Case Report
A 20-years-old female patient presented for pre-operative evaluation for excision of left sided adrenal tumour. She complained of intermittent abdominal pain, excessive sweating, episodic headache since 2 years and palpitations since 6 months. The patient was diagnosed with hypertension two years back and was started on Tabs. Prazosin 15 mg twice daily, Clonidine 100 mg thrice daily, Furosemide 40 mg daily. The patient’s previous medical and surgical history was uneventful.
On examination, height was 165 cms and weight 53 kgs. The ASA physical status classification was ASA 3. Mallampatti classification-1. The heart rate was regular, 140 per minute. Her blood pressure in supine position was - 200/130 mm of Hg and standing- 190/120 mm of Hg. Pulse rate was 140 bpm, regular in nature. Rest of the examination was unremarkable [Table/Fig-1,2,3and4].
| Hb - 12 g% |
|---|
| ESR - 10 mm 1st hour |
| RBS - 88mg/dl |
| Blood Urea- 30mg/dl, Serum Creatinine- 0.6 mg/dl |
| Serum Electrolytes-Sodium-137 mmol/L, Potassium-4.6 mmol/L, Calcium- 9 mg/dl |
| ECG–Tachycardia, LVH with strain pattern. |
| Thyroid function tests-within normal limits |
| PT-15.4 S INR-1.16 |
| Renal Doppler- within normal limits |
|---|
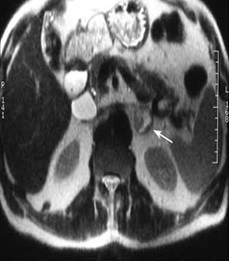
| CT whole body-head and neck-Normal, chest-Normal, abdomen: adrenal- heterogenous left adrenal mass 4.6x3.6x5.2mm, no evidence of extra adrenal Pheochromocytoma. |
| 2D Echo– left ventricular hypertrophy with mild TR with 58% ejection fraction. |
| Chest X Ray– normal lungs fields with cardiomegaly. |
| MIBG–revealed no extra adrenal involvement |
CT showing left-sided adrenal mass
| Urine VMA- 164.4 mmol/ 24 hrs. |
|---|
| Cortisol- 248.4 mmol/ L |
| Epinephrine- 98.9 μg/ 24hrs |
| Noradrenaline- 4794.84 μg/ 24hrs |
| Dopamine- 2536.98 μg/ 24hrs |
Ophthalmology, Endocrinology and Cardiology opinions were taken. Increase in drug dosage, addition of β-blocker and Calcium Channel blocker was advised.
By second visit, she was receiving tablets Clonidine 100 mg thrice daily, Prazosin 15 mg twice daily, Furosemide 40 mg once daily, Atenolol 50 mg twice daily, Nicardipine 20 mg twice daily and Alprazolam 0.5 mg once daily. Her B.P. was -150/110 mm of Hg in sitting and 150/100 mm of Hg in supine position with a pulse rate of 120 bpm.
Patient was started on Tab. Lorazepam 3 days before surgery for anxiolysis. I.V fluid therapy with 1.5 litres of crystalloid/day was started 3 days prior to ensure hydration. All drugs were continued till day of surgery. Preoperative B.P in supine position was 120/98 mm of Hg, standing 80/40 mm of Hg with a pulse rate of 88 bpm.
Patient was planned for combined General and epidural Anaesthesia.
Two 18 G I.V. line secured. Two Ringer Lactate started. ECG, SpO2, NIBP, CVP and EtCO2 monitors were arranged. Epidural catheter was secured at T10-T11 level, a test dose of lignocaine 3 cc tried and a bolus of 0.5% bupivacaine 6 cc administered.
Premedication was achieved with I.V. Glycopyrrolate 0.2 mg, Midazolam 2 mg, Fentanyl 100 μg, Ondansetron 4 mg and Hydrocortisone 100 mg. Induction of anaesthesia was started with 100 mg I.V. Lignocaine, Esmolol 5 mg, Inj Propofol 120 mg and tracheal intubation was facilitated by Vecuronium 4 mg I.V. At induction of anaesthesia BP was 110/80 mm of Hg and post intubation it was 100/70 mm of Hg.
CVP triple lumen 18G line was secured under asepsis. Blood pressure was monitored. Continuous ECG, PR, and EtCO2 monitoring was done. CVP and urine output were measured every half an hour. Patient was started on I.V. Vecuronium infusion of 3 mghr-1, epidural infusion of 0.125% bupivacaine with fentanyl 25 μg at 6ml/ hr and maintained throughout the duration of surgery. SNP infusion started at 0.5 μgkgmin-1 at incision and titrated according to B.P. with maximum dose at 1 μgkgmin-1. Propofol infusion started at 100mghr-1. Inj fentanyl 50 μg I.V. was repeated at 1.5 hr and 3 hrs. CVP was maintained around 10cms of H2O.
Intraoperatively, vitals remained stable. After ligation of main adrenal vein, patient’s B.P. and P.R. increased. Administered Esmolol bolus 5 mg which was repeated after 15 min, Esmolol infusion 50 μg/kgmin-1 was started and tapered accordingly. Multiple draining veins were ligated. B.P. reduced, Esmolol infusion and SNP infusion were stopped.
Patient received 10 crystalloids and 2 colloids over 4 hrs and sustained a blood loss of 400 ml. Urine output was 2500 ml over 4 hrs. Post-operatively patient was not on any vasodilators/ vasopressors. Patient was reversed with inj. Glycopyrrolate 0.4 mg and Neostigmine 2.5 mg after adequate respiratory efforts. Patient was not extubated, as she was drowsy and was shifted to ICU with ‘T’ piece, O2 support and was continuously monitored. Post-operative vitals- B.P.-120/90 mm of Hg, P.R.-88 bpm, SpO2 on room air was 100% [Table/Fig-5].
Intraoperative specimen of tumour

The same evening, patient was extubated as she was conscious and was monitored in ICU for 2 post operative days. On second post-operative day patient had increase in B.P. -150/100 mm Hg, Tab clonidine 100 mg once daily was resumed and was planned to withdraw gradually. Patient was receiving epidural analgesia postoperatively. Glucose level monitoring was done every second hour. Patient was shifted out of ICU on 3rd post-operative day.
Follow up on 3rd week revealed reduction in urine catecholamine levels. Patient was tapered off from Clonidine. Histopathology confirmed ““Pheochromocytoma””.
Discussion
The World Health Organization defines pheochromocytoma as a tumour from catecholamine-producing chromaffin cells in adrenal medulla—an intra-adrenal paraganglioma [1,2]. Usually, found in adrenal medulla but they may arise anywhere in the body [1].
Patient’s symptoms reflect excessive secretion of catecholamines into circulation [3]. Clinical presentation varies from triad of episodic headache, diaphoresis and palpitations to a variety of non-specific symptomatology. Most frequent symptom of Pheochromocytoma is hypertension.
Prolonged exposure of the circulation to high norepinephrine concentration results in constriction, of both arteriolar and venous circulation, with a decrease in circulating volume [4,5].
The best confirmatory test is to measure free catecholamines and their metabolites in a 24 hrs urine collection [6,4].
MRI and CT both provide accurate and consistent identification of Pheochromocytomas [7]. Tumours in unusual sites and metastases may have to be identified with metaiodobenzguinidine (MIBG) scintigraphy [5].
A clinical evaluation of the cardiac status of the patient is to be done. A baseline and serial monitoring of full blood count and haematocrit provides an assessment of the adequacy of volume expansion when α-blockade has been started [8].
Preopertive investigations
Blood glucose level measurement is needed as hyperglycaemia is common.
ECG: ST and T changes secondary to myocardial ischemia, ventricular hypertrophy, arrhythmias.
Chest X-ray may reveal cardiomegaly or pulmonary oedema [4].
2D ECHO: to estimate myocardial function if cardiomyopathy is suspected.
Renal function can be assessed using Urea, Creatinine and electrolytes.
Prior to surgery, it is necessary to control arterial pressure, heart rate and arrhythmias and to restore the blood volume to normal [9, 8]. This is conventionally done with α-blockade over a period of 10-14 days and subsequently, additional β-blockade is required to treat any tachyarrhythmias [4].
Prazosin (2-5 mg twice or thrice a day), selective α1-blocker, is favoured because of its shorter half life and ease of titration to the desired end point.
β-blockade is not instituted until α-blockade is established. A non selective β blocker should not be instituted before α blockade is achieved as blockade of β 2 vasodilatory receptors leads to unopposed stimulation and worsening of hypertension. β-blockers with additional α-blocking properties are synergistic with α-blockers in reducing B.P. eg. labetalol (100-400mg/day) and carvedilol (12.5-50mg/day).
Calcium channel antagonists can be used for preoperative control of B.P. and reduce preoperative and intraoperative coronary spasm. Preoperative sedation and anxiolysis and assurance will decrease anxiety and prevent marked haemodynamic fluctuation in immediate preoperative period [4] [Table/Fig-6] [10].
| To assess adequacy of preoperative management of Pheochromocytoma, following Roizen criteria should be met: |
|---|
| No in-hospital B.P. >160/90 mm Hg for 24 hours prior to surgery. |
| No orthostatic hypotension with B.P. <80/45 mm Hg. |
| No ST or T wave changes for 1 week prior to surgery. |
| Not more than 5 premature ventricular contractions per minute11. |
Communication between operating and anaesthesia teams is crucial for success of intraoperative management of patients undergoing resection.
Routine monitoring along with CVP monitoring. Pulmonary artery catheter is not an absolute requirement and should be reserved for severe left ventricular dysfunction and cardiovascular compromise [11].
G.A. with thoracic epidural anaesthesia was chosen for our patient as thoracic epidural blocks, sensory and sympathetic discharge in area of surgical field and hence, provides better haemodynamic stability.
Midazolam can be used to facilitate co-induction [6]. Anaesthesia can be induced with fentanyl 2-5 μkg-1 and Propofol 1-2 mgkg-1.
Intubation should be attempted with satisfactory depth of anaesthesia. Vecuronium, Rocuronium and Cisatracurium have shown cardiovascular stability and release the least histamine. Atracurium and mivacurium release histamine.
To achieve intraoperative and postoperative analgesia by epidural route, infusion of bupivacaine 0.1-0.125% with fentanyl 2 mcgml-1 at the rate of 6-12 mlhr-1, is administered after an initial bolus of 8-10 ml of 0.25% bupivacaine in divided doses [4,5].
Sodium Nitroprusside (SNP), Phentolamine (boluses of 1-5 mg), Prazosin, Nitroglycerine (NTG) and various other agents like Magnesium Sulphate (loading dose of 40-60 mgkg-1 followed by 1-2 ghr-1), Nicardipine, Diltiazem, Esmolol are used to control rises in B.P. [4,12,5,8,13,14].
Lidocaine is useful for ventricular arrhythmias while Amiodarone is an alternative.
Volume loading before tumour ligation and fluid boluses should be tried before choosing adrenaline, noradrenaline and phenylephrine for Catecholamine withdrawal following venous ligation.
Patient is usually kept in ICU unit for first 24 hrs and monitored for haemodynamic instability [15,5,16,17]. Epidural analgesia provides good post-operative pain relief and may be supplemented by oral medications.
Approximately 50% patients remain hypertensive for few days, likely related to elevated catecholamine levels which persist for one week after resection [11].
Conclusion
Pheochromocytoma is rare and can present with multitude of symptoms mimicking other diseases. Good preoperative preparation and the judicial use of a combination of vasodilatory and vasopressor medications help in reducing mortality and morbidity associated with surgery. Good communication between surgeon, endocrinologist and anaesthesiologist is crucial for the safe management of these patients.
[1]. Pacak K, Eisenhofer G, Ahlman H, Bornstein SR, Gimenez-Roqueplo AP, Grossman AB, Kimura N, Mannelli M, McNicol AM, Tischler AS, Pheochromocytoma: recommendations for clinical practice from the First International SymposiumNat Clin Pract Endocrinol Metab 2007 3:92-102. [Google Scholar]
[2]. Karel Pacak APPROACH TO THE PATIENT Preoperative Management of the Pheochromocytoma Patient.The Journal of Clinical Endocrinology & Metabolism 92(11):4069–4079 Printed in U.S.A. Copyright © 2007 by The Endocrine Society doi: 10.1210/jc.2007-1720 [Google Scholar]
[3]. Prys-Roberts C, Pheochromocytoma - recent progress in its managementBr J Anaesth 2000 85:44-57. [Google Scholar]
[4]. Kinney MA, Narr BJ, Warner MA, Perioperative Management of PheochromocytomaJ Cardiothorasic Vasc Anesth 2002 16:359-69. [Google Scholar]
[5]. Singh G, Kam P, An overview of anaesthetic issues in PheochromocytomaAnn Acad Med Singapore 1998 27:843-8. [Google Scholar]
[6]. Hull CJ, Pheochromocytoma: diagnosis, preoperative preparation, and anaesthetic managementBr J Anaesth 1986 58:1453-68. [Google Scholar]
[7]. Perel Y, Sclumberger M, Marguerite G, Alos N, Revillon Y, Sommelet D, Pheochromocytoma and paraganglionoma in children: a report of 24 cases of the French Society of Pediatric OncologyPediatr Hematol Oncol 1997 14:413-22. [Google Scholar]
[8]. Jalil ND, Pattou PN, Combemale F, Chafuis Y, Henry JF, Peix JL, Effectiveness and limits of preoperative imaging studies for localization of pheochromocytomas and paragangliomas: a review of 282 casesEur J Surg 1998 164:23-8. [Google Scholar]
[9]. Vuguin P, Perez N, Monsalve MM. Pheochromocytoma. Web article from eMedicine Specialties>Pediatrics>Oncology. Last updated: June 5, 2006 [Google Scholar]
[10]. Roizen MF, Horrigan RW, Koike M, Eger EI 2nd, Mulroy MF, Frazer B, Simmons A, Hunt TK, Thomas C, Tyrell B, A prospective randomized trial of four anesthetic techniques for resection of pheochromocytomaAnesthesiology 1982 57:A43 [Google Scholar]
[11]. Desmonts JM, Marty J, Anaesthetic management of patients with pheochromocytomaBr J Anaesth 1984 56:781-9. [Google Scholar]
[12]. Chung PC, Ng YT, Hsieh JR, Yang MW, Li AH, Labetalol pretreatment reduces blood pressure instability during surgical resection of pheochromocytomaJ Formos Med Assoc 2006 105:189-93. [Google Scholar]
[13]. Schif RL, Welsh GA, Perioperative evaluation and management of the patient with endocrine dysfunctionMed Clin N Am 2003 87:175-92. [Google Scholar]
[14]. Tauzin-Fin P, Sesay M, Gosse P, Ballanger P, Effects of perioeprative alphal block on haemodynamic control during laparoscopic surgery for PheochromocytomaBr. J. Anaesth 2004 92:512-7. [Google Scholar]
[15]. Schif RL, Welsh GA, Perioperative evaluation and management of the patient with endocrine dysfunctionMed Clin N Am 2003 87:175-92. [Google Scholar]
[16]. Tauzin-Fin P, Sesay M, Gosse P, Ballanger P, Effects of perioeprative alpha l block on haemodynamic control during laparoscopic surgery for PheochromocytomaBr J Anaesth 2004 92:512-7. [Google Scholar]
[17]. Dugas G, Fuller J, Singh S, Watson J, Pheochromocytoma and pregnancy: a case report and review of anesthetic managementCanadian Journal of Anesthesia 2004 51:134-8. [Google Scholar]