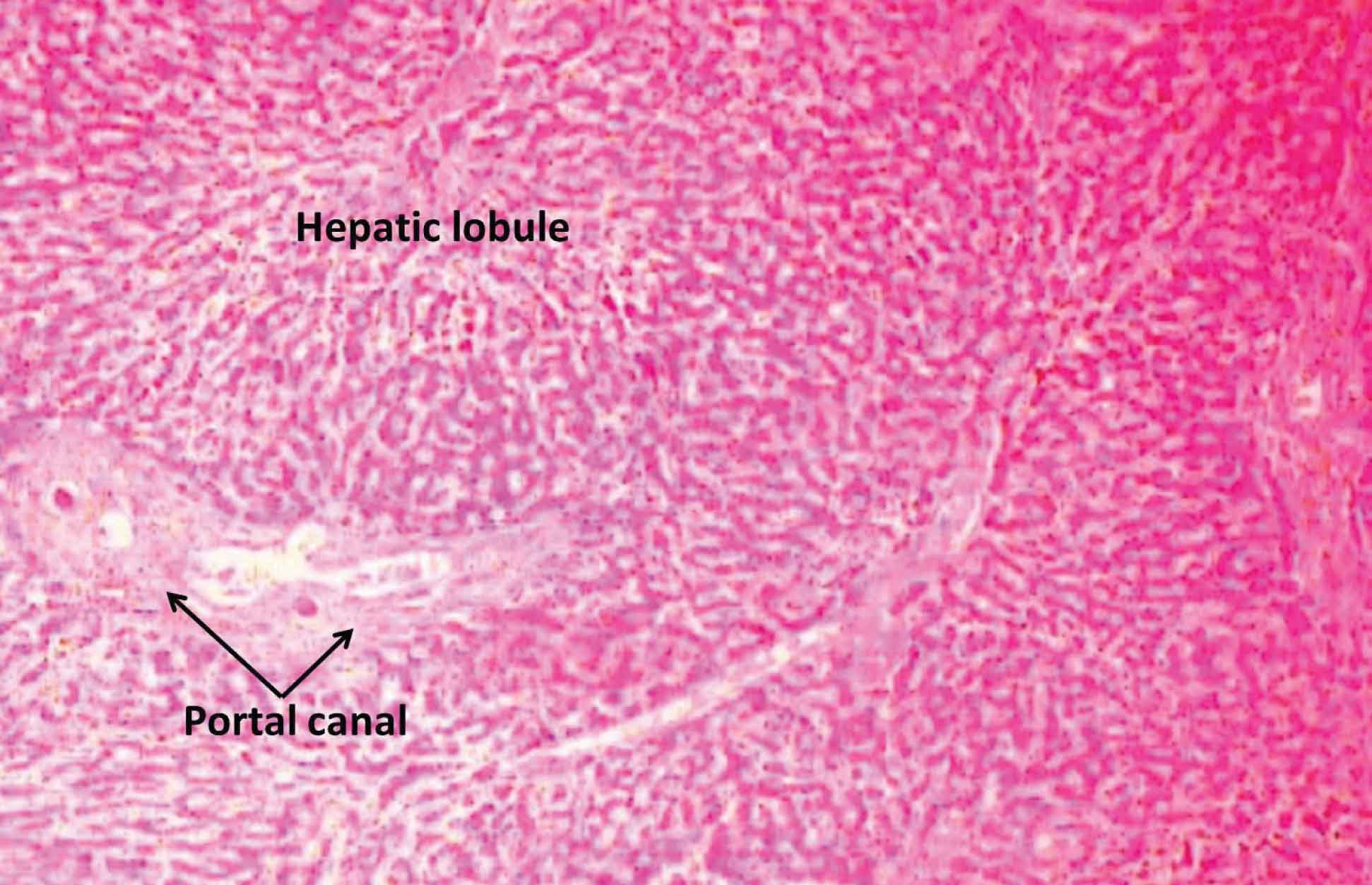
During dissection classes which were held for undergraduate medical students, we saw a small accessory lobe of the liver in an adult male cadaver which was aged approximately 70 years. It was situated in the posterior part of the fissure for ligamentum teres, close to the porta hepatis [Table/Fig-1]. The lobe was triangular in shape and about one inch in width. It was attached to the left anatomical lobe of the liver through a vascular pedicle which contained the branches of hepatic artery, portal vein and hepatic duct [Table/Fig-1 and 2]. Histological processing of the lobe revealed an apparently normal liver architecture in the accessory lobe [Table/Fig-3].
Dissection of upper abdominal region showing accessory liver lobe (AL)
(RLL – right lobe of the liver; LLL – left lobe of the liver, LT – ligamentum teres; GB – gall bladder; CHD – common hepatic duct)
Closer view of the accessory liver lobe (AL) of the liver
(RLL – right lobe of the liver; LLL – left lobe of the liver, LT – ligamentum teres; VP – vascular pedicle of the accessory lobe; GB – gall bladder; CHD – common hepatic duct)
Photomicograph of the accessory lobe of the liver (H&E staining, 10x10 magnification)
Discussion
The occurrence of accessory liver lobes is one of the rarest variations. Among the reported accessory lobes, Reidel’s lobe is the commonly occurring variation [1]. It is a downward growth from the right lobe of the liver towards the iliac fossa and it rarely produces any symptoms [2]. According to Caygill and Gatenby [3], there are four main types of abnormally positioned livers (1) a liver which is not connected to the main liver and, which is usually, attached to the gallbladder or the intra–abdominal ligaments; (2) a microscopic ectopic liver which is found in the gallbladder wall; (3) a large accessory liver lobe which is attached to the main liver by a stalk, and (4) a small accessory liver lobe (10–30 g in weight) which is attached to the main liver. The accessory lobe which was observed by us belonged to the 4th type, but it was much smaller than the earlier reported cases. The accessory lobes can also be classified into three types, based on the biliary drainage pattern. In type 1, the duct of the accessory lobe drains into an intra–hepatic bile duct of the normal liver; in type 2, the duct of the accessory lobe drains into an extra–hepatic bile duct of the normal liver, and in type 3, the accessory lobe and the normal liver have a common capsule and the bile duct of the accessory lobe drains into an extra–hepatic duct [4]. Our observation showed a type 1 liver, according to this classification.
The accessory lobe which is being reported here is surgically and radiologically very important due to its small size and the presence of a vascular pedicle. Due to the small size, it might be mistaken for a lymph node. It might be accidentally removed during the surgeries in and around the porta hepatis. A damage to the lobe or its vascular pedicle might result in bleeding into the abdominal cavity. Accessory lobes need attention when there is torsion of the vascular pedicle or metastasis occurring in them. Torsion of the accessory lobes is a surgical emergency and it has to be attended to early [5,6].
An accessory lobe could be formed by the displacement of the primitive rudiment of the organ, or by persistence of the mesodermal septa during its proliferation [7]. Its presence occurs due to an error in the formation of the endodermal caudal foregut and segmentation of the hepatic bud in the third month of the intrauterine life [5].
Conclusion
Awareness of the presence of a small accessory lobe of the liver near the porta hepatis is useful for surgeons and radiologists in diagnosing, surgical planning and avoiding iatrogenic injuries of the accessory lobe.
[1]. Massaro M, Valencia MP, Guzman M, Mejia J, Accessory hepatic lobe mimicking an intra-abdominal tumorJ Comput Assist Tomogr 2007 31:572-73. [Google Scholar]
[2]. Bingham JB, Maisey MN, Unusual scintigraphic appearance of a mobile accessory lobe of the liverJ Nucl Med 1978 19:1235-37. [Google Scholar]
[3]. Caygill CP, Gatenby PA, Ectopic liver and hepatocarcinogenesisEur J Gastroenterol Hepatol 2004 16:727-29. [Google Scholar]
[4]. Elmasalme F, Aljudaibi A, Matbouly S, Hejazi N, Zuberi MS, Torsion of an accessory lobe of the liver in an infantJ Pediatr Surg 1995 30:1348-50. [Google Scholar]
[5]. Carrabetta S, Piombo A, Podesta’ R, Auriati L, Torsion and infarction of accessory liver lobe in young manSurgery 2009 145:448-49. [Google Scholar]
[6]. Elmasalme F, Aljudaibi A, Matbouly S, Hejazi N, Zuberi MS, Torsion of an accessory lobe of the liver in an infantJ Pediatr Surg 1995 30:1348-50. [Google Scholar]
[7]. Pujari BD, Deodhare SG, Symptomatic accessory lobe of liver with a review of the literaturePostgrad Med J 1976 52:234-36. [Google Scholar]