Soft tissue tumours comprise a large heterogeneous group of mesenchymal neoplasms that is classified according to their normal tissue counterpart [1]. Benign tumours are at least 100 times more common compared to their malignant counterparts. The annual incidence of benign soft tissue tumours has been estimated to be about 3000/million population whereas that of soft tissue sarcoma is about 30/million that is less than 1% of all malignant tumours. Currently, there are no data to demonstrate a change in the incidence of sarcoma based on geographic areas [2].
Although most of these tumours are classified as either benign or malignant, many are of an intermediate nature displaying a locally aggressive behaviour with a low-to-moderate tendency to metastasize [3]. Hence these are divided into four categories: benign, intermediate (locally aggressive), intermediate (rarely metastasising) and malignant [4].
Benign tumours are usually superficial, well-defined, encapsulated masses demonstrating a slow growth [4]. However, any soft tissue tumour with any of the following four clinical features are invariably malignant requiring confirmation of diagnosis [5]: (i) increasing in size, (ii) size >5 cm, (iii) deep to the deep fascia, and (iv) painful.
Biopsy is a quintessential component of the preoperative investigations and should be done in every case, especially when malignancy is suspected. This would help in deciding the management approach: whether surgical excision is adequate, or a multimodal therapeutic approach is warranted [6].
Soft-tissue tumours are ubiquitous and can pose a challenge in terms of diagnosis and therefore, management. Soft tissue tumours, especially those that are present in a peripheral location and obvious to the patients entail lot of visits to the outpatient department. Though the morbidity caused due to the benign tumours is not significant, the financial implications due to the outpatient visits, investigations and the surgeries are not quantified.
Additionally, although soft tissue tumours are frequently encountered in clinical practice, they are hardly reported, especially in India and therefore there is a paucity of published literature from our sub-continent. Therefore, we conducted a study to understand various modes of clinical presentation, diagnostic modalities and to correlate them with operative findings, to delineate the various modes of management for patients with soft tissue tumours and also to assess the risk factors and complications associated with soft tissue tumours.
Material and Methods
This was a prospective study conducted from January 1, 2011 to May 30, 2013 at the Department of General Surgery. Approval was obtained from the Institutional Ethics Committee and all patients gave an informed consent to be included in this study.
Patients with peripheral soft tissue tumours like those of the upper and lower extremities, trunk, head and neck were included in the study. Those with visceral and retroperitoneal soft tissue tumours were excluded from the study.
Accurate history was elicited from all patients including operative risk factors, previous surgeries for soft tissue tumours and a thorough physical examination was done. The patient demographics were noted. Clinical parameters which were assessed included location and size of swelling, any associated pain, neurovascular symptoms (tingling, numbness, paraesthesia, weakness, pallor and ischemic changes in and around the region of the tumour), presence of any deformity (cosmetic disfigurement or restriction of movement in the nearest joint) and medical risk factors such as diabetes, hypertension and ischemic heart disease.
Biochemical investigations included fasting and postprandial blood sugar, blood urea and serum creatinine. Haematological investigations included haemoglobin percentage, total and differential counts, bleeding time and clotting time.
To diagnose the type of swelling, biopsy was done. The various biopsy techniques employed were fine needle aspiration cytology (FNAC), trucut biopsy, excision biopsy and incisional biopsy. The indications of biopsy were: (i) soft tissue mass in a patient with no history of trauma or that persisted for more than six weeks after local trauma, (ii) all soft tissue masses more than five centimetres in diameter and (iii) new, enlarging or symptomatic lesions.
The swelling was removed surgically in all patients. In case of malignancy, additional therapeutic modalities like radiotherapy and chemotherapy were employed.
Post-operative complications and hospital stay were recorded. Wound infection was defined as the absence of primary healing, with or without positive bacterial cultures, requiring antibiotics, with or without drainage. Septicaemia was defined as a rise of temperature above 40oC, with or without positive blood cultures All the results are described as percentages, mean and range.
Results
A total of 74 patients were enrolled in the study. Of them, 37 were males and 37 were females. The mean age at presentation in females and males were 32.89 years (Range: 11–64 years; Standard deviation [SD] 12.51) and 43.02 years (Range: 13-85 years; SD 6.80) respectively. Overall, the mean age was 37.96 years.
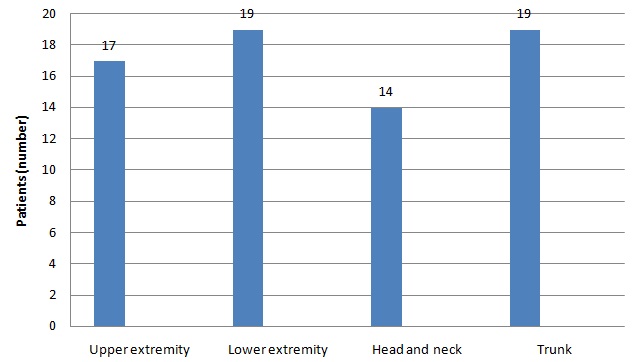
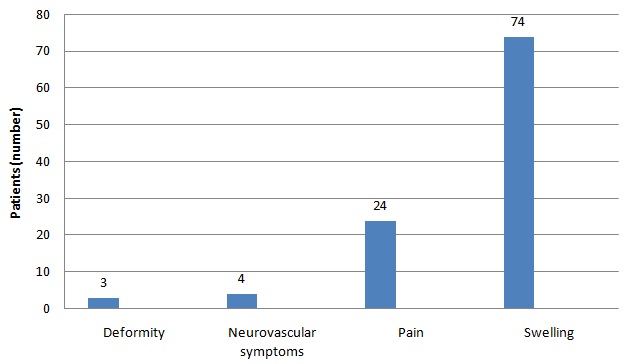
All the 74 patients were presented with a swelling. The distribution of the tumour based on the site is shown in [Table/Fig-1]. The lower extremities (25.60%) and trunk (25.67%) were the commonest sites. The size of the tumour ranged from 2 to 10 centimetres in diameter. A total of 24 (33.3%) patients complained of pain at the site of the tumour and 3 (4%) patients had deformities because of the swelling. Neurovascular symptoms were present in 4 (5%) patients [Table/Fig-2]. None of the patients had undergone any surgery previously for soft tissue tumours. Additionally, 3 (4.05%) patients each had diabetes and hypertension.
Distribution of soft tissue tumours
Of the 74 patients, 61 (82.4%) underwent FNAC, 6 (8.1%) trucut biopsy, 5 (6.7%) excisional biopsy and 2 (2.7%) incisional biopsy.
Seventy one patients had a benign tumour while in three patients, it was malignant. Based on the histopathological examination, the type of tumour was detected. Lipoma was the most common tumour present in 48 (64.86%) patients, followed by neurofibroma (n=14; 18.91%). Desmoid tumours and haemangiomas were present in 4 patients each. The occurrence of the different types of tumours is shown in [Table/Fig-3].
Type of soft tissue tumours
| Type of tumour | Number of patients (%) |
|---|
| Lipoma | 48 (64.86%) |
| Neurofibroma | 14 (18.91%) |
| Desmoid | 4 (5.4%) |
| Haemangioma | 4 (5.4%) |
| Haemangiopericytoma | 1 (1.35%) |
| Dermatofibrosarcoma | 1 (1.35%) |
| Schwannoma | 1 (1.35%) |
| Haemangioendothelioma | 1 (1.35%) |
With respect to management, for benign tumours, simple excision was done. For the malignant tumours, a multimodal therapeutic approach was adopted. For dermatofibrosarcoma protuberans, wide excision with primary skin grafting was done. For malignant Schwannoma, the tumour was excised, and then the patient was referred for radiotherapy. For haemangioendothelioma, the tumour was excised, and then the patient underwent chemotherapy with carboplatin and etoposide.
The mean hospital stay period was 7.2 days, ranging from 8 to 15 days. Two patients had skin ulceration over the tumour, preoperatively. Six patients developed wound infection postoperatively, and were treated with appropriate antibiotics.
Discussion
In our study, all patients presented with a swelling, which was associated with pain in about one-third of them. There was an equal distribution among both men and women and the average age of presentation was 37.96 years.
Benign tumours outnumber their malignant counterparts by a ratio of about 100:1.2 In our study of 74 patients, 71 of tumours were benign and 3 were malignant (benign: malignant=23.6:1). Lipoma was the most frequently encountered swelling.
The age and sex distribution of soft tissue tumours has not been well documented. They can occur at any age and in both sexes. The age-sex distribution depends on the type of tumour. For example, the distribution of malignancies which are familial is more in childhood, as stated by William and Strong [8] Similarly, in a study of soft tissue sarcomas of the extremities conducted by Geer et al., [9], the age of patients ranged from 16 to 88 years and male to female ratio was 1.3:1. The incidence of soft tissue tumours has been shown to be slightly higher in males than in females [3]. In our study, the age of patients ranged from 11 to 64 years with a mean age of 37.96 years. The male to female ratio was 1:1.
Both benign and malignant soft tissue tumours were present as a painless mass. In a study conducted by Lawrence et al., [10] in over 5800 patients, the most common presenting symptom was a swelling, followed by pain due to swelling. In our study, swelling was present in all the 74 patients. Pain was present in 24 patients (32.4%). Three patients had neurovascular symptoms. There are no reliable symptoms or signs to distinguish whether a tumour is benign or malignant. Most soft tissue sarcomas of the extremities and trunk wall were present as painless tumours, and were accidentally observed and do not caused any functional problems. Therefore, these tumours are frequently misinterpreted as benign [2]. Therefore, other diagnostic tests are to be relied upon to find out the type of tumour.
FNAC is the best investigation for assessing benign soft tissue tumours [3,11–13]. There are several histopathological types of tumours, but most of them are rare and can be diagnosed only on histopathological examination [3]. According to Rydholm,[14] open biopsy is not indicated because it increases both the magnitude of subsequent surgery as well as the need for adjuvant radiation therapy. Using FNAC, the surgeon directly proceeds to open operation. In our study, 61 patients (82.4%) underwent FNAC, 6 patients (8.1%) trucut biopsy, 5 patients (6.7%) excisional biopsy and 2 (2.7%) underwent incisional biopsy.
In our study, lipoma was the most frequently encountered tumor. Lipomas are the most common subcutaneous soft-tissue tumours, with an estimated annual incidence of one per 1,000 persons [15]. About one-third of the benign tumours are lipomas and another third fibrohistiocytic and fibrous tumours. The remaining tumours comprise of vascular tumours (10%) and nerve sheath tumours (5%). Lipomas are usually painless, unless when they compress a nerve [2,16]. About 80 percent of them are less than 5 cm in diameter [16]; however, some can be even more than 20 cm [17]. They are usually solitary in about 80% of cases, but sometimes, may be multiple, especially among young men [4,15].
Management of soft tissue tumours depends on whether the tumours are benign or malignant. Benign soft-tissue tumours required only complete local excision for adequate treatment. For a clinically localised primary or recurrent soft tissue sarcoma, surgery is the mainstay of therapy. Some non-metastasizing lesions, like desmoid-type fibromatosis or intramuscular haemangioma require wide excision similar to a sarcoma, otherwise local recurrence is very frequent [2]. Enneking et al., classified surgical procedures for sarcomas according to the margins achieved. They described four types of excisions: intralesional, marginal, wide and radical excisions [18]. Wide excision is the procedure of choice for lower-grade sarcomas whereas for higher grade sarcomas, multimodal therapy is preferred, including surgery, radiotherapy and/or chemotherapy.
In conclusion, soft tissue tumours were frequently encountered in surgical practice, and were mostly benign and required simple excision. However, since sarcomas were present frequently in a way indistinguishable from benign tumours, histopathological examination of all tumours should be mandatory. The chief limitation of our study is that the sample size is small, and therefore, it would be prudent to conduct a larger study.