Trauma to spine is one of the grave injuries. They cause infinite morbidity and disability to the patient. If not treated promptly and rationally, patient might be confined to bed for his life [1]. Thoraco-lumbar spine is the most commonly injured segment of the spine. Commonly it affects young adult males who are the major bread earners in the family. This causes infinite economic and emotional burden to family in particular and society in general.Historically thoraco-lumbar fractures have been treated with recumbency i.e. bed rest for 8 to 12 weeks [2,3]. This mode of treatment is accompanied by complications of recumbency. It is very labour intensive. Cost of therapy in terms of hospital hours used, bed occupancy and care by trained personnel is very high. In a country like ours, where there is acute shortage of hospital facilities and trained manpower, conservative management, more often than not, ends up as benign neglect. Lately consensus is evolving across the world for stabilization of unstable spines with fusion and instrumentation even though most authors agree that neurological recovery is independent of treatment modality [1]. In pedicular screw instrumentation, fixation is achieved is more rigid as the screw is passed through force nucleus of the vertebra. This is the point through which five anatomical structures – the superior facet, the inferior facet, the lamina, the pedicle and the transverse process; channel all the posterior forces transmitted to the body [4]. Objectives of this study were to evaluate the effectiveness of spinal stabilization with pedicular instrumentation in the management of thoraco-lumbar fractures to restore the structural stability, early ambulation and improving neurological status of the patient.
Material and Methods
During the period from October, 2009 to September, 2010 after getting Institution ethical committee clearance, a prospective study of management of unstable thoraco-lumbar spine fracture treated operatively with posterior decompression and pedicular screw instrumentation was carried out.Inclusion criteria included skeletally mature patients presenting with unstable thoracolumbar fractures to our institution. The instability was judged by the following criteria [1]:
Presence of neurological deficit or worsening of neurological status on conservative management.
Significant vertebral instability i.e. (i) Compression of vertebral body height of more than 50%. (ii) Kyphosis of more than 20%. (iii) Fracture dislocations and subluxations. (iv) Significant cord compression in MRI.
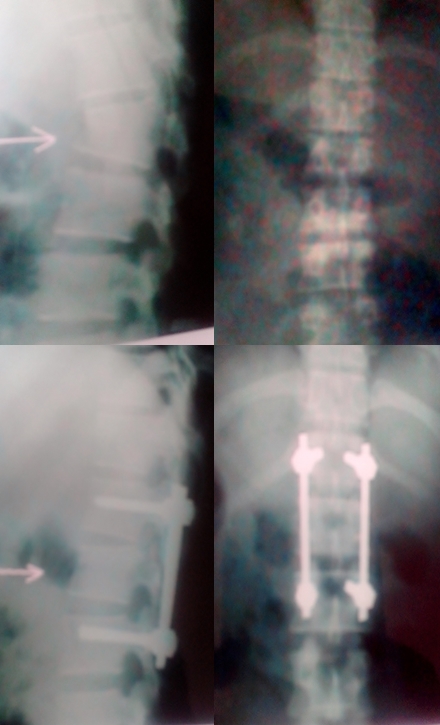
Exclusion criteria included skeletally immature patients, poly trauma patents and those associated with head injury. Thirty three patients were included, of these, 3 cases were lost to follow-up. Hence the results of 30 cases were evaluated. All patients were evaluated with detailed history and a thorough general physical and neurological examination to find out mode of injury, the level of injury and the extent of neurological damage. All patients had radiographs of thoraco-lumbar spine in both antero-postrior and lateral views [Table/Fig-1]. All fractures were classified according to Majerl (AO) classification [5]. The exact level of injury, type of fracture and mechanism of injury were ascertained. MRI was taken in 26 patients. Affordability was the main limiting factor. Pre-operative neurological assessment was done using ASIA scale [6] and individual patient’s neurology was graded Grade A (complete paraplegia) to Grade E (normal neurology). Radiologically deformity was assessed by calculating sagittal angle (SA) and sagittalindex (SI).
Preoperative and post-operative radiographs
Surgical procedure
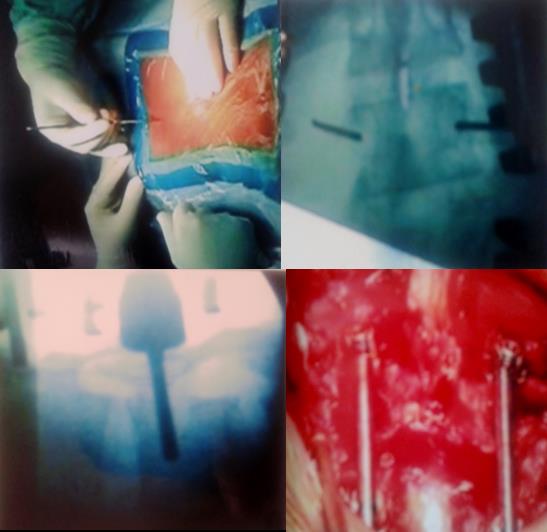
Prophylactic antibiotics were given preoperatively. After general anaesthesia, the patient was placed in prone position on a padded spinal frame on a radiolucent table. This position avoids venostasis and decreases intra-abdominal pressure, thus reducing the venous bleeding. A posterior midline incision was made centring over the injured vertebra and extending two levels above and below. The incision was deepened to expose the posterior elements of the vertebrae one level above and below the injured vertebra. The dissection was carried laterally to the tips of transverse processes, maintaining meticulous haemostasis. The pedicles were located by identifying the point of convergence of a horizontal line along the centre of transverse process and vertical line along the centre of superior facet. Using a rongeur, cortical bone was removed to expose the underlying cancellous bone. Blunt k-wires were placed into the pedicles and their position confirmed in both AP and lateral views using image intensifier. Pedicle was probed in all four quadrants to make sure that there is no violation of pedicular cortex. Now the pedicles were tapped. The vertebral body was not tapped to increase the screw purchase. The appropriate sized pedicular screws were inserted making sure it penetrates 50 to 70% of the body. Posterior laminectomy was done and any bony fragments inside the spinal canal were removed. Posterior elements were gently decorticated and prepared for fusion and cancellous graft harvested from iliac crest was generously spread over fusion bed. Rods were contoured and placed over the screws and provisionally held by tapered nuts. Using distractor, acceptable correction of deformity and vertebral height was achieved under image intensifier control and nuts were tightened to maintain reduction. Thorough haemostasis was achieved and wound closed in layers [Table/Fig-2]. The mean intra-operative time was 2:30 hours.
Intra-operative pictures of pedicular screw instrumentation
Five patients had significant additional injury. 1 patient had calcaneal fracture, which was treated conservatively, 3 patients had multiple rib fractures and were treated conservatively, 1 patient had talus fracture and was treated with open reduction and internal fixation with cancellous screws. Post-operatively patients were given intravenous antibiotics for 5 days and then switched over to oral antibiotics till suture removal. Intravenous corticosteroids were given for three days. Intensive physiotherapy was started from first post-operative day in the form of stretching and active, active assisted and passive range of movements. On the second day they were allowed to roll from side to side. They were made to sit up and mobilized on wheel chair after applying Knight-Taylor brace from the fourth post-operative day. Sutures were removed on twelfth day. Knight-Taylor brace was used up to 12 weeks and patients were gradually ambulated depending upon neurological recovery. Patients with good neurological recovery were gradually weaned off urinary catheter whereas those with complete paraplegia and without good recovery were taught clean intermittent self catheterisation. All patients were followed up in OPD at monthly interval. At each follow-up, results were evaluated for neurological recovery by ASIA score and radiological correction by sagittal angle and index [Table/Fig-1]. The complaints or complications were duly noted and treated.
Observation and Results
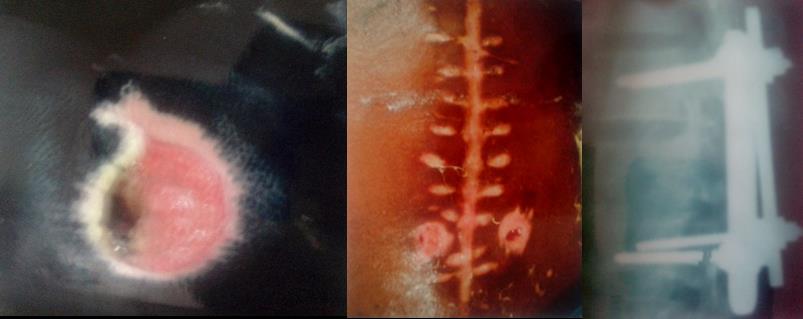
During the study period 33 patients were treated of which 3 were lost to follow-up. Hence the results of 30 patients were evaluated. The mean duration of follow-up was 11 months (range 6-12 months). Of the 30 patients 28 were male and 2 female. The age ranged from 18 to 52 years. The most common age group involved was 21 to 30 years. Fall from height was the commonest mode of injury (19), followed by road traffic accidents (9) and weight falling on the back (2). T12 was the commonest site of fracture (12), followed by L1, T11, T10, L2 and T9. All fractures were classified according to Magerl classification system. There were 17 type A, followed by type C (7) and type B (6) fractures. The earliest surgical intervention was at 16 hours after the trauma. The mean interval between injury and surgery was 4 days (range 16 hours to 10 days). Mean duration of follow-up was 11 months (range 6 months to 20 months). All patients were assessed for neurological status using ASIA scale. Nineteen patients presented with complete paraplegia (grade A) and 11 with incomplete paraplegia (Grade B,C,D and E). Of the 30 patients 24 showed neurological improvement by at least 1 grade and average grade of improvement was 1.5 grades. Mean preoperative sagittal angle (SA) was 19.9 degrees and sagittal index (SI) was 0.54. Mean post-operative SA was 9.3 degrees and SI was 0.72. Mean SA and SI during final follow-up were 10.9 degrees and 0.69 respectively. During post-operative period and follow-up following complications were noted: Urinary tract infection (5), bed sores (3), superficial wound infection (1) and deep wound infection (1), implant prominence (1) and implant failure (1). All patients with UTI were treated with repeated thorough bladder wash and appropriate antibiotics. All responded well to treatment. The reason for development of bed sore in three patients was the non-compliance of the patient and attenders to adhere to posture change regimen [Table/Fig-3a]. They were treated by antiseptic dressing, antibiotics and use of water bed and ring cushion below the sacral area. All bed sores healed over time without need for a secondary procedure. One patient with superficial wound infection responded to daily dressing and antibiotics according to culture and sensitivity report. One patient who had deep infection did not respond well to antibiotics [Table/Fig-3b]. A thorough surgical debridement and wash out was given. In spite of that infection persisted, so implants had to be removed at 4 months, following which infection subsided. One patient with T12 fracture had kyphosis of 26 degrees. As the patient had pain on lying supine because of implant prominence, they were removed at 5 months. Patient did not have neurological deterioration. One patient with T12 fracture presented with a broken pedicular screw during 6th month of follow-up [Table/Fig-3c]. Since patient was asymptomatic and showed no neurological deterioration, it was left alone.
Various complications seen during follow-up period
Discussion
Posterior trans-pedicular screw fixation initially was reported by Boucher in 1959 [7]. Since then, modern instrumentation systems have been developed. These systems control segmental motions in three dimensions, preserve motion segments, avoid long fusions, and provide a more stable construct [8]. Pedicle screws have a high pull-out and cut-out strength and can withstand high stresses without failure [9]. They can therefore achieve and maintainreduction of a short segment. Operative stabilization consists of segmental distraction with pedicle screw fixation one level above and one level below the injured segment. By applying distraction, ligamentotaxis is exploited to aid in reduction of retro-pulsed bone and disc fragments.
Advantages of posterior instrumentation include: Familiar approach to orthopaedic surgeons, does not compromise lung function, which may be already compromised after the injury, fracture reduction is easier and complication rates are low.
Disadvantages include: Decompression of canal is difficult and often incomplete and difficult to achieve anterior fusion. As with all surgical implants; trans-pedicular screw instrumentation maintains reduction until bony union is achieved. Short-segment posterior fixation (SSPF) is the most common and simple treatment, offering the advantage of incorporating fewer motion segments in the fusion [10–13].
Advantages of pedicular screw systems include: Very rigid fixation, high percentage of fusion, low percentage of hardware failure, short segment immobilisation and maintenance of curvature of spine.
Disadvantages include: Surgical technique has a very steep learning curve, exposure to radiation from image intensifier, chance of injury to nerve roots, cord and blood vessels.
During the surgical procedure, it is imperative that wide exposure is performed, till the tips of transverse process to achieve good postero-lateral fusion. It is important to insert pedicular screws before doing laminectomy, as it helps to decompress the cord by reducing retropulsion and reduce the chances of iatrogenic cord injury. It is also important to achieve posterolateral fusion to augment stabilization. Wang et al., [14] concluded that fusion significantly improves the clinical outcome and substantially reduces the incidence of recurrent kyphosis.
Of the 30 patients, 70% were between 20-40 years, i.e. young adults. One of the reasons for high incidence in young adults could be due to their predominant outdoor activities. This is the economically most active group and thus these fractures cause a great economic burden on their families and society. 93% of patients were males. In a similar study conducted by R Roy Camille et al., [8], mean age was 30 years and male to female ratio was 2:1. In KD Tripathi and AK Singh study [15], mean age was 29.3 years and male to female ratio was 4:1. Predominantly manual labour and climbing trees for fruit harvesting by males might be responsible for very high incidence in them. Fall from height accounted for 63% of the injuries followed by road traffic accidents (30%). R.Roy Camille study [8] found road traffic accident as the most common cause (46%) and in K.D. Tripathi and A.K. Singh study [15], fall from height was the commonest cause (60%).The high incidence of fractures following fall from height in our study could be due to coconut and areca nut cultivation in our parts of state. T12 & L1 accounted for 66% of cases. The thoraco-lumbar junction is very vulnerable to injury due to high mobility at this site. Also rib cage gives additional support to thoracic segments. Type A accounted for 56% of the fractures. These are vertebral body compression fractures. Amongst these Type A3 (burst fractures) predominated. Fall from height typically result in these fractures. Type B&C were commonly seen with road traffic accidents. These are high energy injuries and complete paraplegia is common in this group. T12-L1 level accounted for 66% of the cases in KD Tripathi and AK Singh study [15] and 42% of the cases in R Roy Camille et al., study [8] [Table/Fig-4].
Comparison of studies regarding patient variables, mode of injury and level of injury
| R. Roy Camille et al. | K.D. Tripathi & A.K. Singh | Our study |
|---|
| Mean age | 30 years | 29.3 years | 31.6 years |
| Male:Female | 2:1 | 4:1 | 9:1 |
| Commonest mode of injury | Road traffic accidents (46%) | Fall from height (60%) | Fall from height (63%) |
| T12-L1 injury | 42% | 66% | 66% |
Neurological improvement by at least 1 grade was seen in 24 (80%) of patients during follow-up. The average grade of improvement was 1.5 grades. In the study by Jerome M Cottler et al., [16], 31.9% of the patients showed neurological recovery and Keiichiro Shiba et al., [17] reported neurological improvement in 47% of the patients. Higher percentage of neurological recovery could be due to higher number of incomplete cord injuries in our series [Table/Fig-5]. Radiological correction achieved was fair to good and there was minimal loss of correction during follow-up. In our study, the mean loss of sagittal angle (SA), during the follow-up was 1.6 degrees. In R. Roy Camille study [8], the mean loss of correction was 3 degrees and in a study by Essess et al., [18], the mean loss of correction was 3.5 degrees [Table/Fig-6].
Comparison of studies regarding neurological course
| Neurological course | Jerome M Cottler et al., | Keichro Shiba et al., | Our study |
|---|
| Percentage of patients having neurological recovery by at least 1 grade | 31.9% | 47% | 80% |
Comparison of studies regarding radiological course
| Radiological course | R. Roy Camille et al., | Esses et al., | Our study |
|---|
| Mean loss of sagittal angle during follow-up | 3° | 3.5° | 1.6° |
The disadvantages of pedicular screw system are steep learning curve, high technical expertise and experience to minimize complications of faulty placement of pedicular screws and requirement of image intensifier. The results in our short series of 30 cases have been encouraging. But there is need for more cases and longer follow-ups to come to categorical conclusion.
Conclusion and Summary
As demonstrated by our study, patients with unstable thoraco-lumbar fractures are better treated by stabilization and decompression as it reduces complications of recumbency and helps in early mobilisation. Pedicular screw system is very versatile and technically superior as it achieves three column fixations and helps in efficient and sustainable distraction. The results in our short series of 30 cases have been encouraging. But there is need for more cases and longer follow-ups to come to categorical conclusion.