Early orthodontic interventions are often initiated in the developing dentition to promote favourable developmental changes. Interceptive orthodontic can eliminate or reduce the severity of a developing malocclusion, the complexity of orthodontic treatment, overall treatment time and cost. The safest way to prevent future malocclusions from tooth loss is to place a space maintainer that is effective and durable. An appropriate use of space maintainer is advocated to hold the space until the eruption of permanent teeth. This case report describes the various changing trends in use of space maintainers: conventional band and loop, prefabricated band with custom made loop and glass fibre reinforced composite resins as space maintainers.
Space maintainer, Prefabricated bands, Ribbond
Introduction
The primary dentition plays a very important role in the child’s growth and development, not only in terms of speech, chewing, appearance and the prevention of bad habits but also in the guidance and eruption of permanent teeth [1]. Exfoliation of primary teeth and eruption of permanent teeth is a normal physiological process [2]. When this normal process is disrupted, due to factors like premature loss of primary teeth, proximal carious lesions etc, it may lead to mesial migration of teeth resulting in loss of the arch length which may manifest as malocclusion in permanent dentition in the form of crowding, impaction of permanent teeth, supraeruption of opposing teeth etc [3]. The best way to avoid these problems is to preserve the primary teeth in the arch till their normal time of exfoliation is attained [4]. Hence it is rightly quoted that primary teeth serve as best space maintainers for permanent dentition.
However, if premature extraction or loss of tooth is unavoidable due to extensive caries or other reasons, the safest option to maintain arch space is by placing a space maintainer. The fixed space maintainers are usually indicated to maintain the space created by unilateral/bilateral premature loss of primary teeth in either of the arches. Of the various fixed space maintainers bBand and lLoop type of space maintainers are one of the most frequently used appliances [5].
Bands and loops are being has been used since long as a space maintainer with good high success rates Baroni et al., [6] Rajab [7]; Fathian et al., [8] but Inspite of good patient compliance, disintegration of cement, solder failure, caries formation along the margins of the band and long construction time are some of the disadvantages associated with them [4].
Considering this, there has been many pilot studies that explains the use of newer adhesive directly bonded splints eg: Glass fibre reinforced composite resins Ribbond [9], Everstick [10,11] as fixed space maintainers.
Ribbond is a biocompatible esthetic material made from high strength polyethylene fibres. The various advantages of this material includes its ease of adhesion to the dental contours, fast technique of application and good strength [12]. There are many options available to design various kinds of space maintainers. The case report describes various options as space maintainers.
Clinical Procedure
Patients in the age group ranging from 4-9 years who visited the outpatient were screened & the patients who either required extraction of the primary first/second molar or having pre-extracted primary 1st or 2nd molar in any of the arches were selected for the purpose of study. These patients were further screened on the basis of inclusion criteria.
The patients ranging from the age group of 4-9 years, in whom the extraction sites which had no space loss, erupting permanent tooth having adequate bone covering, fully erupted carieous free teeth, patients with dmf ≤ 4 were included in the study. Patients willing to participate in the study was selected & who were informed consent was taken.
A brief history was recorded and clinical examination was done. Intraoral periapical radiographs were taken in areas of tooth loss. Study models were prepared and space analysis was carried out for every child. For every selected child oral prophylaxis was done prior to the placement of space maintainer.
Case 1
GROUP I: (Conventional band and loop)
Group 1 consisted of extraction sites where conventional band and loop space maintainer was planned to be used.
Day 1 a) Fabrication of Band
Band was fabricated as follows:
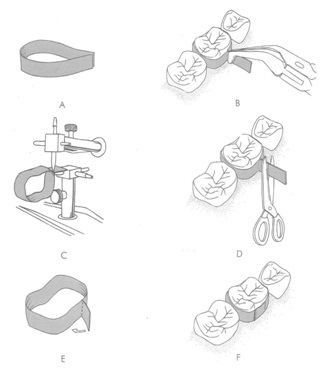
A 0.180×0.005 inch thickness of band material was taken and a ring was made [Table/Fig-1a]. This band material was seated in the patientspatient’s mouth with a band pusher & contoured with a Johnsons contouring plier and then a straight hoe was used to approximate the ends of ring [Table/Fig-1b]. This ring was then pinched as close to tooth surface as possible and then spot welded [Table/Fig-1c].This band was then seated in patient’s mouth and excess band material was cut off with band cutting scissors [Table/Fig-1d]. The remaining band material was adapted along the contours of band [Table/Fig-1e]. Band was then festooned and trimmed and ensured that the band covered the entire surface of tooth [Table/Fig-1f].
Impression was made with alginate, band was removed from the patientspatient’s mouth with a band removing plier and was stablised in impression and then it was poured in dental stone.
(a) Band material folded to form a ring (b) Approximating the ends of band (c) Spot welding (d) Excess band material is cut-off (e) Remaining band materials is adapted along with contours of band (f) Cemented band in place
Day 1 (b) Extraction of the involved tooth
The 1st or 2nd primary molars which were indicated for extractions because of furcal pathosis or cariously involved non-restorable tooth, were extracted under local anaesthesia. Extraction was performed under complete aseptic and sterile conditions & by applying the accurate exact principles of extraction.
Day 1 (c) Lab Procedure
The tooth extracted was then scrapped off from the cast and a loop was then made with a stainless steel 19 gauge wire using universal plier and it followed the contours of the gingiva. The loop spanned the edentulous area to contact abutment just below the contact point. The buccolingual width of the loop was such to permit the eruption of the cusps of the underlying permanent tooth. A silver solder was used to solder loop with the band at the middle one-third.
Cast was then immersed in water, the appliance removed from the cast & finished. The appliance was checked for any occlusal or gingival interferencesinterference prior to cementation.
Day 2 (a) Seating of appliance & cementation
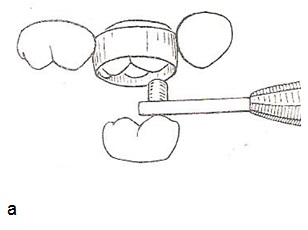
Oral prophylaxis was done, the abutment tooth was isolated with cotton rolls & then the appliance was cemented on the abutment tooth the using luting GIC [Table/Fig-2a,2b].

The applience was cemented on the abutement tooth the using luting GIC

Post-operative instructions
Patient was instructed not to eat or drink for 30 minutes and not to bite on any hard food. The patient was recalled after 3 months.
GROUP II (Prefabricated band with custom made loop)
Group II consisted of extraction sites where prefabricated band with custom made loop was planned to be used.
DAY 1: a) Selection of appropriate size of band & Impression taking
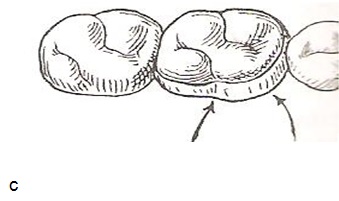
A prefabricated band was selected for the abutment tooth by measuring the mesiodistal diameter of abutment tooth with a caliper and then internal diameter of the prefabricated band was measured. The two were compared and the corresponding prefabricated band was then placed on the abutment tooth. The band was then seated onto the abutment tooth [Table/Fig-3 a]. Care was taken to keep margins sub-gingivally. [Table/Fig-3b]. Burnishing was done against the grooves and against the contours on the band [Table/Fig-3c]. The band was then festooned and ensured that it covered the entire surface of tooth.
Impressions were taken and poured in dental stone.
Seating of band by alternate pressure at line angles
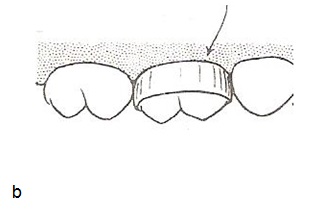
Burnishing into grooves and against contours
DAY 1(b): Extraction
The 1st or 2nd primary molars indicated for extraction were was then extracted as described above in Group 1
Day 1 (c) Lab Procedure
The extracted tooth was scrapped off from the cast and a loop was fabricated that contacted the tooth mesial it with, just below the contact point. It was then soldered with a silver solder in the middle one-third of band.
Day 2 (a): Seating of appliance & cementation
The cast immersed in water, appliance was removed from the cast and after finishing it was cemented on the abutment tooth as described in Group I [Table/Fig-4a, 4b].

Pre-fabricated Band with Custom Made Loop in Place

Post operative instructions
Patients were instructed not to eat or drink for 30 minutes and also not to bite on any hard food. They were recalled after 3 months.
GROUP III Woven polyethylene fibres (Ribbond)
Group III: This group consisted of extraction sites in which woven polyethylene fibres (RIBBOND) were placed as a space maintainer.
Day 1 (a) Extractions & impression:
Extraction was done as described in Group I and II. Impressions were taken and diagnostic casts were made. The amount of ribbond to be placed was measured with Vernier calliper [Table/Fig-5].
Measuring the sample site by vernier caliper

Day 2 a) Placement of Ribbond:
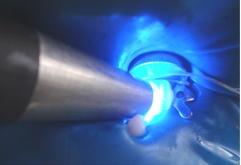
The abutments on which Ribbond was to be placed [Table/Fig-6a] were cleaned with pumice. The area was isolated with rubber dam [Table/Fig-6b], acid etched with 37% orthophosphoric acid [Table/Fig-6c] (3M), it is washed with water and then dried. The bonding agent (3M) was applied and cured for 10 seconds according to manufacturers instructions.
Site for Ribbond placement

Isolation with rubber dam (c) Acid etching


A thin layer of flowable composite (Flowline, Heraeus Kulzer Germany ) was applied on distal surface of the mesial tooth and on the mesial surface of the distal tooth of the created space without light curing where Ribbond was intended to be placed.
Ribbond was placed on the abutment teeth. After preliminary curing on both the teeth, additional restorative composite was further placed & cured for 40 seconds to completely bond the space maintainer with the abutment [Table/Fig-6 d,e].
Finished space maintainer

DAY 2 (b) Post-operative instructions:
The space maintainer was checked for any occlusal and gingival interferences [Table/Fig-6 f]. Finishing was done with composite finishing burs. Patient was instructed not to bite on any hard foods.
Occlusal view of ribbond space maintainer

Discussion
Conventional band and loop has long been used for maintaining space (Wright GZ, Kennedy DB)[5] but certain disadvantages like tendency for disintegration of cement, inability to prevent rotation or tipping of adjacent teeth, increased chair side and laboratory time make it a cumbersome procedure[13]. Introduction of prefabricated bands in a variety of sizes in November 1935[14] overcome these disadvantages with limitations being the same that indicates the need for newer designs and materials of appliance.
One such material is Glass fiber-reinforced composite resins (FRCRs) available to the pediatric dental market which can be used as an alternative to the conventional space maintainer [9]. Ribbond provides an excellent esthetic choice as a space maintainer. It is well tolerated by the patient, esthetic and less time consuming. However there is limited literature is available in terms of efficacy and longevity.
[1]. Barberia E, Lucavechi T, Free end Space Maintainers: Design Utilisation and AdvantagesJ Clin Pediatr Dent 2006, Fall 31(1):5-8. [Google Scholar]
[2]. Rao AK, Sarkar S, Changes in arch length following premature loss of deciduous molarsJ Indian Soc Pedo Prev Dent 1999; March :28-32. [Google Scholar]
[3]. http://depts.washington.edu/peddent/AtlasDemo/space009.html [Google Scholar]
[4]. Kirzioglu Z, Ozay MS Z, Ozay MS, Success of reinforced fibre material space maintainersJ Dent Child 2004 71(2):158-62. [Google Scholar]
[5]. Wright CZ, Kennedy DB, Space control in the primary and mixed dentitionsDent Clin North Am 1978 22:579-601. [Google Scholar]
[6]. Baroni C, Franchini A, Rimondini L, Survival of different typesof space maintainersPediatr Dent 1994 16:360-61. [Google Scholar]
[7]. Rajab LD, Clinical performance and survival of space maintainers: Evaluation over a period of 5 yearsJ Dent Child 2002 69:156-60. [Google Scholar]
[8]. Fathian M, Kennedy DB, Nouri MR, Laboratory made space maintainers a 7 years retrospective study from private pediatric dental practicePediat dentistry 2007 29(6):500-06. [Google Scholar]
[9]. Karman AI, Kir N, Four applications of reinforced fibre material in orthodontic practiceAm J Orthod Dentofacial Orthop 2002 121:650-54. [Google Scholar]
[10]. Kargul B, Caglar E, Kabalay U, Glass fibre reinforced composite resin as fixed space maintainer in children 12 month clinical follow upJ Dent Child 2005 72(3):109-12. [Google Scholar]
[11]. Kargul B, Çaglar E, Kabalay U, Glass fiber-reinforced composite resin space maintainer: case reportsJ Dent Child 2003 71:258-61. [Google Scholar]
[12]. Goldberg AJ, Frelich MA, Tooth splinting and stabilisationDent Clin North Am 1999 Mar 43(1):127-33. [Google Scholar]
[13]. Nayak UA, Louis J, Sajeev R, Peter J, Band and loop space maintainer made easyJ Ind Soc Pedo Prev Dent 2004 22(3):134-36. [Google Scholar]
[14]. Ricketts RM, Bioprogressive therapy as an answer to orthodontic needs part IAm J Orthod Dentofacial Orthop 1976 70(3):241-68. [Google Scholar]