Composite Compound Odontoma-A Case Report
K.S. Kannan1, Ramachandra Prabhakar2, R. Saravanan3, Karthikeyan4, Rajvikram5
1 Professor and HOD, Department of Pedodontics, Thai Moogambigai Dental College, Chennai, India.
2 Professor, Dean & HOD, Department of Orthodontics, Thai Moogambigai Dental College, Chennai, India.
3 Professor, Thai Moogambigai Dental College, Chennai, India.
4 Professor, Thai Moogambigai Dental College, Chennai, India.
5 Reader, Thai Moogambigai Dental College, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ramachandra Prabakar, Professor, Dean & HOD, Department of Orthodontics, Thai Moogambigai Dental College, Chennai, India.
Phone: 9444468399,
E-mail: dr.ramachandra.prabhakar@gmail.com
Composite Compound Odontoma is a rare odontogenic tumour most commonly occuring in the anterior region of maxilla. An 11-year-old female patient reported a complaint of missing left central incisor. Clinical and diagnostic investigation revealed an odontogenic mass in the region of 21. This rare case report appraises the clinical diagnosis, surgical and orthodontic intervention which was planned and performed for its management.
Composite compound odontoma, Impacted incisors, Surgical exposure
Case Report
An 11-year-old female patient visited the Department of Pedodontics and Preventive Dentistry in Thai Moogambigai Dental College and Hospital, Chennai, India with the chief complaint of missing tooth in the upper left front region of jaw. The history revealed that the primary teeth had been retained for a longer period of 3 years. The extra-oral examination revealed no abnormalities such as incompetent or elevated lips. Intra oral examination disclosed an ill-defined, diffuse swelling associated with the attached gingiva of the left central incisor region. On palpation, the swelling was ovoid in shape, approximately 2 x 1 cm in size, extending from the labial frenum. It was bony hard and non-reducible, non-compressible and non-mobile. Radiographic examination revealed impacted 21 with evidence of swelling associated [Table/Fig-1 and 2].
The swelling is seen in the 21 region

The Ortho Pantanogram shows the lesion in 21 region
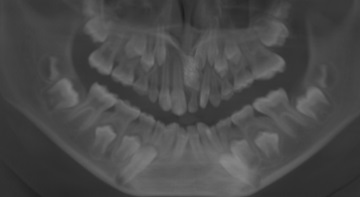
Clinical differential diagnosis included an Ameloblastic fibro-odontoma, Adenomatoid odontogenic tumor, Calcifying odontogenic cyst, Focal sclerosing osteitis, osteoma [1]. Routine hematological investigations revealed normal values. Orthopantomograph showed an ill defined mixed radiopaque radiolucent lesion in 21 region. The mixed radiopaque – radiolucent lesion, measured approximately 2.5 x 1.5 cm in size along with impacted incisor. IOPA is missing.
The radiographic differential diagnosis included odontoma, ameloblastic fibro-odontoma, and ameloblastic fibro - dentinoma.
On further CBCT (Cone Beam Computed Tomography ) examination 3D image had been obtained of the lesion and dimensions were approximated of the measurement of the OPG, showing an extraordinary view of the lesion in all the three axis. The CBCT gave a 3 Dimensional overview of the lesion thereby a precise surgical planning was accomplished [Table/Fig-3a and 3b].
This shows The CBCT images of the lesion with impacted incisors

The image was taken in frontal view and in dentition view to get a clear cut view of the lesion, its approximation of the impacted incisor to other teeth, the deciduous left central incisor and the alveolar crest, in relation to 21.
Surgical Procedure
Surgical removal of the odontoma under local anaesthesia was planned. A mucoperiosteal flap on the labial surface from the left lateral incisor to the right lateral incisor was reflected. The layer of bone overlying the labial surface was removed and the calcified mass was exposed. After excision of the lesion a number of calcified small structures looking like teeth were found in it and removed without disturbing the underlying tooth. A bracket was bonded to exposed left central incisor and ligated to facilitate the eruption of incisor. The remaining teeth were bonded with Brackets before the start of the surgery [Table/Fig-4 and 5].
The surgical Exposure of impacted incisor after the removal of the lesion

The excised Lesion with Denticles
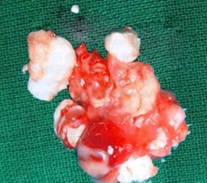
The specimen was sent for histopathological examination. Histopathological reports showed that the dentin appeared to have normal tubular pattern, strands of connective tissue and empty spaces of pulp chamber. These findings were suggestive of compound composite odontoma. The odontoma was excised, impacted incisor was exposed and bracket debonded for eruption. The remaining teeth were bonded with pre-adjusted edgewise brackets before the start of surgery.
It was seen in the CBCT that the tooth 21 had more than two third of root formation. It was noted during consecutive follow-ups that there was a significant change in its position. Patient was on regular follow-ups for more than a year and the permanent left central incisor was observed to move down along the path of eruption without any evidence of recurrence of the bony mass [Table/Fig-6].
The post operative photograph showing the erupted impacted incisor with PEA brackets

Discussion
Odontomas are comparitively common odontogenic lesions, generally asymptomatic [2]. They are rarely diagnosed before the second decade of life [3]. Here, the lesion was diagnosed in the patient’s 11th year. This lesion lead to impaction of the left central incisor which the composite compound odontoma frequently involved in [4]. Odontomas have been associated to trauma with inflammatory and infectious conditions, hereditary anomalies (Gardner’s syndrome, Hermann’s syndrome), odontoblastic hyperactivity and alterations in the genetic components responsible for controlling tooth development [5].
Compound odontomas are usually located in the anterior region of the maxilla, over the crowns of erupting teeth, or between the roots of erupted teeth [6]. Here the patient exhibited to have the lesion in the maxillary anterior region [3]. These lesions are usually unilocular and contain multiple radiopaque, miniature tooth-like structures known as denticles. Complex odontomas in turn are found in the posterior mandibular region, over impacted teeth, and can reach several centimeters in size [7].
Radiologically, these lesions manifest as a radiopaque solid mass with nodular elements occasionally, and surrounded by a fine radiotransparent zone. These lesions are unilocular and are differed from the normal bone by a well defined cortical bone formation [8]. Here the lesion was approximated with the help of CBCT which gave the cutting edge image of the lesion.
Clinically, these lesions often associated to alterations in permanent or temporary tooth eruption [9]. The diagnosis is usually established on occasion of routine radiological studies (panoramic and /or intraoral X-rays), but recently CBCT has played an important role in accurate diagnosis and identification of the lesion [10]. The treatment of choice is surgical removal of the odontoma, followed by histological analysis. Clinical experience and the dental literature illustrates that an individualized radiographic examination of any pediatric patient that presents clinical evidence of delayed permanent tooth eruption or temporary tooth displacement with or without a history of previous dental trauma, should be performed with at most recent diagnostic aid [4,11]. As demonstrated by this report, early diagnosis of odontomas with 3D imaging allows adoption of a less complex and less expensive treatment and ensures better prognosis [11]. A single CBCT imaging should proves preventive, i.e., preventing additional surgery and / or extended orthodontic treatment. In the case of odontomas associated to impacted teeth, the latter should be preserved in wait of spontaneous eruption, or alternatively fenestration followed by orthodontic traction is indicated [10].
If detected at earlier stages, interceptive treatment can be provided effectively enhancing esthetics, functions and structural balance in developing dentition [8]. Early removal of the cause of eruption disturbances is important in the developing dental arch. Compound odontomas are formed by tooth like structures which look like pulp tissue in the central portion surrounded by a dentin shell and partially covered by enamel [7]. Complex odontomas are conglomerates without orientation of dentin, enamel, enamel matrix, cementum, and areas of pulp tissue. The capsule of connective tissue that surrounds an odontoma is similar to the follicle that covers a normal tooth [7].
Conclusion
The advancement of diagnostic aids such as CBCT leads to a more efficient treatment planning for atraumatic excision of the lesion which was not possible with previous conventional radiographic methods. It is mandatory for every dental specialist to update and apply the advanced aids available.
[1]. Wood NK, Goaz PW, Lehnert J, Mixed radiolucent-radiopaque lesions associated with teeth. In: Wood NK, Goaz PW, editorsDifferential diagnosis of oral and maxillofacial lesions 1998 SingaporeHarcourt Brace & Company Asia Pvt Ltd:289-314. [Google Scholar]
[2]. Shafer Hine Levy A textbook of oral pathology 1993 fourth editionW.B. Saunders & Co.:308-12. [Google Scholar]
[3]. Khan Muslim, Din Qiam ud, Ishfaq Muhammad, ODONTOMES– A DESCRIPTIVE CASE SERIES ON 38 PATIENTSJKCD June 2011 Vol. 1(No. 2):91 [Google Scholar]
[4]. Philipsen HP, Reichart PA, Praetorius F, Mixed odontogenic tumours and odontomas. Considerations on interrelationship. Review of the literature and presentation of 134 new cases of odontomasOral Oncology 1997 33(2):86-99. [Google Scholar]
[5]. Slootweg PJ, An analysis of the interrelationship of the mixed odontogenic tumors- ameloblastic fibroma, ameloblastic-fibroodontoma, and the odontomasOral Surgery, Oral Medicine, Oral Pathology 1981 51:266-76. [Google Scholar]
[6]. Singh S, Singh M, Singh I, Khandelwal D, Compound Composite Odontome Associated with an unerupted deciduous incisor- a rarityJ. Ind. Soc. Ped. Prev. Dent vol 2005 23:146-50.Singh et al. [Google Scholar]
[7]. Or S, Yucetas S, Compound and complex odontomasInter J Oral Maxillofacial Surgery 1987 16:596-599. [Google Scholar]
[8]. Branca Heleisa de Oliveira, Vera Campos, Seira Marcal, Compound composite odontoma - diagnosis and treatment 3 Case ReportsPediatric Dentistry 2001 23(2):151-57. [Google Scholar]
[9]. Hitchin AD, The etiology of the calcified composite odontomaBrit Dent J 1971 130(11):475-82. [Google Scholar]
[10]. Anuraag B, Choudhary Mayur, Chaudhary B, Motwani Mukta B, Chaudhary Shweta M., Banode Pankaj J, UTILITY OF CONE BEAM CT IN MAXILLO-FACIAL RADIOLOGYInt J Dent, Case Reports 2013 3(1):134-45. [Google Scholar]
[11]. Olga Hidalgo Sánchez, Berrocal Ma Isabel Leco, González José Ma Martínez, Meta analysis of the epidemiology and clinical manifestations of odontomasMed Oral P Patol Oral Cir Bucal 2008 Nov 1 13(11):E730-4. [Google Scholar]