Cardiovascular Disease (CVD) & related mortality has emerged as a major health burden worldwide with atherosclerosis being the major cause. The incidence of coronary artery disease has doubled in Indians during the past three to four decades. It will soon emerge as the single largest non communicable disease accounting for nearly one-third of all deaths in India.
Current prevalence of CVD to be between 7-13 % in urban and 2-7% in rural India [1]. An estimated 1.3 million Indians died from this in year 2000. The projected death from coronary artery disease by 2015 is 2.95 million of which 14% will be <30 years, 31% will be <40years [2]. WHO has predicted that from years 2000 to 2020 Disability Adjusted Life Years Lost (DALYs) from CVD in India shall double in both men and women from the current 7.7 and 5.5 million respectively [3].
In India, there is a wide variation of race, geographic factor, dietary habits, life style, tobacco & alcohol usage among population. So, epidemiological study of specific population is of great importance [4]. Indian population affected atherosclerosis with more advanced lesion at younger age than in other ethnic group [5].
As study of atherosclerosis in the living population is difficult, invasive & expensive especially in developing countries like India [6]. With the limited amount of resources available in rural and semi-urban population in India for studying atherosclerosis, an autopsy study gives a good measure of the prevalence, grading and distribution pattern of atherosclerotic lesions. Identifying the prevalence of sub-clinical atherosclerosis in a population helps the health administrators to plan preventive measures & strategy to prevent death in young age [7].
Material and Methods
This study was conducted on 264 hearts obtained from autopsies conducted by the Department of Forensic Medicine in M.P.Shah Government Medical College & GG Government Hospital, Jamnagar, a district, located in the western part of Gujarat, a state in India, from January 2012 to January 2013. Jamnagar, a district, located in the western part of Gujarat, a state in India. Completely autolyzed heart was excluded from our study. Each autopsy subject was identified, examined, and post mortem examination was done after obtaining consent from next of kin in case of medical autopsy and requisition from the Police/Department of Forensic Medicine in medico legal autopsies & after that cause of death was made.
The hearts was weighed & fixed in 10% buffered formalin solution. The heart was examined grossly & measurements of right ventricular wall, left ventricular wall, inter-ventricular septa & stump of aorta were taken. Circumference of mitral, tricuspid, pulmonary & aortic valve was noted. Coronary arteries were dissected along the flow of blood. Left Anterior Descending artery (LAD), Left Circumflex Artery (LCA), and Right Coronary Artery (RCA) were dissected longitudinally & each sectioned at 3 mm intervals to examine for any atherosclerotic plaques.
The coronaries were examined grossly for the presence of thrombus, narrowing of lumen, plaque of atherosclerosis & calcification. Tissue bits were taken from LAD, LCA, and RCA from gross atherosclerotic lesions as well as suspicious lesions for the microscopic assessment of atherosclerosis. If no lesions were found, random tissue bits were taken from above mentioned three sites. Tissue bits from calcified plaque were kept for decalcification.
After routine tissue processing & Paraffin embedding, section of 4-5 micrometer was cut by rotary microtome. Hematoxylin and eosin-staining of all the sections were done. Special stain like Trichrome stain was used when necessary to identify fibrous component in atheromatous plaque. Microscopic grading of atherosclerosis was done using the Modified American Heart Association (AHA) Classification of atherosclerosis [Table/Fig-1].
Modified American Heart Association (AHA) classification of atherosclerosis based on morphological description
| Description | Thrombosis |
|---|
| Non–atherosclerotic lesions |
| Intimal thickening | The normal accumulation of Smooth Muscle Cells (SMCs) in the intima in the absence of lipid or macrophage foam cells | Absent |
| Intimal xanthoma, or “fatty streak” | Luminal accumulation of foam cells without a necrotic core or fibrous cap. Based on animal and human data, such lesions usually regress. | Absent |
| Progressive atherosclerotic lesions |
| Pathological intimal thickening | SMCs in a proteoglycan-rich matrix with areas of extracellular lipid accumulation without necrosis | Absent |
| Erosion | Luminal thrombosis; plaque same as above | Thrombus mostly mural and infrequently occlusive |
| Fibrous cap atheroma | Well-formed necrotic core with an overlying fibrous cap | Absent |
| Erosion | Luminal thrombosis; plaque same as above; no communication of thrombus with necrotic core | Thrombus mostly mural and infrequently occlusive |
| Thin fibrous cap atheroma | A thin fibrous cap infiltrated by macrophages and lymphocytes with rare SMCs and an underlying necrotic core | Absent; may contain intraplaque hemorrhage/fibrin |
| Plaque rupture | Fibroatheroma with cap disruption; luminal thrombus communicates with the underlying necrotic core | Thrombus usually occlusive |
| Calcified nodule | Eruptive nodular calcification with underlying fibrocalcific plaque | Thrombus usually nonocclusive |
| Fibrocalcific plaque | Collagen-rich plaque with significant stenosis usually contains large areas of calcification with few inflammatory cells; a necrotic core may be present. | Absent |
According to Modified AHA classification importance of Pathological Intimal thickening lesion (Intermediate lesion), they are precursor lesion for future atherosclerotic lesion. Whether thrombus formation is associated with lesion or not is a new addition in this classification [8]. This classification has more clinical implication & descriptive terminology.
Results
The degree of atherosclerosis in Left Anterior Descending artery (LAD) was significantly more in compared with Left Circumflex Artery (LCA) & Right Coronary Artery (RCA). Intimal xanthoma, Pathological intimal thickening, fibrous cap atheroma & thin fibrous cap atheroma were common lesion in all three coronary artery. Intimal xanthoma was the highest in number amongst all lesion.[Table/Fig-2]. LAD showed highest, 58 cases of Pathological intimal thickening compared to LCA & RCA [Table/Fig-3]. Nine cases shows calcified nodule in LAD indicate more stabilization of plaque, less chance of plaque rupture & subsequent thrombotic occlusion. Maximum Number of thin fibrous cap atheroma (37 cases) was seen in LCA compared to RCA & LAD. Thin fibrous cap atheroma associated with high degree inflammation, erosion, thrombus indicates plaque vulnerability for rupture [Table/Fig-4].
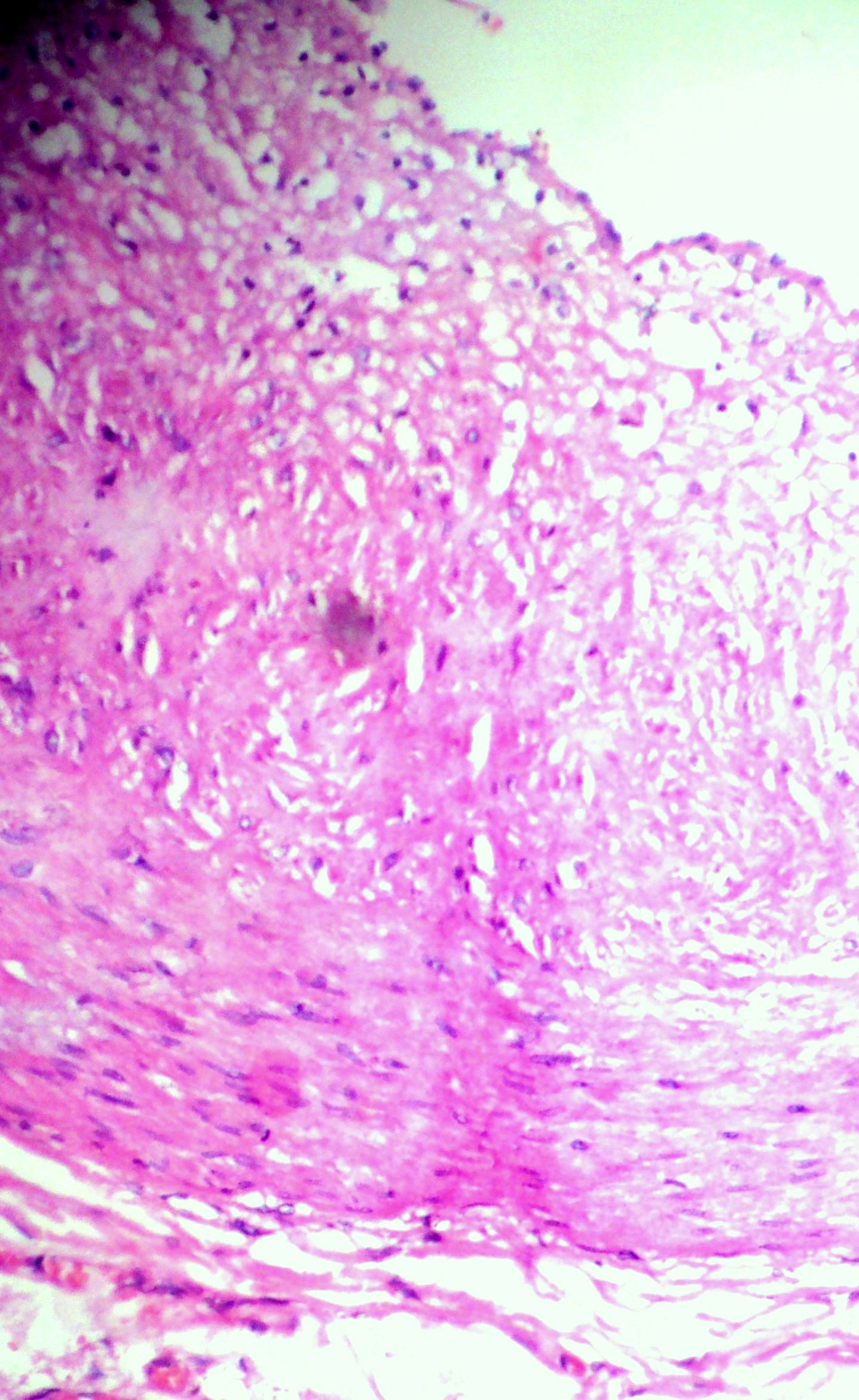
(400X) Haemtoxylin & Eosin stain show Intimal xanthoma in coronary artery
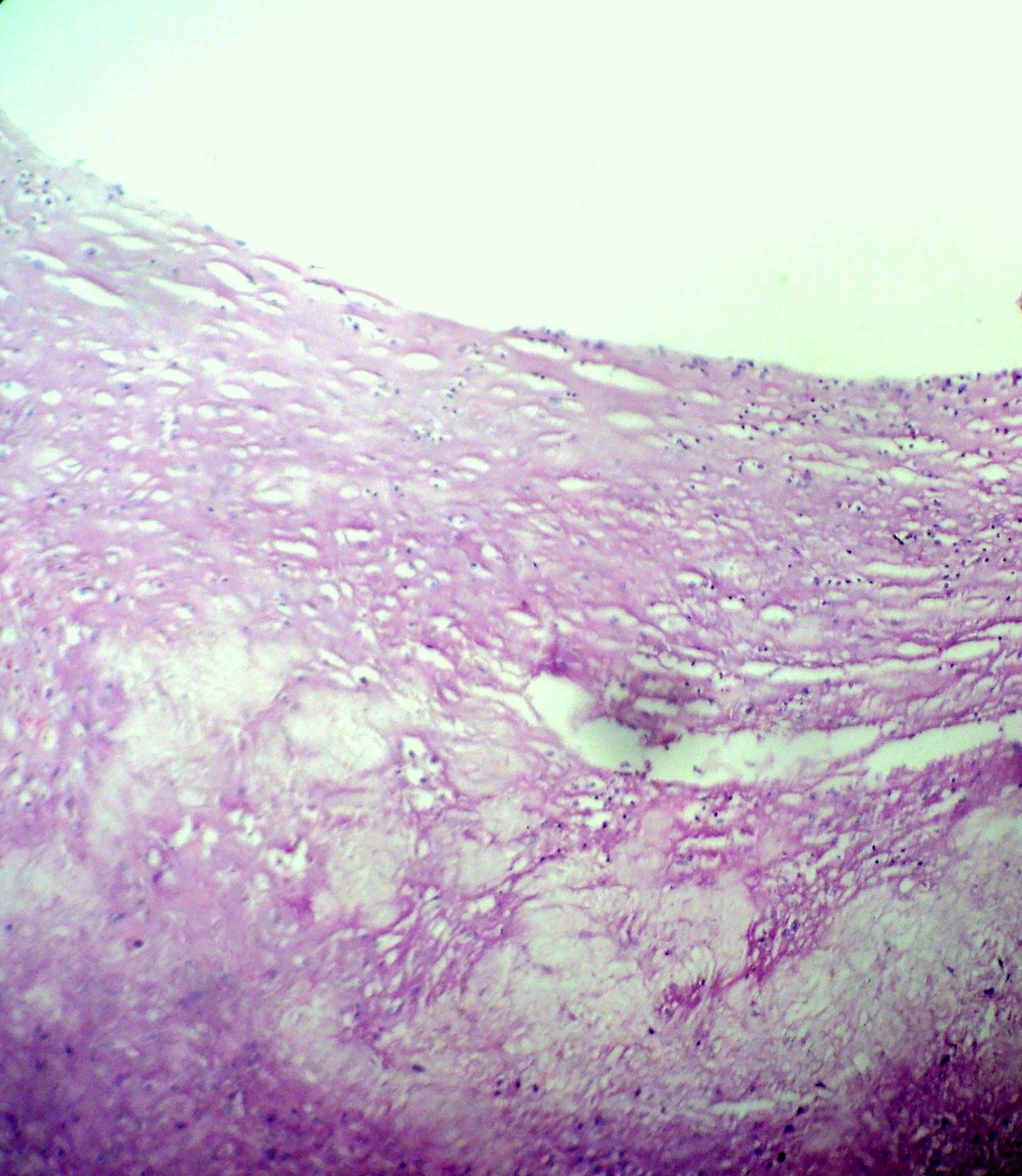
(400X)Haemtoxylin & Eosin stain show Pathological intimal thickening in coronary artery
Coronary Artery based distribution, according to Modified AHA classification of atherosclerosis based on morphological description
| Lesion | LAD | LCA | RCA |
|---|
| Intimal Thickening | 29 | 23 | 25 |
| Intimal Xanthoma | 63 | 61 | 60 |
| Progressive Intimal Thickening | 55 | 56 | 58 |
| Fibrous Cap Atheroma | 51 | 54 | 53 |
| Thin Fibrous Cap Atheroma | 32 | 37 | 37 |
| Calcified Nodule | 18 | 14 | 13 |
| Fibrocalcific Nodule | 16 | 19 | 18 |
| Total | 264 | 264 | 264 |
The present study was carried out on 264 hearts, and the age of the subjects ranged from 8 to 79 years. Maximum number of cases belonged to the 40-49 years (20%), followed by 30-39 (17%), 50-59 years & 60-69 years (16%). Out of the 264 cases 168 were male (64%) & 96 were female (36%) [Table/Fig-5].
Distribution of cases in age & sex wise distribution
| Age Groups | Male | female | Total | Percentage |
|---|
| 0–9 years | 1 | 1 | 2 | 1% |
| 10–19 years | 11 | 7 | 18 | 7% |
| 20–29 years | 21 | 13 | 34 | 13% |
| 30–39 years | 31 | 15 | 46 | 17% |
| 40–49 years | 32 | 20 | 52 | 20% |
| 50–59 years | 28 | 16 | 44 | 16% |
| 60–69 years | 27 | 14 | 41 | 16% |
| 70–79 years | 17 | 10 | 27 | 10% |
| Total | 168 (64%) | 96 (36%) | 264 | 100% |
Male cases have more atherosclerotic lesion (59 %) compared to female (52%) [Table/Fig-6]. A total 98 cases of younger age group (10-39 years), Pathological intimal thickening lesion (46%) were common & advanced atherosclerotic lesion (14%) were least common in this age group [Table/Fig-3 and 7]. A total 164 cases of older age group (40-79 years), Pathological intimal thickening lesion (41%) were common followed by advanced atherosclerotic lesion (35%) were common in this age group. 60% of younger age group shows changes of atherosclerosis & 76% of older age group show changes of atherosclerosis. Thus, advanced atherosclerotic lesions were more common in older age group compared to younger age group & pathological intimal thickening were more common in younger age group, which are precursor lesion for development of advanced atherosclerotic lesion [Table/Fig-8].
Distribution of atherosclerosis in gender according to Modified AHA classification based on morphological description
| No. of Gender Cases | Type of atherosclerosis | No. of Coronary | Percentage |
|---|
| Male n = 168(64%) | Non atheromatous | 68 | 41% |
| Pathological intimal thickening | 54 | 32% |
| Advanced athresclerotic lesion | 46 | 27% |
| Female n = 96(36%) | Non–atheromatous | 46 | 48% |
| Pathological intimal thickening | 34 | 35% |
| Advanced atherosclerotic lesion | 16 | 17% |
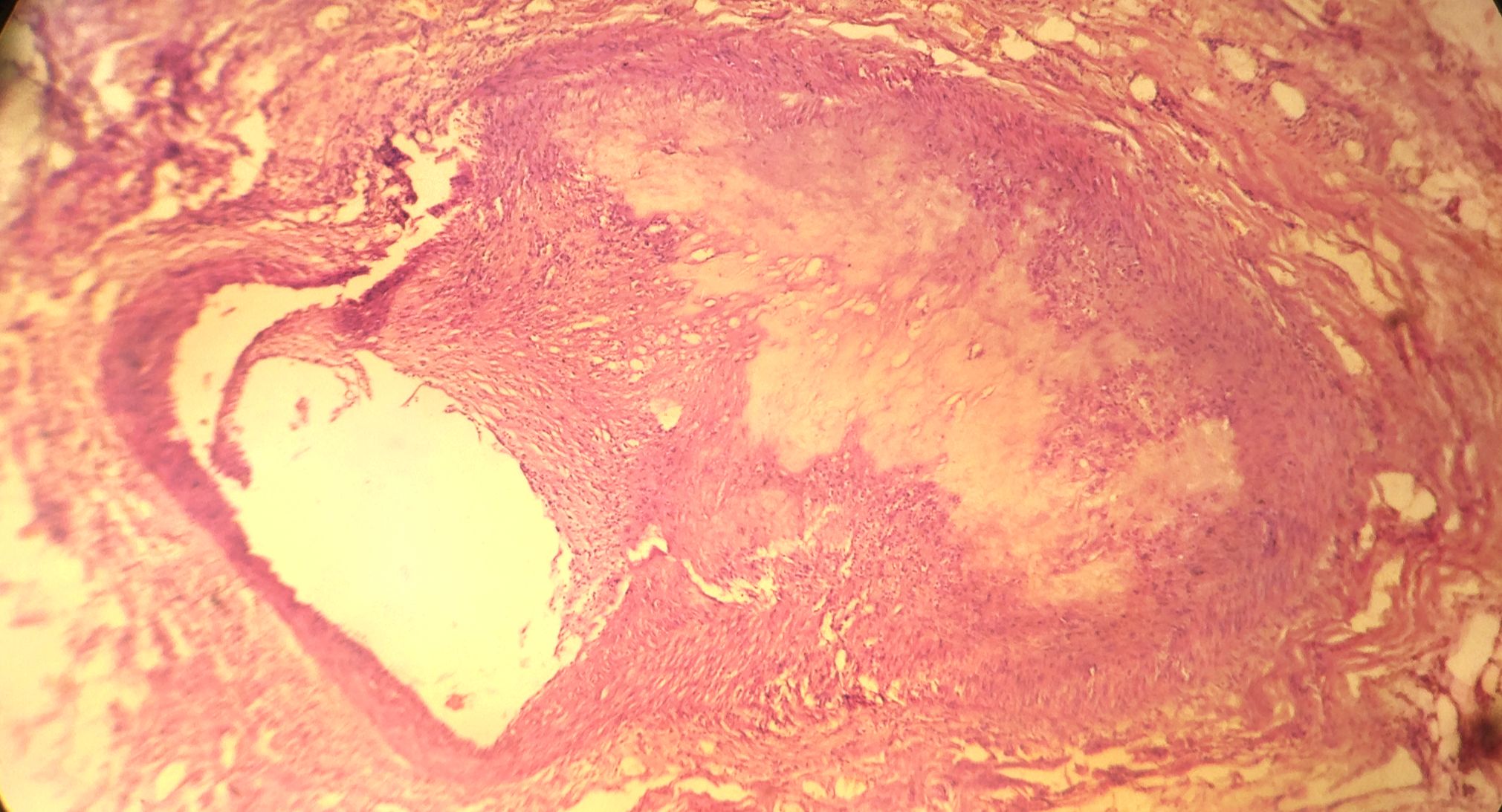
(100X)Haemtoxylin & Eosin stain show marked advanced atherosclerosis in coronary artery
Distribution of atherosclerosis in Young & Old individuals, according to Modified AHA classification based on morphological description
| No. of cases | Type of atherosclerosis | No. of Coronary | Percentage |
|---|
| Young Individuals (10–39 Years) n =98 | Non atheromatous | 39 | 40% |
| Pathological intimal thickening | 45 | 46% |
| Advanced atherosclerotic lesion | 14 | 14% |
| Old Individuals (40–79 Years) n =164 | Non–atheromatous | 39 | 24% |
| Pathological intimal thickening | 68 | 41% |
| Advanced atherosclerotic lesion | 57 | 35% |
Discussion
Atherosclerosis has been a human disease for more than 3,500 years; it occurred in Egyptian mummies and showed the same pathologic features that are observed in modern times [9]. Epidemiological studies performed in last 50 years have revealed that there is a significant rise in prevalence of coronary artery disease in urban as well as in rural Indian population and Coronary Artery Disease (CAD) has been predicted to assume epidemic proportions in India by the year 2015 [10,11].
Coronary Artery Disease has a multi-factorial aetiology. Rapid change in dietary habits & life style coupled with less physical activity, behavioral risk factors, tobacco and alcohol usage are responsible for about 80% of coronary heart disease in India as a consequence of urbanization may partly explain the escalation of CAD. The greater cause for concern is the early age of CAD deaths in the developing countries compared to the developed countries, which cripple the major work force of the nation [12,13].
Atherosclerosis is a disease of the arterial wall consists of gradual lifelong continuum of histological changes characterized by lipid retention, oxidation & modification, which provoke chronic inflammation, ultimately causing thrombosis or stenosis. In the natural course of atherosclerosis, spontaneous regression of early-stage lesions may occur, but the intermediate and advanced stages appear to be continuously progressive. The life of an atherosclerotic plaque can be divided into three stages: (1) initiation and formation, (2) adaptation and (3) clinical. Biologically active molecules regulate several dynamic cellular functions. Identification of a single “master” atherogenic gene responsible for most atherosclerosis is unlikely. Rather, one should consider that multiple gene defects and/or polymorphisms interact with the environment and with each other. When an imbalance between proatherogenic and antiatherogenic factors and processes favors atherogenesis, atherosclerotic plaques begin and grow.
In the present study using modified AHA classification of atherosclerosis is a better than earlier classification & define intermediate lesion that are precursor for atherosclerosis in future.
Most plaques that rupture show less than 50% luminal stenosis, and over 95% are less than 70% stenosed. Plaque rupture often occurs at the shoulder of the plaque, suggesting that hemodynamic shear stress weakens and tears the fibrous cap. If not repaired, endothelial loss leads to plaque erosion, weakening the fibrous cap and exposing the plaque to blood constituents. Plaque rupture occurs in atherosclerotic plaques with a thin fibrous cap overlying a necrotic core that is rich in lipids and it is the most important mechanism of plaque instability that leads to coronary thrombosis [14].
Barker’s group originally examined cardiovascular mortality in men born in Hertfordshire, England & proposed hypothesis. Deaths from ischaemic heart disease were indeed commoner in men who had been small at birth and at 1 year. As an adaptation to under nutrition in fetal life permanent metabolic and endocrine changes occur this would be beneficial if nutrition remained scarce after birth. If nutrition becomes plentiful, however, these changes predispose to obesity and impaired glucose tolerance. Indian babies are exceptionally small, with a mean birth weight of only 2700 g, and 30% have a birth weight of 2650 g or less. The hypothesis predicts that more heart disease and impaired glucose tolerance will be seen in a population that is undergoing transition from sparse to better nutrition. Low birth weight generally seen in many babies born in a semi-urban and rural population as in this study could play role in the development of early atherosclerosis [15].
In the Present study, the degree of involvement of atherosclerosis in LAD (42%) was more compared to LCA(40%) & RCA(39%). Our study is concordant with study done by Sudha et al., showed LAD(47%), Thej et al., & Yazdi et al., showed showed LAD(60%), followed by RCA (50%) and LCA(42.5%) [16,4,17].
In the present study, younger age group (10-39 years), out of the 98 cases, 46% shows intermediate lesion (Pathological intimal thickening) which is a precursor for future atherosclerosis & 14% shows advanced atherosclerotic lesion (fibrous cap atheroma). Similarly, in the present study, older age group (40-79 years), out of the 164 cases, 41% shows Pathological intimal thickening & 35% shows advanced atherosclerotic lesion. Our results are concordant with study done by Fausto et al., showed 10% of young people showed atherosclerosis in western population [18]. Puri N et al., showed 33% in 15-20 year age group & 100% evidence of atherosclerosis in the above age of 25 years in Indian population using earlier AHA classification [5]. Yazdi SAT et al., showed 25% in 21-30 year population & 78.5% in older population in Iran [17].
In the present study, it was observed that 168 cases (64%) were males and 98 (36%) were females, which are concordant with the Bhargava et al studied 74.8% males and 24.2% females, Tandon found 66.5% males and 33.5% females in their study [19,20].
In the present study, 59% of male showed atherosclerosis & 52% of female showed atherosclerosis which are concordant with the study of Thej et al., showed 62% were males & 50% were females in Indian population [4]. Study reported by Yazdi SAT et al., showed 73% males and 61% females had atherosclerosis in a population of Iran. This difference is again explained by the demographic, geographic, racial, lifestyle & dietary variation in population [17] Singh H et al., have reported the incidence of atherosclerosis in the coronaries to be 68% in males and 27% in females [21].
Our study has limitation. No information regarding cardiovascular risk factor such as lipid profile, blood glucose & any past cardiac disease was available of the individual autopsied. To overcome this limitation in a large country like India, having considerable urban-rural life style, habit differences & socio-regional diversity. We need to do large multi–centre prospective long term follow up studies of the CAD & atherosclerosis.
Conclusion
In the twenty first century, cardiovascular disease has become a ubiquitous cause of morbidity and a leading contributor to mortality in most countries including India. Autopsy-based studies for studying the prevalence of atherosclerosis in a population are cost-effective procedures and help in estimating the future disease burden in the population particularly in developing nation like India. An increased prevalence of atherosclerosis was found in the males compared to females indicating that preventive measures, screening of cardiovascular risk factor, life style modification & change of dietary habits should be instituted early in the third decades of young Indians.