Human brain and its complex vascular network may be viewed as a “three pound biological computer”. It is composed of billions of specialised cells and circuits which make it the most vital organ in the human body. It is richly supplied with blood vessels which provide oxygen and other essential nutrients. Brain is supplied by two internal carotid and two vertebral arteries, connected by a central anastomosis – circulus arteriosus, which lie in the interpeduncular fossa at the base of brain. The internal carotid artery divides into the anterior and middle cerebral arteries. The two anterior cerebral arteries are joined together by an anterior communicating artery. The basilar artery formed by the union of the two vertebral arteries, branches into two posterior cerebral arteries.The posterior communicating artery, a branch of internal carotid completes the arterial polygon by joining with the posterior cerebral artery. A classical arterial circle is bilaterally symmetrical and a complete ring of vessels. There may be variations in this typical configuration. Vessels generally vary in caliber; often they are hypoplastic, duplicated or even absent [1]. Several studies have shown that these variations play an important role in the development of cerebrovascular diseases [2]. Anatomical variations are probably genetically determined, develop in early embryonic stage and persist in post-natal life [3]. Any change in the normal morphology of the circle may condition the appearance and severity of symptoms of cerebrovascular disorders, such as aneurysms, infarcts and other vascular anomalies [4]. Arterial aneurysms such as berry aneurysms and arterial variations are interconnected. Aneurysms usually tend to occur at branches or at the bifurcations of cerebral arteries [5]. There is a possible link between the anomalies of circle of Willis and the mentally ill and patients with cerebrovascular catastrophy [6–8]. The state of the circle becomes important in determining the adequacy of the brain circulation in operations for cerebral aneurysms and also in ligation of the internal carotid artery. A thorough knowledge of the variations of vessels is useful to surgeons in planning their shunt operations and the choice of the patients. These problems make it desirable to have an intimate knowledge of the variations in the anatomy of the cerebral arterial circle and try to correlate these anomalies to the occurrence of the certain common clinical conditions such as stroke, aneurysms and other arterio-venous malformations. The inferences obtained from this study are also useful to anatomists and sonologists in enhancing their knowledge in teaching and investigative procedures.
Material and Methods
Fifty randomly selected specimens were obtained during routine autopsy studies. The specimens were collected after obtaining the ethical clearance from the institute. The base of the brain including the brainstem with intact arterial circle was sliced horizontally and preserved in 10% formalin for 10 days. The circle of Willis, each major cerebral artery to the point of its major division distal to the circle, basilar artery and the sub-arachnoid portion of each vertebral artery were carefully dissected under water using a magnifying lens. The specimens were then dried and the blood vessels were painted with Fevicryl red poster colour. The circles were then numbered and photographed. The circle of Willis was then analysed with special reference to the following factors - whether the circle is complete or incomplete, any asymmetry in the configuration and variations in the size, and number of the component vessels, and absence, duplication or triplication of any of the vessels. The arteries examined were the anterior communicating artery, the proximal and the distal (1cm) segments of the anterior cerebral, the internal carotid distal to the origin of the posterior communicating, middle cerebral at its beginning, the posterior communicating, the proximal and distal (1cm) segments of the posterior cerebral, basilar and the sub-arachnoid portion of the vertebral arteries. The results obtained were tabulated.
Results
The circles were classified into two main groups.
1. Normal circles and 2. Anomalous circles.
1. Normal circles
The Internal carotid artery bifurcates at the medial end of the Sylvian fissure into anterior and middle cerebral arteries. The two anterior cerebral arteries are joined at the anterior end of the longitudinal fissure by the anterior communicating artery. The basilar artery bifurcates at the ponto-mesencephalic junction into two posterior cerebral arteries, which are in turn connected to the ipsilateral internal carotids by the posterior communicating artery. The normal circle is more polygonal and it is symmetrical in configuration. Of the total fifty circles which form the basis for this study, 24 circles (48%) were found to be ‘normal’ in anatomical configuration [Table/Fig-1].
Photograph of the Normal circle of Willis

2. Anomalous circles
In the present series 26 circles (52%) were found to be anomalous. The anomalies encountered were discussed under the following sub headings.
1. Attenuated Vessels
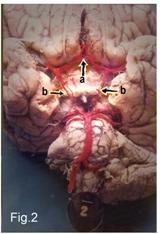
The most common anomaly of the circle of Willis in normal brains was hypoplasia of one or other components of the circle. Arteries of less than 1 mm in external diameter were considered hypoplastic, except for the communicating arteries, where less than 0.5 mm was considered hypoplastic. Such hypoplastic vessels were encountered either alone or in combination with other anomalies in 12 circles (24%). Of these vessels, the posterior communicating artery was the most frequent to be hypoplastic, followed by the circular part of the posterior cerebral artery (P-1 segment), circular part of the anterior cerebral artery (A-1 segment) and the anterior communicating artery [Table/Fig-2]. The relative incidence of hypoplasia was depicted in [Table/Fig-3]. On examination with magnifying lens, majority of the hypoplastic vessels in this series were found to be patent.
Photograph of the hypoplastic Posterior and Anterior communicating arteries. a) Hypoplastic ACOA; b) Hypoplastic PCOAs
Incidence of hypoplastic vessels in this study
| Name of the Vessel | Incidence (%) |
|---|
| Posterior communicating artery | 10 |
| Posterior cerebral artery (circular part P-1 segment) | 6 |
| Anterior cerebral artery (circular part A-1 segment) | 4 |
| Anterior communicating artery | 4 |
| Total | 24 |
2. Accessory vessels
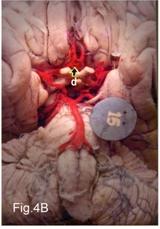
Accessory vessels were present in the form of duplications/triplications of one of the components of the polygon. Such accessory vessels were found in six circles (12%) in this series. Majority of these duplications had occurred in the anterior portion of the circle - in the anterior communicating (8%) [Table/Fig-4A and 4B] and anterior cerebral arteries (4%). In the cases of double anterior communicating arteries, one of the two vessels was found to be hypoplastic, but it was patent. A mid-line persistent corpus callosal branch arising from the anterior communicating artery was seen in two circles (4%) [Table/Fig-5]. This triplicate anterior cerebral artery occurred as the only anomaly in one circle and combined with multiple anomalies in the other circle. This mid-line aberrant vessel was usually about the same diameter as the right and left anterior cerebral arteries.
Photograph of the duplications of Anterior communicating artery. c) Duplicated ACOAs

Photograph of the triplications of Anterior communicating artery. d) Triplicated ACOAs
Photograph of the triplicate Anterior cerebral arteries e) Triplicate ACAs

3. Anomalous origin
The persistence of the embryonic derivation of the posterior cerebral artery from the internal carotid was encountered in five circles (10%). This vessel was connected to the basilar artery by a small communicating type of vessel. This was present as a bilateral symmetrical anomaly in two circles (4%) [Table/Fig-6A] and as a unilateral anomaly in three circles (6%) [Table/Fig-6B].
Photograph of the bilateral embryonic origin of Posterior cerebral from Internal carotid arteryf) Bilateral embryonic origin of PCAs

Photograph of the unilateral embryonic origin of Posterior cerebral from Internal carotid artery g) Unilateral embryonic origin of PCA

4. Absent vessels
The least common anomaly of the circle of Willis was the absence of one or other posterior communicating arteries. Complete absence of a posterior communicating artery on one side was found in three circles (6%). The absence of an anterior communicating artery was not encountered in this series.
5. Circles with multiple anomalies
Of the total 50 circles included in this series, 12 circles (24%) exhibited a single anomaly in one of the component vessels. Multiple anomalies were found in 14 circles (28%). Among the multiple anomalies 10 circles (20%) had two anomalies. More than two anomalies were found in 4 circles (8%). Among the multiple anomalies hypoplastic posterior communicating artery was usually combined with opposite embryonic derivation of the posterior cerebral artery and duplication of the anterior communicating artery.
Discussion
The observations made during the present study on the circle of Willis were compared with those recorded in earlier studies on the same topic. The prevalence of the typical circle i.e., the “normal text-book” polygon ranges from 4.6% [9] to 72.2% [10]. A possible reason for the wide range may be due to the diversity in nomenclature and the criteria used to define hypoplastic vessels. In the present study 48% of the circles exhibited the normal configuration. This was compared to 26.8% [11], 53.2% [12] and 45.2% [13] of the Indian population, 14.2% in Sri Lankans [14] and 52.3% in western population [1]. The wide range in the prevalence of the typical configuration among various races warrants further researches to confirm the influence of genetic, regional, environmental and hemodynamic factors or the combination of these factors.
The most common anomaly of the circle of Willis in normal brains has been found to be an attenuation of one of the component vessels. In the present group 24% of the circles showed hypoplastic or string-like vessels. Alpers et al., reported an incidence of 27% [1], Kamath 24% [6], and Fetterman and Moran 23% [15] and the present observations fairly coincide with that of other workers.The usual site of string-like vessels was one or both posterior communicating arteries (PCOA) in this series. The circular part of the posterior cerebral artery (PCA P-I segment) was next to be hypoplastic in this study. The hypoplasia of the anterior segments of the circle viz., the anterior communicating artery (ACOA) and the circular part of the anterior cerebral artery (ACA A-I segment) were less commonly encountered in this series. The incidences of hypoplastic vessels were compared with that of other workers in [Table/Fig-7].
Incidence of hypoplastic vessels as reported in the Literature
| Name of Author | Incidence of hypoplastic vessels (%) |
|---|
| PCOA | PCA (P1 segment) | ACOA | ACA (A1 segment) |
|---|
| Alpers et al., [1] | 22 | - | 3 | 2 |
| Riggs & Rupp [4] | 53 | 17.7 | 9.15 | 11.97 |
| Puchades-Orts et al., [18] | - | 11.3 | 6.4 | 6.4 |
| Kamath [6] | 10 | - | 2 | 2 |
| Milenkovic et al., [21] | - | 7.68 | - | 9.16 |
| Present study | 10 | 6 | 4 | 4 |
The percentage of hypoplasia varied widely as was evident from [Table/Fig-7]. The reason for this wide range may be due to the different criteria used to measure hypoplastic vessels. Vessels with less than 1mm in diameter have been classified as hypoplastic by various authors. Others by using 3 DTFMR angiography measured the vessels with less than 0.8 mm were hypoplastic, while Kamath fixed the diameter 0.5 mm or less were considered hypoplastic [1,2,4,6,10,15–17]. We have followed Kamath’s observations in defining hypoplasia and fixed arterial diameters of less than 1mm and 0.5 mm as hypoplastic for cerebral and communicating arteries respectively. Hypoplasia was more prominent in the posterior portion of the circle of Willis in this study. This finding was in agreement with those of other workers [1,4,6,18]. Alpers et al., Riggs and Rupp, Raja Reddy et al., and Fetterman and Moran have reported that hypoplastic vessels were more commonly occur in the posterior communicating arteries followed by the posterior cerebrals [1,4,12,15]. But Kamath and Fawcett et al., observed that the hypoplasia was more common in the posterior cerebrals than in the posterior communicating arteries [6,10]. The observations made in the present series concur with that of the former.
The minimum threshold diameter for collateral flow through circle of Willis, as assessed by transcranial colour-coded duplex ultrasonography (TCCD) and carotid compression tests, was compared with unfixed postmortem specimens’ lies in the range of 0.4 to 0.6mm. The PCOA threshold diameter for collateral flow was slightly higher than the ACOA, possibly due to greater length of PCOA. The studies conducted so far were silent about the similarity of the postmortem diameters to in vivo measurements and the effect of absent perfusion pressure and possible postmortem shrinking of the arteries [2,14]. The collateral anastomotic polygon usually preserves normal cerebral perfusion in cases hypoplasia/partial blockade of any component vessels. Symptoms of ischemia usually develop when cerebral blood flow decreases less than half of the normal. Initially symptoms are only of Transient ischemic Attack (TIA), by that time the communicating arteries enlarge to maintain normal perfusion for the proper functioning of the brain. However in cases with extensive hypoplasia associated with vascular occlusion, the collateral ability of the circle was deranged, leading to stroke with irreparable brain damage [19].
Accessory vessels in the form of duplications/triplications involving one or more arteries were frequently encountered in the anterior portion of the circle of Willis and were found in 12% of the circles in this series. Among the accessory vessels, duplications/triplications of anterior communicating arteries were commonly occurred followed by triplicate anterior cerebral arteries. The incidence of accessory vessels in this series was compared with that of earlier investigators in [Table/Fig-8]. In the case of triplicate ACAs, the two normal ACAs were accompanied by a midline third anterior cerebral vessel, arising from the anterior communicating artery. Baptista referred the third artery of such triple arteried brains as the accessory ACA. The accessory ACA is of variable length and has almost the same diameter as both the anterior cerebral arteries, and was described as the Median artery of Corpus Callosum (MACC) [20]. It runs in the epicallosal sulcus, while its companion ACAs course on the medial cerebral surface. Milenkovic et al., and Perlmutter and Rhoton have referred this artery as the Arteria Termatica of Wilder [21,22].
Incidence of accessory vessels as reported in the Literature
| Name of the Author | Incidence of accessory vessels (%) |
|---|
| ACOAs | Triplicate ACAs |
|---|
| Duplications | Triplications | Total |
|---|
| Fawcett & Blachford [10] | 7.28 | 0.42 | 7.7 | 3.2 |
|---|
| Alpers et al., [1] | - | - | 9 | - |
| Puchades-Orts et al., [18] | 6.4 | 4.8 | 11.2 | - |
| Milenkovic et al., [21] | 32 | 5 | 37 | 5 |
| Baptista [20] | - | - | - | 13 |
| Present study | 6 | 2 | 8 | 4 |
The embryonic origin of the posterior cerebral artery from the internal carotid persisted as a fairly common anomaly and was found in 10% of the circles in this series. Such a vessel was connected to the basilar artery by a small communicating type of vessel. The recorded incidence of the embryonic origin of the PCA in the literature is compared with the present observation in [Table/Fig-9].
Incidence of embryonic origin of PCA from the Internal carotid
| Name of the author | Incidence of embryonic origin of PCA from ICA (%) |
|---|
| Alpers et al., [1] | 15 |
| Riggs & Rupp [4] | 22 |
| Milenkovic et al., [21] | 21 |
| Present study | 10 |
The reported incidence of absent vessels in the circle of Willis in normal brains leading to incomplete circle ranges from 0.6% [1] to 17% [23]. When absent vessels were reported, they were usually in the region of the posterior communicating artery. Fawcett and Blachford in 700 autopsies, found an incidence of 3.8% of absent PCOAs [10]. De Silva does not encounter an absent PCOA in his studies involving 225 autopsies [14]. In the present series, incomplete circles resulting from absent PCOAs were found in 6% of the circles. Even though a relatively high incidence of absent PCOAs was encountered in the present study, on close observation, minute anastomosis between the filiform twigs arising from posterior cerebral and internal carotid arteries could be seen. Alpers et al., stated that in circles with absent PCOAs, on careful examination, a torn nubbin/fragile or filiform channels exists in the anticipated site of PCOA to perform the collateral circulation [1]. So it is probable that although the PCOA was absent anatomically, the collateral circulation was complete to certain extent and the function of PCOA was partially performed by this posterior communicating anastomosis. Partial duplications and plexiform PCOAs as described in the literature may probably belong to this group [14].
The present study in general, confirms the previous impressions of the difference between the anterior and the posterior half of the circle of Willis, in respect to the type of anomaly [1]. Most of the variations in the posterior half are either string-like vessels or persistent embryonic derivations of the PCAs from the internal carotids. The anomalies of the anterior circle are overwhelmingly those of accessory vessels, such as duplications or of triplications.
Many theories had been put forward to explain the variations of the circle of Willis. Lazorthes et al., stated that the variations in the caliber of the segments were due to amplitude of neck movements in the later years of life [24]. Fields stressed that all segments of the circle of Willis with its morphological variations and anomalies that play a role in post-natal life, have been developed prenatally. The genetic factors are very important, although random biochemical or physical factors could also be responsible [25]. Milenkovic et al., also observed that anomalies and variations of the circle of Willis are probably genetically determined and they develop in the early embryonic stage and persists into post-natal life [21]. Hillen stated that the variations of the circle of Willis are due to delicate hemodynamic tuning of all segments and that the relations between diameters of segments exist without reference to flow changes in the afferent arteries during neck movements [26]. Stehbens concluded that the topographical modifications of the circle occur during postnatal development of brain and with secondary modifications of collateral vessels in pathological occlusive disease [5]. Van Overbeeke et al., observed that the variations in posterior segments of the circle were due to developmental modifications with increased functional demands in connection with rapid growth of occipital lobes [27].
Cerebrovascular diseases such as stroke, aneurysms, internal carotid artery occlusion, unilateral flow restrictive external carotid artery disease together with their signs and symptoms grossly depend upon the variations of the anatomical pattern of circle of Willis. The main collateral blood flow in the circle is through communicating arteries and in symptomatic internal carotid artery occlusion, the blood flow through collateral pathways may be important in determining the severity of hemodynamic impairment [28]. The collateral ability of circle of Willis was assessed by Hoksbergen et al., by using Transcranial colour-coded duplex ultrasonography with common carotid artery compression tests in atherosclerotic patients with no cerebrovascular symptoms and concluded that the anterior collateral pathway (ACOA) of the circle was always functional while the posterior collateral pathway (PCOA) is nonfunctional in almost half of the hemispheres [2].
Rogers observed that the circle of Willis is not an equalizer and distributor of blood from different sources, there being no mingling of blood from different sources in the circle under normal circumstances. It functions as an anastomosis and offers a potential shunt under abnormal conditions such as might occur during an occlusion or spasm [29]. The state of the circle becomes important in determining the adequacy of the brain circulation. The possibility of bypass/shunts in occlusion of one of the cerebral vessels and the adequacy of recovery or lack of recovery after vascular occlusions may be explained in part by variations in the anatomy of the circle of Willis [14].
The association between anomalies of circle of Willis and cerebral aneurysms has been well documented [30]. A high incidence of anomalous circle of Willis has been reported in patients of saccular aneurysms of the intra cranial arteries [1,4]. Structural defects in the form of absence of tunica media in the vessel wall at or near the branching of a short segment of intra cranial arteries may cause berry aneurysms [4,5]. Perlmutter and Rhoton have stated that a malformation in structure, such as asymmetry of the anterior circle of Willis by producing local alterations in intravascular hemodynamics, may provide a mechanical basis for the development of aneurysms [22]. Kapoor et al., examined 1000 cadaveric brains and concluded that all aneurysms are located in the anterior half of the circle, at the junction of anterior cerebral and anterior communicating arteries [31]. Lazzaro et al., analysed 132 patients with ACOA and PCOA aneurysms and concluded that circle of Willis anomalies were commonly found associated with rupture of aneurysms and concluded that the presence of circle anomaly is an important criterion for selecting patients for preventive aneurysm treatment [32].
Blackburn studied the development of the encephalic arteries in 220 consecutive cases of mental diseases and concluded that there was evidence to show a decided predominance, in general, of anomalous circles among the mentally diseased [7]. He further analysed 400 cases of mental disease and found 42 instances of the azygos anterior cerebral arteries. This median/azygos ACAs has been found in all forms of mental diseases, possibly a little more frequently in cases of dementia and do not see any special relationship between the mental disease and the presence of this anomalous vessel [8]. Kamath stated that a higher percentage of anomalies of circle of Willis has been reported in the mentally ill patients and in patients with cerebrovascular catastrophy, thereby linking a possible connection of one being consequent of other [6]. These observations are only empirical assumptions and need further studies for definite evidence.
Cucchiara et al., analysed various anomalies of circle of Willis and its association with migraine and concluded that an incomplete circle was more commonly associated with migraine with aura patients than with control. They also further suggested that the variations of circle of Willis as a factor associated with migraine might be useful from a diagnostic perspective to classify migraine patients according to etiology and for selection of therapeutic strategies [33].
Conclusion
The anomalies of the circle of Willis play an important role in the occurrence, manifestation of symptoms, treatment options and recovery process of certain cerebrovascular disorders viz., stroke, and aneurysms. Variations were also found to be associated with migraine and mentally ill patients. The anomalies encountered include hypoplasia of the component vessels, duplications/triplications of anterior communicating arteries, triplicate anterior cerebral arteries, embryonic origin of posterior cerebral and the absent posterior communicating arteries. Hypoplasia and absent vessels were more prevalent in posterior circle, while accessory vessels were common in anterior portion of the circle. The neurosurgical importance lies during the exposure of the region for different purposes. A thorough knowledge of the vascular variants will increase the success of the procedure.