Ventilator-associated pneumonia (VAP) refers to the development of parenchymal lung infection after a patient has undergone intubation and received mechanical ventilation (MV) for ≥ 48 hours [1].
The main route for acquiring VAP is gross or micro aspiration of oropharyngeal organisms into the distal bronchi, either directly or secondarily by reflux from the stomach into the oropharynx. Other potential routes are less common, such as haematogenous carriage of microorganisms to the lung from remote sites of local infection (eg, catheter-related bloodstream infections or from the environment, especially from the hands of health care workers) or contaminated respiratory equipment, bronchoscopes, medical aerosols, water or air [2].
Early-onset VAP, defined as occurring within the first 4 days of hospitalization, usually carry a better prognosis, and are more likely to be caused by antibiotic sensitive bacteria. Late-onset VAP (5 days or more) are more likely to be caused by multidrug-resistant (MDR) pathogens, and are associated with increased patient mortality and morbidity [1].
But the etiologic agents widely differ according to the population of patients in an intensive care unit, duration of hospital stay, and prior antimicrobial therapy [3]. Despite the advancements in antimicrobial regimes, VAP continues to be an important cause of morbidity and mortality. VAP requires a rapid diagnosis and initiation of appropriate antibiotic treatment, as there is adverse effect of inadequate antibiotic treatment on patient’s prognosis and the emergence of multidrug-resistant (MDR) pathogen [4]. Inadequate antimicrobial therapy, such as inappropriate antimicrobial coverage, or delayed initiation of antimicrobials has been associated with higher hospital mortality in subjects with hospital acquired pneumonia (HAP) or VAP [5].
The presence of HAP increases hospital stay by an average of 7-9 days per patient [6], also imposes an extra financial burden to the hospital. The risk of VAP is highest early in the course of hospital stay, and is estimated to be 3%/day during the first 5 days of ventilation, 2%/day during days 5-10 of ventilation and 1%/day after this [7].
Detection of the causative organism is crucial for the diagnosis of VAP. This is done by collecting the lower respiratory tract sample either by invasive (protected specimen brush [PSB] or broncho-alveolar lavage [BAL]) or non-invasive (endotracheal aspirate [ETA]) techniques and culturing quantitatively or semi-quantitatively. The American Thoracic Society (ATS) guidelines recommend that quantitative cultures can be performed on ETA or samples collected either bronchoscopically or non-bronchoscopically [1].
Therefore, the microbiological differentiation between early-onset and late-onset VAP has been implicated in the selection of broad spectrum antimicrobial coverage for MDR pathogens. Because appropriate antimicrobial treatment of patients with VAP significantly improves outcome, more rapid identification of infected patients and accurate selection of antimicrobial agents represent important clinical goals [3].
Therefore, this study aims at characterising the etiological agents of early and late onset VAP isolated from endotracheal aspirates from clinically suspected VAP cases.
Material and Methods
Study design
We conducted a retrospective study over a period of 12 months (February 2012 -February 2013). The data were collected from the case records of the patients who were admitted to the intensive care unit of the tertiary care hospital in Bangalore, India.
We assessed the clinical parameters which included the history, the number of days the patient spent on ventilator, the timing of sample collection, clinical examination of the patient and relevant investigations. This included the blood counts, renal function tests, blood glucose, liver function tests, endo-tracheal aspirates for gram staining and culture, blood culture, ABG (arterial blood gas analysis) and chest X-rays or any other relevant investigations.
Inclusion criteria: Patients on mechanical ventilation for more than 48 hours.
Exclusion criteria: Patients with pneumonia prior to mechanical ventilation or within 48 hours of mechanical ventilation, patients with Adult Respiratory Distress Syndrome (ARDS), cavitary lung disease based on chest X-ray findings, primary lung cancer or another malignancy metastatic to the lungs and cystic fibrosis. Tuberculosis patients and patients with acquired, induced or congenital immunodeficiency, leukopenia <1000 cells/mm3, neutropenia <500 PN/mm3 were also excluded from the study.
During this period 148 patients, who were on mechanical ventilation for more than 48 hours were studied. The patients fulfilling both the clinical and microbiological criteria were diagnosed as VAP cases and the remaining were categorized as non-VAP cases. Microbiological criteria included positive Gram stain (>10 polymorphonuclear cells / low power field and ≥1 bacteria/ oil immersion field). Clinical criteria included modified Clinical Pulmonary Infection Score (CPIS) > 6 [Table/Fig–1], developed by Pugin et al., [8].
CPIS: Clinical pulmonary infection scoring
| CPIS points | 0 | 1 | 2 |
|---|
| Tracheal secretions | Rare | Abundant | Purulent |
| Leukocyte count (mm3) | >4,000 and <11,000 | <4,000 and >11,000 | <4,000 or >11,000 + band forms |
| Temperature (oC) | >36.5 and < 38.4 | >38.5 and < 38.9 | >39 or <36 |
| PaO2/FiO2 ratio (mmHg) | >240 or ARDS | - | ≤240 and no ARDS |
| Chest radiograph | No infiltrate | Diffuse infiltrate | Localized infiltrate |
| Culture of tracheal aspirate | Negative | - | Positive |
Patients on mechanical ventilation for less than 4 days (48-96 hours) were included in the early-onset VAP group and 5 days or more were included in the late onset VAP group [1].
Processing of sample
The endotracheal aspirates sent to the lab were processed immediately [9]. The samples were first subjected to Gram’s staining and then quantitative cultures were performed.
Samples were mechanically liquefied and homogenized by vortexing for 1 min. The 0.01 mL of sample solution was then plated on sheep blood agar, chocolate agar (CA), MacConkey agar by using 4 mm Nichrome wire loop (Hi-Media, Mumbai, India). All plates were incubated overnight at 37°C and CA plates at 37°C in candle jar. All plates were checked for growth overnight and then after 24 and 48 h of incubation.
For definite diagnosis of VAP, 105 CFU/ mL was considered as threshold [10]. Growth of any organism below the threshold was assumed to be due to colonization or contamination. Any growth was characterized by colony morphology and Gram’s staining from the plates.
A detailed biochemical testing identified any significant growth, and antibiotic sensitivity testing was performed on Mueller–Hinton agar plates by Kirby—Bauer disc diffusion method. Zone diameter was measured and interpreted as per the Clinical and Laboratory Standards Institute (CLSI) guidelines [11]. Suspected extended-spectrum beta lactamases (ESBLs) producing organisms were confirmed by double disk synergy test as described previously [12]. Detection of plasmid-mediated AmpC was done by the AmpC disk test and the isolates showing reduced susceptibility to carbapenems (imipenem and meropenem) were selected for detection of metallo-beta lactamases (MBLs) enzymes by imipenem-EDTA disk method [13]. For quality control of disc diffusion tests ATCC control strains of Escerichia.coli ATCC 25922, Staphylococcus aureus ATCC 25923 and Pseudomonas. aeruginosa ATCC 27853 strains were used.
Statistical Analysis
The results were expressed as percentages for the analysis of various data. Microsoft excel was used for the interpretation of these results.
Results
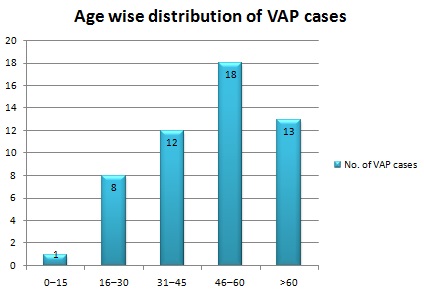
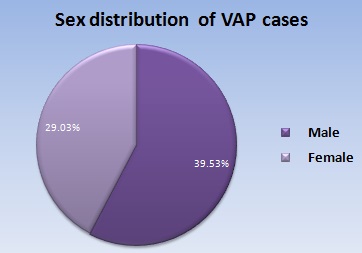
A total number of 148 patients were included in this study, as they were on mechanical ventilator for more than 48 hours during the study period. Out of 148, only 52 patients were diagnosed as VAP cases based on clinical and microbiological grounds [Table/Fig-2a,2b]. The incidence of VAP was more common in men (39.53%) than females (29.03%) [Table/Fig-3a,3b].
Age-wise distribution of VAP cases
| Age (years) | Total patients (n=148) | VAP (n=52) | Non-VAP (n=96) |
|---|
| 0–15 | 2 | 1 (50%) | 1(50%) |
| 16–30 | 30 | 8(26.67%) | 22 (73.33%) |
| 31–45 | 38 | 12(31.58%) | 26(68.42%) |
| 46–60 | 46 | 18(39.13%) | 28 (60.87%) |
| >60 | 32 | 13(40.63%) | 19(59.37%) |
Age-wise distribution of VAP cases (Graphicalrepresentation)
Gender distribution of VAP cases
| Gender | No. of VAP cases (n=52) | No. of cases in whom VAP was absent (n=96) | Total no. of cases (n=148) |
|---|
| Male | 34(39.53%) | 52(60.47%) | 86(100%) |
| Female | 18(29.03%) | 44(70.97%) | 62(100%) |
Gender distribution of VAP cases (Pie-chart)
The occurrence of VAP was more common in the age group of 46-60 years (18%).
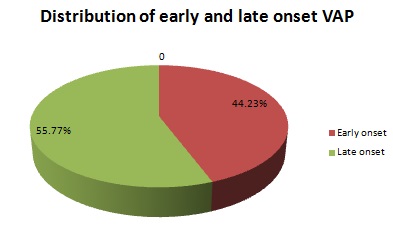
The incidence of VAP in our study was 35.14%. Out of the 52 VAP cases, 23(44.23%) were categorized under early onset VAP and 29 (55.77%) under late onset VAP [Table/Fig-4a,4b].
Distribution of early and late onset VAP cases
| Duration of ventilation | No. of VAP cases (n=52) |
|---|
| Early onset VAP | 23 (44.23%) |
| Late onset VAP | 29 (55.77%) |
Distribution of early and late onset VAP cases(Pie-chart)
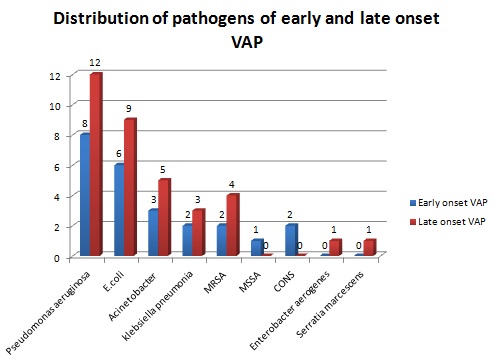
Among the 52 VAP cases, 45(86.54%) were monomicrobial (one bacterial species in ETA) and 7 (13.46%) were polymicrobial (two bacterial species in ETA), thus yielding 59 isolates [Table/Fig-5a,5b]. shows that Pseudomonas aeruginosa is the commonest isolate causing both early and late onset pneumonia 20(33.9%) followed by E.coli 15(25.42%) and Acinetobacter baumanii (13.56%)
Organisms isolated from early and late onset VAP cases
| Pathogens | Early onset VAP | Late onset VAP | Total |
|---|
| Pseudomonas aeruginosa | 8(33.33%) | 12 (34.29%) | 20(33.9%) |
| E.coli | 6(25%) | 9 (25.71%) | 15(25.42%) |
| Acinetobacter baumanii | 3(12.5%) | 5 (14.29%) | 8(13.56%) |
| Klebsiella pneumonia | 2 (8.33%) | 3 (8.57%) | 5(8.47%) |
| MRSA | 2 (8.33%) | 4(11.43%) | 6(10.17%) |
| MSSA | 1 (4.17%) | 0 | 1(1.69%) |
| CONS | 2 (8.33%) | 0 | 2(3.4%) |
| Enterobacter aerogenes | 0 | 1 (2.86%) | 1(1.69%) |
| Serratia marcesens | 0 | 1 (2.86%) | 1(1.69%) |
| Total | 24 | 35 | 59 |
Organisms isolated from early and late onset VAP cases(Graphical representation)
[Table/Fig-6]. shows the resistance pattern in gram negative bacteria isolated in this study. The gram negative bacilli showed 100% resistance to ampicillin. All the Enterobacteriaceal isolates were ESBL producers. None of the strains were AmpC producers. Among the 20 Pseudomonas aeruginosa isolates, 8 (40%) were resistant to all groups of antibiotics, including carbapenems. 3 out of 8 (37.5%) Acinetobacter baumanii, showed resistance to all groups of drugs including carbapenems. MBL production was detected in 25% of Pseudomonas aeruginosa and 25% of Acinetobacter baumanii isolates. 100% of the gram positive isolates were resistant to penicillin. Six out of 7 Staphylococcus aureus strains were methicillin resistant. Fifty percent of the CONS (Coagulase-negative Staphylococcus aureus) was resistant to cefoxitin and erythromycin. However, all the gram positive cocci were sensitive to vancomycin and linezolid [Table/Fig-7].
Antibacterial resistance pattern of gram negative bacilli (%)
| Pseudomonas aeruginosa (n=20) | E.coli (n=15) | Acineto- bacter baumanii (n=8) | Klebsiella pneumonia (n=5) | Enterobacter aerogenes (n=1) | Serratia marcescens (n=1) |
|---|
| AMP | NT | 100 | NT | 100 | 100 | 100 |
| CFS | 40 | 0 | 37.5 | 0 | 0 | 0 |
| AMI | 70 | 53.33 | 62.5 | 40 | 100 | 100 |
| GEN | 80 | 66.66 | 62.5 | 66.66 | 100 | 100 |
| TBR | 70 | NT | 62.5 | NT | NT | NT |
| NET | 65 | 26.66 | 37.5 | 20 | 0 | 0 |
| CAZ | 55 | 100 | 75 | 100 | 100 | 100 |
| CTX | NT | 100 | NT | 100 | 100 | 100 |
| CIP | 60 | 66.66 | 62.5 | 66.6 | 100 | 100 |
| TZP | 55 | 0 | 75 | 0 | 0 | 0 |
| IMP | 40 | 0 | 37.5 | 0 | 0 | 0 |
| MRP | 40 | 0 | 37.5 | 0 | 0 | 0 |
| AZT | 25 | 100 | 25 | 100 | 100 | 100 |
Antibacterial resistance pattern of the Gram positive cocci (%)
| Antibiotics | Staphylococcus aureus n=7) | CONS (n=2) |
|---|
| PEN | 7 (100%) | 2(100%) |
| AMC | 6 (85.71%) | 0 |
| CXN | 6 (85.71%) | 1 (50%) |
| ERY | 5(71.43%) | 1 (50%) |
| CLD | 3 (42.86%) | 0 |
| LZD | 0 | 0 |
| VAN | 0 | 0 |
AMP-Ampicillin, CFS - Cefoperazone – Sulbactam, AMI – Amikacin, GEN - Gentamicin, TBR- Tobramycin, NET - Netilmycin, , CAZ – Ceftazidime, CIP - Ciprofloxacin, CTX - Cefotaxime, TZP - Pipercillin-Tazobactam, IMI - Imipenem, MRP - Meropenem. AZT – Aztreonam, PEN- penicillin, AMC- Amoxyclav, CXN- Cefoxitin, ERY- Erythromycin, CLD- Clindamycin, LZD- Linezolid, VAN- Vancomycin; NT – Not tested.
Discussion
The administration of accurate and timely initial empirical antibiotic therapy has been shown to have a major impact on mortality from nosocomial pneumonia. Because early-onset nosocomial pneumonia is most often reported as being due to antibiotic-sensitive pathogens, while late-onset nosocomial pneumonia is frequently caused by more-resistant pathogens, guidelines recommend monotherapy with narrow-spectrum antibiotics for early-onset infections and broad-spectrum therapy for late-onset infections [14].
The bacteriological approach for the management of VAP avoids the problem of over treatment by separating colonizers from infecting pathogens. Several methods to avoid contamination have been proposed like the use of invasive bronchoscopic methods and bronchial biopsy for sampling from the site of infection and a protected specimen brush. These methods have been shown to be highly specific in diagnosing VAP [15]. However, bronchoscopy is not accessible in many settings and because of the invasive nature and cost of the bronchoscopy, and investigators have evaluated other techniques for collecting lower respiratory tract secretions. Several methods to obtain good respiratory samples have been extensively investigated; each technique having its own diagnostic threshold and methodological limitations. The choice of method depends on expertise, experience, availability and cost [9]. Some studies have also shown that those patient outcomes were similar irrespective of the method used for diagnosis (bronchoscopic or endotracheal aspiration) [16].
The incidence of VAP in our study was 35.14%, which was similar to studies done by Shalini et al., (35.78%) [17] and Gadani et al., (37%) [18]. Even higher incidence rates were reported by Dey et al., (45.4%) [19] and Rajashekaran et al., who reported a very high incidence rate of 73% [9].
Our study shows that patients in the age group of 46-60 years were more prone to VAP as the number of patients exposed to mechanical ventilation (>48hours) were also more in this age group and this was found in accordance with earlier studies [4]. The incidence of VAP was more in males (39.53%) compared to females (29.03%) which was similar to studies conducted by Sharma et al., [20].
Out of 52 VAP cases, 44.23% were categorized under early-onset VAP and 55.77% under late-onset VAP which was in concordance with studies conducted by Dey et al., [19] and Chastre et al.,[3]. Rates of polymicrobial infection vary widely. In our study only 13.46% of cultures were polymicrobial. In a study by Singhal et al., 12.3% were polymicrobial [21]. Other studies have reported even higher rates [22].
Pseudomonas aeruginosa and E.coli were the commonest isolates obtained in both early and late onset VAP cases, which were also reported as the commonest isolates by other studies (Sharma et al., [20], Mukhopadhyay et al., [23].
Few studies have shown gram positive cocci mainly Staphylococcus aureus and Streptococcus pneumonia as the most frequently isolated organism in early onset VAP which is in contrast to our study [24]. Restrepo et al., and co-workers (2013) reported gram negative bacilli as the commonest etiological agents of late onset VAP which remains the same in our study also [25].
All the Enterobacteriaceae were ESBL producers. Dey et al., also observed a high prevalence of ESBL producers in their study [19]. Meropenem resistance was high in this study as 40% of the Pseudomonas and 37.5 % of Acinetobacter species showed multi-drug resistance (MDR), even to carbapenems, which is in concordance with other studies [19,26]. Whereas certain studies reported a lower incidence of meropenem resistance [4,20]. 85.71% of Staphylococcus aureus strains were MRSA. Among the 6 MRSA strains, 4 were isolated from patients with late onset VAP. The high incidence of MRSA in our study correlates well with studies done by Gupta et al., [27]. The overall picture suggests that number of drug-resistant strains of various organisms is rising and is an important cause of VAP in our setting.
Therefore, this study suggests that most cases of VAP in our setting are those of late-onset VAP and a majority of these are caused by highly resistant strains and also the frequency of specific MDR pathogens causing VAP may vary by hospital, patient population, and exposure to antibiotics, type of ICU patients and changes over time, emphasizing the need for timely local surveillance data.
Conclusion
In conclusion, the present study showed a gradual increase in VAP cases along with the duration of stay in ICU, with its occurrence being most in the age group 46-60 years. This study showed that quantitative culture of ETA is a useful test for early diagnosis of VAP and provides specific knowledge of the causal agents associated with early and late onset VAP along with their sensitivity pattern, which will help as an epidemiological marker for initial prophylactic and treatment planning for mechanically ventilated patients in our ICU setup. Also adherence to infection control protocols and short term use of invasive devices and judicious use of antibiotics are important in preventing VAP caused by these MDR pathogens.