Multidisciplinary Approach to the Rehabilitation in Management of Child with Early Childhood Caries: A Case Report
Neeraj Sharma1, Sidhi Passi2, Vinay V. Kumar3
1 Senior Assistant Professor, Department of Oral Medicine and Radiology Dr. HSJ Institute of Dental Sciences Panjab UniversityChandigarh, Punjab, India.
2 Senior Assistant Professor, Department of Pedodontia Dr. HSJ Institute of Dental Sciences Panjab UniversityChandigarh, Punjab, India.
3 Senior Lecturer, Swami Devi Dyal Hospital and Dental CollegeBarwala Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sidhi Passi, Assistant Professor, Department of Pedodontia, Dr. HSJ Institute of Dental Sciences Punjab University Chandigarh, Punjab, India.
E-mail: sidhi.passi@gmail.com
The aesthetic requirement of severely mutilated primary anterior teeth in case of Early Childhood Caries (ECC) has been a challenge to paediatric dentists. ECC involves the upper anterior teeth early in life and by the time the dentist sees the child, most of the coronal structure is lost. This article presents the clinical sequence of rehabilitation of maxillary anterior primary teeth, and the mandibular posterior teeth.
Early childhood caries, Aesthetics, Hybrid composite, Polyethylene fibre
Case Report
A problem which is commonly faced in paediatric clinics is the restoration of these primary maxillary incisors which are destroyed by trauma or caries. Most of the cases are children with nursing bottle caries [1, 2]. In early childhood caries, there is early carious involvement of the maxillary anterior teeth [3]. The early loss of primary anterior teeth may result in a reduced masticatory efficiency, loss of vertical dimension, development of parafunctional habits (tongue thrusting and speech problems), aesthetic-functional problems such as malocclusion and space loss, and psychological problems that can interfere in the personality and behavioural development of the child [4]. With the introduction of new adhesive systems and restorative materials, a new approach for treating these teeth has been explained and documented for clinical cases, where fibre core posts are introduced into the root canals of primary incisors for a distance of 2 to 3 mm. Adhesive restorations allow clinicians to create minimally invasive preparations, thereby preserving sound tooth structure [5].
A 5-year–old male patient reported to the Department of Pedodontics and Preventive Dentistry, with chief complaints of pain in the lower posterior region and decayed upper front teeth [Table/Fig-1]. On intra-oral examination, a complete set of deciduous teeth was found .52, 62 and 54 were found to be carious, while IOPA revealed the pulpal involvement of 51, 61 and 84. Seventy four was found to be grossly decayed and it was extracted, followed by the placement of a band and a loop space maintainer [Table/Fig-2]. An endodontic treatment was carried out for 51, 61 and 84. For 84, it was followed by the placement of a stainless steel crown [Table/Fig-3], while for 51and 61, a pulpectomy was done and the cervical third of each tooth was prepared for the placement of an intra canal retainer i.e. a polyethylene fibre (Ribbond) – of 4 mm thickness.
Preoperative intra oral photograph of the patient

Band and loop space maintainer after extraction of 74

Stainless steel crown on 84

The treatment plan was divided into 2 steps for 51 and 61:
Step 1: The Endodontic Phase
Labial and palatal infiltrations were carried out for 51and 61, the pulp chamber was opened and working length was determined. The pulp tissue was extirpated by using no.15 – no.35 K-files. After irrigation with copious amounts of 2.5% sodium hypochlorite and normal saline, the root canal was dried by using paper points. A thick mix of Endofloss paste was then condensed with lentulo-spiral into the canal [Table/Fig-4].
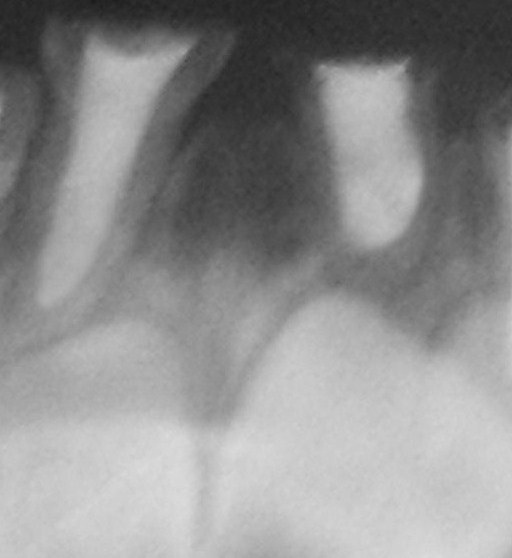
IOPA showing obturation of 51 and 61
Step 2: Construction of the Restoration
The post–space was prepared 1 week after the endodontic treatment was completed. The post–space was created by removing approximately 4mm of Endofloss material by using a thin straight fissure bur. All visible Endofloss cement on the walls of the post –space was removed.
The prepared post space was then cleaned with saline, air-dried and acid – etched with 37% phosphoric acid for 15 seconds. This space was rinsed and air dried and after that, a light cured bonding agent was applied. It was then light cured with for 20 seconds. The polyethylene post was then cured for 20 seconds in order for it to gain rigidity, before its insertion into the post–space. The necessary length of tape for each dental element was achieved and the fibre was cut to approximately twice the height of coronary core restoration. The fibre was inserted into the canal [Table/Fig-5] after it was immersed in the dental adhesives system (scotch bond, 3m), along with a thin layer of flowable composite. A visible light curing was done and finally, teeth were restored with hybrid composite [Table/Fig-6].
Polyethylene fiber post inserted

Post operative photograph of the patient

Discussion
Restoration of primary anterior teeth that have been grossly destructed by caries is very challenging for paediatric dentists. When there is severe loss of coronal tooth structure, the use of posts which are placed inside the canal after endodontic treatment will give retention, provide stability to the reconstructed crown, and withstand masticatory forces in function. A variety of root posts are used in paediatric dentistry. Prefabricated posts are fast, cheap and easy to use, but they do not take into account the individual shape of the root canal. Although metal posts are indicated for primary teeth, because of their colour, metal posts do not meet the aesthetic requirements. Composite posts provide satisfactory aesthetics; however, there is a risk of loss of retention, owing to polymerization shrinkage [6]. Different fibre types such as glass fibres, carbon fibres, Kevlar fibres and polyethylene fibres are added to composite materials. Carbon fibres prevent fatigue fracture and strengthen composite materials, but they have a dark colour, which is undesirable aesthetically. Kevlar fibres which are made of an aromatic polyamide, increase the impact strength of composites, but they are unaesthetic and hence, their use is limited.
One of the latest techniques which are used to restore these teeth, as has been described in this paper, is the use of polyethylene fibres (Ribbond). Ribbond has adequate translucency , ease of manipulation, a decreased chair side time, etc. Polyethylene fibres improve the impact strength, modulus of elasticity and flexural strength of composite materials and they are almost invisible in the resinous matrix. Due to these reasons, they are the most appropriate and the best aesthetic strengtheners of composite materials.
The treatment which has been described in this case report, about the use of Polyethylene fibres, is simple and effective and it represents a promising alternative for rehabilitation of grossly destructed or fractured primary anterior teeth.
[1]. Johnsen DC, Characteristics and background of children with “nursing caries”Paediatr Dent 1982 4:218-24. [Google Scholar]
[2]. Yui CK, Wei SH, Management of rampant caries in childrenQuintessence Int 1992 23:159-68. [Google Scholar]
[3]. McDonald Avery Dean Dental caries in the child and adolescent 2005 8th editionMosby:209-10. [Google Scholar]
[4]. Rocha Rrachel de Oliveira, Neves Lucimara Teixrira das, Marotti Noely Regina, Wanderley Marica Turolla, Correa Maria Salete Nahas Pires, Intracanal reinforcement fiber in pediatric dentistry: A case reportQuintessence International 2004 35:263-68. [Google Scholar]
[5]. Mannocci F, Berteli E, Sherriff M, Watson TF, Ford P, Three-year clinical comparison of survival of endodontically treated teeth restored with either full cast coverage or with direct composite restorationJ Prosthet Dent 2002 88:297-301. [Google Scholar]
[6]. Uzun G, Hersek N, Tincer T, Effect of five woven reinforcements on the impact and transverse strength of a denture base resinJ. Prosthet Dent 1999 81:616-20. [Google Scholar]