Residual ridge resorption has been considered as an inevitable consequence after extraction of the teeth. There is a gradual loss of the alveolar bone due to the pattern of bone remodeling. In spite of the availability of newer treatment modalities like endodontic restoration and periodontic procedures for preservation of the remaining teeth they are not feasible for the patients in severe stages where restoration might not be possible. The only reliable method of preserving the remaining bone is by maintaining the functional health of the teeth. Over the years, many studies showed that roots which are fractured and left behind during extractions are retained into the alveolar bone with no evidence of pathosis. Over denture as a treatment option was developed in an effort to preserve the remaining alveolar bone by retaining the natural teeth or roots. In over denture treatment, the teeth selected as abutments are prone to caries and periodontal disease over a period of time, hence evolved the vital or non vital root submergence concept. After a thorough radiographic and clinical examination, few teeth without pathosis are retained that eventually are surgically submerged in the alveolar ridge. After healing, the over denture with reaining vital or non vital teeth preserve the integrity of the bone, making the treatment an effective and successfull preventive prosthodontic treatment.
Case Report 1
Vital submerged root
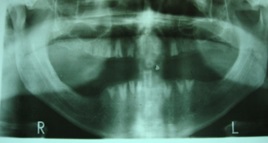
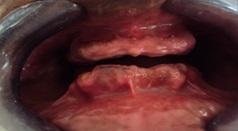
A 46-year-old male patient reported to the department of Prosthodontics for replacement of the missing teeth [Table/Fig-1]. In order to select the patient for root submergence treatment medical history, dental history and history of habits was noted, clinical examination, both intra–oral and extra–oral was done. For thorough examination OPG was advised [Table/Fig-2]. It was seen that there were multiple decayed teeth which cannot be restored and many teeth were missing. Teeth 11,21,22,31 were extracted due to caries. With the remaining teeth that cannot be used as abutments for fixed prosthetic treatment, it was decided that root submergence could be the choice of treatment. The patient was informed about root submergence method of treatment, its advantages and disadvantages. With the patients consent vital root submergence treatment was selected.
Pre-operative clinical photograph

Pre-operative panoramic view

Further evaluation was done after a healing period of one month. In the vital submergence technique, as the vitality of the root has to be maintained, the teeth indicated for submergence were treated as atraumatically as possible. The vital root submergence procedure was carried by reflecting the full thickness flap. The coronal part of the teeth selected for vital submergence (13,14,23,33,34,35,41,42,43,44) was reduced to 2 mm below the alveolar crest using a chisel and a mallet slowly such that the vitality of the tooth is not effected [Table/Fig-3]. Once the tooth was sectioned 2mm below the alveolar crest, the irregular / sharp surface of the sectioned teeth and surrounding bony irregularities were smoothened using a round bur and straight hand piece under copious irrigation ensuring well rounded and smooth edges to the hard tissue. Using a bone file, the interdental bone is smoothened. The flap is then approximated to evaluate for complete closure.
Surgical Procedures for vital Submergence of roots

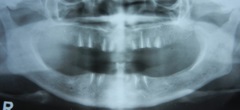
The flap was sutured and primary closure was obtained [Table/Fig-4]. Patient was recalled after 7 days for suture removal. After satisfactory healing an assessment of the intra arch space available was recorded [Table/Fig-5]. The Interarch space was 18mm for this patient, which was sufficient for fabrication of a complete over denture prosthesis supported by the underlying vital submerged roots. The over denture was fabricated in the conventional method by making the preliminary impressions followed by border molding using a special tray with full spacer such that relief was given to the entire alveolar ridge with submerged roots. Light body polyvinlysiloxane was used for the wash impression so that accurate details were recorded. Jaw relations were recorded followed by face bow transfer using Hanau spring bow. Gothic arch tracing followed by centric and protrusive records were obtained for programming the Hanau wide vue Arcon 183-2 articulator, for balanced occlusion. Teeth arrangement was done in the neutral zone so that the forces laid by the denture are well distributed on all the remaining hard tissues such that further resorption of the residual ridge is reduced and clinical exposure of the retained roots is prevented. During Try-in, proper occlusion was ensured and the fabricated denture was lab remounted. All the occlusal corrections were done and after ensuring proper occlusion, denture was delivered to the patient. Post-insertion instructions were given to the patient with emphasis on maintenance of the denture. Patient was recalled after 6 months and OPG was taken. Radiographic examination revealed complete tissue coverage [Table/Fig-6]. Most of the retained vital roots appeared normal.
Sutures Placed Post Surgically


Six months post operative
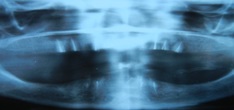
After a period of 1 year the patient was reevaluated [Table/Fig-7]. Radiograph revealed periapical pathology in 35,43 [Table/Fig-8] with clinical exposure of the submerged roots, Apart from those two teeth all the remaining teeth were in sound health. The two teeth were extracted and further evaluation of the patient was done after 1 month. Radiographs did not show any pathology, the alveolar bone was well formed and the healing was satisfactory. Patient did not complain of ill fitting prosthesis even after extraction of the infected teeth. Phonetics and esthetics were evaluated and patient reported complete satisfaction.
Panoramic view one year post operative

One year post operative showing exposure
Case Report 2
Non–vital submerged roots
A 56-year-old female patient reported to the department of Prosthodontics complaining of ill fitting upper and lower anterior fixed prosthesis. The ill fitting prosthesis was removed [Table/Fig-9] and OPG was advised; Medical history, dental history and history of habits was noted; clinical examination, both intra-oral and extra-oral was done. Examination of the radiograph revealed several missing teeth (11,21,31,35,36,37,41,42,45,46,47) [Table/Fig-10] and inadequate bone support for maxillary posterior teeth. Patient did not report of any medical history like diabetes or hypertension. As there was minimal crown portion of the tooth, which cannot be taken as abutment for fixed prosthesis, it was decided to retain the roots which were not infected hence non-vital root submergence treatment was planned for the patient. The patient was informed about the non-vital root submergence method of treatment, its advantages and disadvantages. With the patients informed consent, While presenting the case to patient it was decided that few teeth will be (13,16,17,26,27) extracted followed by root canal treatment for all the remaining (14,15,23,24,25,32,33,34,43,44) teeth.
Pre–operative clinical presentation

Pre–operative panoramic view

After the extraction and endodontic treatment of the indicated teeth was complete, patient was called for a review after one month. An OPG was then taken to evaluate the condition of the remaining teeth. The radiograph did not show any pathology and the remaining teeth which were endodontically treated were in sound periodontal health.
The non-vital root submergence was done by reflecting the periosteal flap [Table/Fig-11], using a straight fissure carbide bur and a hand piece under copious irrigation; the teeth were horizontally sectioned till the crest of the ridge. Later using a round bur the teeth were sectioned 2 mm below the crest of the alveolar ridge. The Guttapercha was burnished with a ball burnisher and remnants of the tooth and gutta-percha were washed with saline. The uneven surfaces of the interdental bone were smoothened using a bone file. Smooth and rounded surfaces were ensured. Later the flap was approximated to ensure close proximity and the flap was sutured with tight closure. After 7 days the sutures were removed and healing was evaluated. After satisfactory healing period of one month, the intra arch space was recorded as 17 mm. Non–vital submerged root supported complete over denture was fabricated in the conventional method starting with preliminary impressions, border molding and final impression, jaw relations, face bow transfer, gothic arch tracing, centric and protrusive records to obtain a balanced occlusion. Try in was done where teeth were arranged in neutral zone so that the forces acting on the alveolar bone are well distributed. The fabricated denture was delivered to the patient [Table/Fig-12]. Patient was educated about the maintenance and post insertion care. After 3 months the patient was reevaluated and OPG was examined which did not reveal any periapical pathology [Table/Fig-13]. The patient was called for further evaluation after 1 year, an OPG was taken and it revealed no periapical pathology. The crestal bone did not show any changes and there was no clinical exposure of the submerged roots [Table/Fig-14]. The patient was satisfied with the over dentures.
Surgical procedure for non vital Submergence of root

Clinical presentation after healing

Panoramic view after three months
Panoramic view after one year
Discussion
Preserving the remaining bone can be achieved by maintaining the functional health of the teeth [1]. In over denture treatment, the abutment teeth are prone to caries and periodontal disease hence evolved the vital or non vital root submergence concept [2]. After a thorough radiographic and clinical examination, teeth are submerged in the alveolar ridge making it a preventive Prosthodontic treatment [3]. The vital and non vital root submergence treatment is of importance in the aged, the handicapped and those with little or poor oral health maintenance [4]. The use of retained roots in over denture reduces loss of alveolar bone and increases stability of the over denture [5]. There are many advantages of this treatment like; Preservation of the alveolar bone which enhances the retention of dentures. Vertical dimension of occlusion is maintained. The Average tactile perception to load for denture wearers was 10 times that of natural teeth. This treatment is Advantageous than over dentures with attachments, as presence of attachments decreases the intra arch space making teeth arrangement difficult. In this method, there is no criterion for preservation of teeth unlike conventional over dentures where the configuration or location of the teeth has to be considered. Hence, any number of teeth can be preserved. It is comparatively inexpensive and maintenance procedure like application of fluoride on the remaining natural teeth is not required as in conventional over denture treatment [6].
The vital and non vital root submergence treatment also has a few disadvantages like development of periapical pathology mostly in case of vital retained roots; this is a surgical procedure which at times may not be advised depending on the systemic health of the patient.
Clinical exposure of the submerged roots is also noticed in few cases; future extraction of the retained roots may cause instability of the denture. Patient may have a stretched appearance of the lips due to the preservation of the bone over which the denture flange lies. There is also possible loss of vestibular depth due to surgery.
In 1959, Simpson examined a number of retained roots in humans and suggested that root fragments, which were originally unaffected, could be safely left in position [7,8]. Preserving the teeth or the roots preserves the periodontal ligament [9]. The first published report of intentional root submersion was by Bjorn in 1961 [9]. In 1970, Howell reported a clinical study of submerged endodontically treated roots, some of which had been under observation for more than 10 years [10]. In 1973, Herd reported on 228 retained roots from 171 patients [11]. He found that 163 of these roots had vital pulp tissue with no inflammation. Howell’s purpose was an attempt to preserve alveolar bone. He claimed there was no apparent loss of bone in this long-term study and appears to be the first to utilize this technique for bone preservation under complete dentures. In 1973, Sander discussed the advantages of root retention for the maintenance of alveolar bone. He cited the main disadvantage of root submersion was the reduction in height of the vestibule [12].
In 1977 Cook et al., Performed a study similar to Bjorn’s 1965 study, except that the submerged teeth were vital. Pulpal tissues associated with submerged roots appeared vital without significant degeneration or inflammation. In 1978 Welker and associates reported on 12 roots submerged in six patients. Eight were vital and four non–vital. Dentures had been worn over the roots for periods up to 51 months [13]. All patients had been termed clinically successful.
Atwood observed that the reduction of residual ridges needs to be recognized as a major unsolved oral disease causing physical, psychological and economical problems to many people. Both objective and subjective findings clearly indicate the significant benefits of the tooth retention since the extraction of few remaining teeth is a serious decision [14]. Alveolar bone maintenance depends on the presence of healthy roots and periodontal ligament which transmit functional forces to the surrounding bone [15]. Denture pressure on a residual ridge also results in bone resorption. The technique of tooth root retention under complete dentures appears to militate against such a force application. The evaluation of individual teeth for the presence or absence of pulpal involvement is essential in the success of root submergence.
Proper diagnosis and endodontic treatment of submucosally retained roots lead to an excellent tissue acceptance and ridge preservation. Three-month follow-up revealed excellent healing of soft tissues. The oral tissues appeared normal in color and texture, and the denture remained stable and retentive. The patient reported favorable denture experience [16]. Clinical examination revealed no further reduction of the residual ridge in the region of retained roots. One factor of major concern in this mode of treatment was that there was decreased vestibular depth and also the intra arch space was limited as the teeth were preserved [17]. As the retained roots preserved, undercuts were formed which make the path of insertion and removal of the prosthesis difficult for the patient [18]. The underlying teeth also increased the fullness of the lip in the facial surface giving the lips a stretched appearance; in order to avoid this denture has to be relived in these areas at times soft liners were also used for the ease of removal and placement of the prosthesis.
Conclusion
Mucosal coverage of roots as a means of preserving the residual alveolar ridge is a sound clinical method for those patients where the entire tooth or teeth cannot be preserved. When a comparison was done between the vital and non-vital submerged root procedure, vital root retention had more problems like periapical pathology of the root and pain sensation by the patient, hence the non vital root submergence method was an advisable option compared to the vital root submergence. Both the treatment methods have certain drawbacks like poor esthetics of the prosthesis as it gives a stretched appearance of the lips. Hence, by this method of treatment the phonetics and the functionality of the patient were well preserved with a little compromised esthetics. The undisturbed root attached to the alveolar bone by the periodontal ligament is the “perfect” implant, and by this method of treatment, many teeth as possible can be preserved in turn preserving the alveolar bone integrity.
[1]. Sharma Anil, Submergence of vital roots for the preservation of residual ridges: A clinical studyOral health and preventive dentistry 2012 10:259-65. [Google Scholar]
[2]. Hiremath Hemalatha Parmeshwar, Endodontic Treatment in Submerged Roots: A Case ReportDent Res Dent Clin Dent Prospect 2010 4(2):64-68. [Google Scholar]
[3]. Kumar J. Srinivas, A Preliminary Report On Over Denture Retained By Submerged Vital RootsInd J Dent Sci 2010 1(1):38-40. [Google Scholar]
[4]. Salma Maurice, Advantages of root submergence technique for the pontic site development in esthetic implant therapyInt J periodontics restorative dent 2007 27:521-27. [Google Scholar]
[5]. Miller P. A., Complete Dentures Supported By Natural TeethJ Prosthet Dent 1959 8:924-28. [Google Scholar]
[6]. Graver Don G, Vital Root Retention in Humans: A Preliminary ReportThe Journal of Prosthetic Dentistry 1978 40(1):23-28. [Google Scholar]
[7]. Morrow RM, Tooth-Supported Complete Dentures: An Approach to Preventive ProsthodonticsJ Prosthet Dent 1969 21:513-522. [Google Scholar]
[8]. Odge CA, Prevention of Complete Denture Problems by the Use of over denturesJ Prosthet Dent 1973 30:403-11. [Google Scholar]
[9]. Thayer HH, Over dentures And the PeriodontiumDCNA 1980 24:369-377. [Google Scholar]
[10]. Derkson GD, Macentee MM, Effect of 0.4% Stannous Fluoride Gel on the Gingival Health of Overdentures AbutmentsJ Prosthet Dent 1982 48:23-26. [Google Scholar]
[11]. Toolson LB, Smith DE, A Five-Year Longitudinal Study of Patients Treated with over denturesJ Prosthet Dent 1983 49:749-56. [Google Scholar]
[12]. Ullo CA, Renner RP, Design Considerations for a Removable Partial OverdenturesCompend Contin Educ Dent 1984 5:15-19. [Google Scholar]
[13]. Casey DM, Lauciello. A, Review of the Submerged Root ConceptJ Prosthet Dent 1980 43:128-32. [Google Scholar]
[14]. Carver DG, Fenster RK, Baker R, Johnson DL, Anti Vital root retention in humans: A preliminary reportJ Prosthet Dent 1978 40:23 [Google Scholar]
[15]. Johnson D. I., Kelly. J. F., Flinton. K., Cornell M.T., Histological evaluation of vital root retentionJ Oral surgery 1974 32:829 [Google Scholar]
[16]. Brewer AA, Morrow R, Overdentures 1975 St LouisThe C. Mosby Co.chap 1 [Google Scholar]
[17]. Guyer SE, Selectively retained vital roots for partial support of over dentures. A patient reportJ. Prothed. Dent 1974 33:258 [Google Scholar]
[18]. Crum RJ, Loisscllc RJ, The stud attachment overlay denture and proprioceptionJ. Am. Dent. Asscc 1971 82:583 [Google Scholar]