The relationships between a fixed partial denture (FPD) and the surrounding hard and soft tissue should be considered crucial for long-term success. An FPD requires an accurate impression that records location of the finish line of the prepared tooth and a portion of apical uncut tooth structure. This is important so that the restoration has a suitable emergence profile with well-adapted and smooth gingival margins [1]. Accurate adaptation of crown to finish line is essential to minimize cement dissolution & to preserve periodontium in fixed partial denture cases. Accurate adaptation of crown is possible only when preparation details are captured adequately in the impression & transferred to cast. For these reasons, gingival displacement is necessary to capture sub-gingival preparation details [2,3].
Gingival retraction is needed for adequate lateral displacement of gingiva, for adequate flow of low viscosity impression material into the sulcus and for accurate capturing of prepared finish line and a portion of apical uncut tooth structure [4,5]. Gingival retraction is also helpful during cementation for easy removal of excess cement without tissue damage and also in assessing the marginal fit and caries if present. Apart from this gingival retraction is also needed to extend the restoration below the gingival margin to enhance retention [6].
Various methods of tissue management such as mechanical methods, mechanico chemical methods, electro surgery, rotary gingival curettage, or gingitage have been described. Several studies reported gingival damage associated with traditional techniques, but other investigators documented complete gingival healing after gingival retraction without permanent damage to soft tissues [1].
Numerous studies reported mechanical methods that involved the use of strings or fibers of different types and diameters to be the most effective, safe and easy methods for tissue displacement. [7,8,4,9]. The cords were placed either by single cord or double cord technique out of which the double cord technique was found to be more effective.
A new retraction material (Merocel, Merocel Co., Mystic, Conn.) was recently proposed for dentistry to displace gingival tissue without tissue damage before impression making. Merocel retraction strips are a synthetic material that is specifically and chemically extracted from a biocompatible polymer (hydroxylate polyvinyl acetate) that creates a netlike strip without debris or free fragments [1,5].
Merocel retraction material is (1) chemically pure, (2) easily shaped, (3) remarkably effective for absorption of intraoral fluids such as blood, saliva, and crevicular fluid, (4) soft and adaptable to the surrounding tissues, (5) free of fragments, without debris, and (6) not abrasive [8].
Merocel retraction material was selected because it is an absorbing, haemostatic material commonly used in otorhinolaryngic, gastric, thoracic, and otoneurosurgical procedures [1]. This study compared the effective gingival displacement produced by Merocel strips and the conventional retraction cord used with double cord technique [5].
This observational, comparative study aimed to determine whether the polyvinyl acetate strips are able to effectively displace the gingival tissues in comparison with the conventional retraction cords.
The key objectives of this study includes to determine the amount of gingival retraction produced by cord; the amount of gingival retraction produced by the strip; to compare the amount of retraction produced by strip with the cord and to evaluate gingival health in both the groups after two weeks.
Material and Methods
After signing an informed consent form, ten patients in good general health were selected for this clinical investigation. Fourteen teeth (maxillary anterior) were selected. The age of patients ranged from 20 to 40 years. All patients were selected with the following criteria:
Inclusion criteria
Subjects with:
Not less than 18 years of age.
Preparation needed for full coverage restoration.
Sound gingival and periodontal health of the abutment teeth.
Abutment teeth of normal size and contour (no developmental anomaly or regressive age changes).
Abutment teeth selected in maxillary anteriors.
Exclusion criteria
Subjects with:
Tipped, tilted or rotated abutment teeth.
Any kind of Gingival pathology
Armamentarium
Mouth mirror, periodontal probe (William’s), and tweezers.
Surgical gloves, mouth mask.
Cotton rolls.
Dappen dish.
Scissors - straight and angled.
Cord packer (Hu-Friedy,USA).
Knitted retraction cord (Ultrapak, Ultradent,USA)
Polyvinyl acetate strips (Merocel, Mystic, Conn) [Table/Fig-1]
Cheek retractor.
Digital vernier caliper (Digimatic caliper, Mitutoyo, Japan) [Table/Fig-2].
Polyvinyl acetate strips (Merocel, Mystic,Conn)

Digital vernier caliper (Digimatic Caliper, Mitutoyo, Japan) 0.01mm accuracy

Materials
Retraction systems used in this study were
Polyvinyl acetate strips (Merocel, Mystic, Conn).
Plain retraction cord (Ultrapak, Ultradent, USA).
Methodology
The study was done using two groups, the same patients served for both the groups. In one group (Group A) the retraction was done using the retraction cord (Ultrapak, Ultradent, USA) and after a two week time interval the other material Merocel (Mystic, Conn) was tested. In the other group (Group B) the order of retraction material used was reversed. This was done to find the effect of the material in gingival health in a two week follow up.
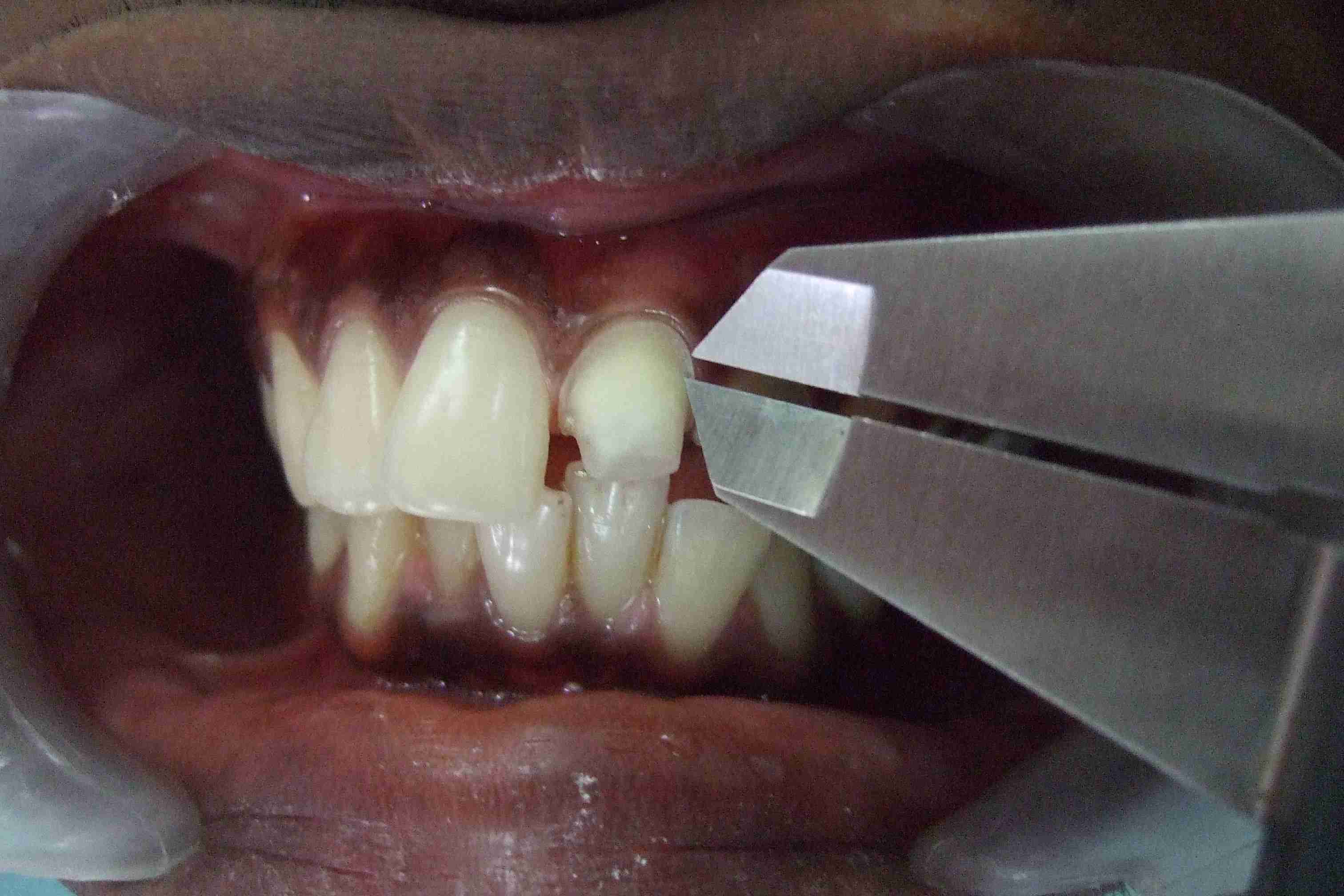
For the clinical procedure, the tooth was prepared with a supra-gingival level without retraction of the gingival sulcus. Clinical measurements were initially recorded immediately before retraction on the buccal and palatal aspect at three points on each side that coincided with the mesial line angle, distal line angle [Table/Fig-3] and at the deepest point on the preparation to the crest of the free gingival margin. The measurement was recorded linear from the prepared finish line to the free gingival margin using digital vernier caliper (Digimatic caliper, Mitutoyo, Japan) of 0.01mm accuracy.
Measuring at Disto-buccal line angle
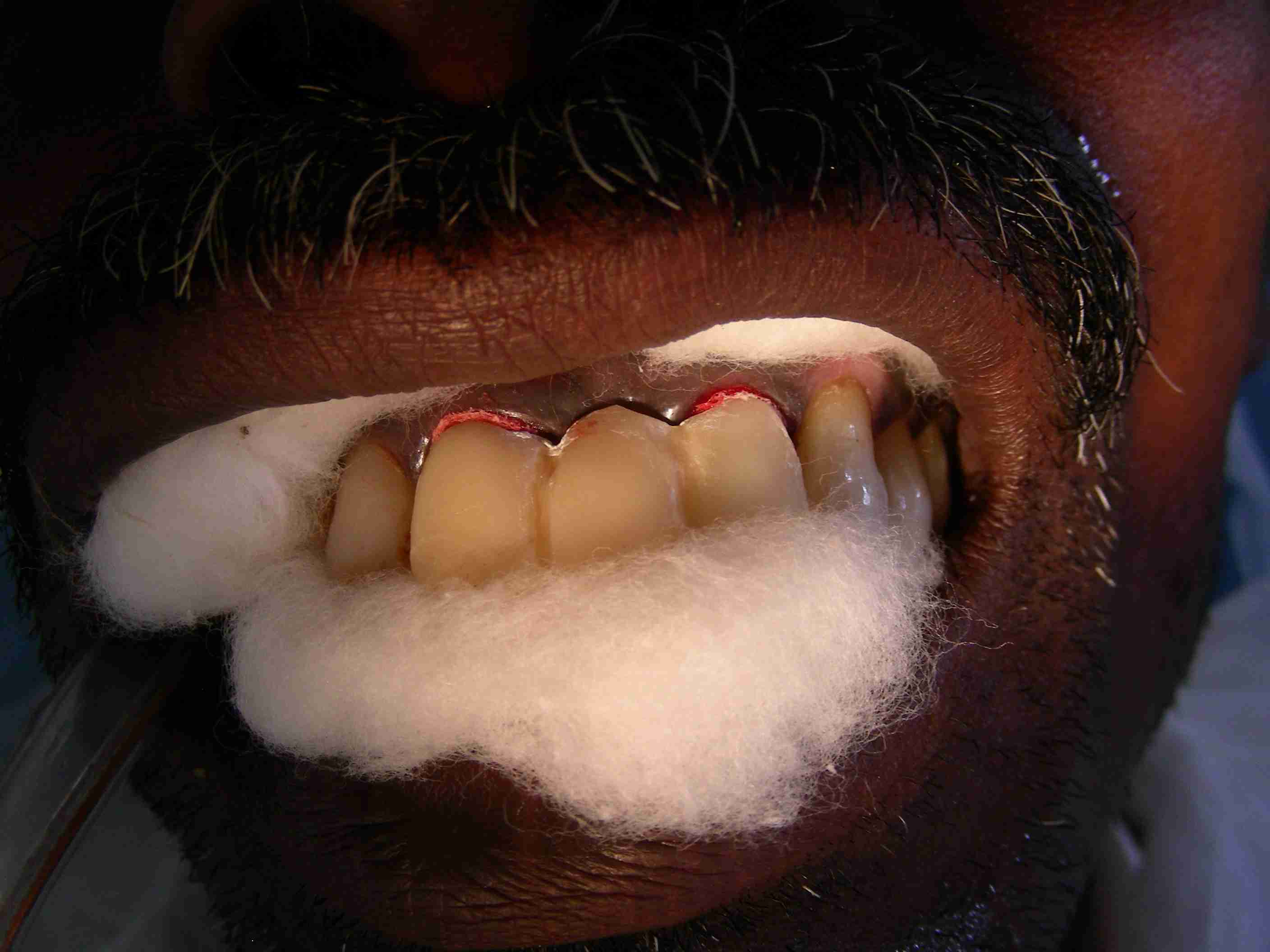
A 2 mm thick Merocel retraction strip was inserted around the tooth using cord packer (Hu-Friedy, USA) and the provisional crown inserted. The patient was asked to maintain pressure on the artificial crown and concomitantly on the Merocel strip with the use of a cotton roll [Table/Fig-4]. This position was sustained for 10 minutes. The Merocel retraction strips tended to expand with absorption of selected oral fluids, exerting pressure on surrounding tissues to provide gingival retraction [Table/Fig-5]. The materials in the intracrevicular space were removed and the measurements repeated.
Merocel strips in gingival sulcus secured with temporary acrylic FPD
After retraction with Merocel strip

After two weeks the retraction was done using conventional plain retraction cords, which were packed dry into the sulcus without any chemicals using double cord technique. The measurements were recorded as before. All the measurements were done by a single operator.
Statistical Analysis
Mean and standard deviation were estimated from the sample for each study group. Mean values were compared between different study groups by paired samples students t-test. In the present study, p<0.05 was considered as the level of significance.
Results
The collected data were analysed using paired sample t-test to test the characteristics of the data. p<0.05 indicates significant difference between the variables.
The data were analysed for the following; the before retraction and after retraction values of cord [Table/Fig-6] and strip [Table/Fig-7] were analyzed respectively. After retraction values of the cord and strip were compared [Table/Fig-8]. Before retraction values of both the groups were compared patient wise [Table/Fig-9] to know its effect on the health of the gingival tissues in a two week interval.
Comparison of before and after retraction mean values with Cord
| Groups | n | Mean | Std. Deviation | t-value | p value |
|---|
| Before | 84 | 1.49 | 0.59 | 5.859 | 0.001 |
| After | 84 | 2.02 | 0.58 |
Comparison of before and after retraction mean values with Strip
| Groups | n | Mean | Std. Deviation | t-value | p value |
|---|
| Before | 84 | 1.47 | 0.58 | 7.334 | 0.001 |
| After | 84 | 2.78 | 0.62 |
Comparison of after retraction mean values of cord with Strip
| Groups | n | Mean | Std. Deviation | t-value | p value |
|---|
| After(cord) | 84 | 2.02 | 0.58 | 1.99 | 0.04 |
| After(strips) | 84 | 2.78 | 0.72 |
Comparison of before retraction mean values of cord with Strip
| Groups | n | Mean | Std. Deviation | Std. Error Mean | t-value | p value |
|---|
| Group A | 6 | 13.86 | 1.10 | 0.45 | 1.678 | 0.154 (NS) |
| Group B | 6 | 13.69 | 0.88 | 0.36 |
The statistical analysis of the collected data revealed that both the conventional retraction cord and the Merocel strip produced significant amount of gingival retraction [Table/Fig-6 & 7]. The mean vertical retraction value obtained for cord was 2.02 (p=0.001) and the mean vertical retraction value obtained for strip is 2.78 (p=0.001). The amount of retraction produced by the strip is statistically more than that produced by the cord [Table/Fig-8] (p=0.04).
The comparison of the mean values before retraction with cord and strips in Group A (13.86) and Group B (13.69) was statistically insignificant (p=0.154). Neither the cord nor the strip produced any significant change in the before retraction values [Table/Fig-9]. Hence their effect on gingival tissue health was not adverse.
The mean and standard deviation was calculated for the measurements recorded before and after retraction with the cord. Both the mean values were compared to know the amount of effective retraction (t=5.859) of significance (p=0.001).
The mean and standard deviation was calculated for the measurements recorded before and after retraction with the strip. Both the mean values were compared to know the amount of effective retraction (t=7.334) of significance (p=0.001).
The mean and standard deviation of the after retraction value with the strip and after retraction value with the cord were compared to know the difference in amount of effective retraction produced by both the materials (t=1.99) of significance (p=0.04).
The mean and standard deviation of the before retraction value with the strip and before retraction value with the cord were compared to know the effect produced by both the materials on gingival health (t=1.678) of significance (p=0.154).
Discussion
This study compared the amount of gingival displacement produced by Polyvinyl acetate strips (Merocel, Mystic, Conn) and conventional retraction cord (Ultrapak,Ultradent,USA). The study was conducted in ten patients with good general and periodontal health requiring full coverage restorations for their maxillary anterior teeth. The patients were divided into two groups. In Group A, retraction was done using cord followed by strip in two weeks interval. In Group B, retraction was done first using strip and then with cord in two weeks interval.
Measurements were recorded before and after retraction from the supragingival finish line to the crest of the free gingival margin using digital vernier caliper (Digimatic Caliper, Mitutoyo, Japan) of 0.01mm accuracy. Three points in the buccal and palatal aspect were chosen corresponding to the mesial and distal line angle and deepest point in the finish line respectively.
The collected data were analysed using paired sample t-test to test the characteristics of the data. p value <0.05 indicates significant difference between the variables.
The mean vertical retraction value obtained for cord was 2.02 and the mean vertical retraction value obtained for strip is 2.78 (p<0.001). The amount of retraction produced by the strip is statistically more than that produced by the cord.
The Merocel strips was selected for the study following the preliminary clinical study by Marco Ferrari et al., who reported that the material had beneficial physical properties like absorption of intraoral fluids, chemically pure and exerting moderate pressure on the gingival tissue without requiring local anesthesia which ensured a gingival displacement without damage [1,5]. Merocel is an absorbing, haemostatic material commonly used in otorhinolaryngic, gastric, thoracic and otoneurosurgical procedures. In his study, he investigated the Merocel material with SEM analysis and clinical procedures for effective gingival management.
However, the amount of retraction produced was not measured numerically and it was not compared with the amount of retraction produced by the conventional retraction cords. Numerous studies have reported mechanical methods that involved the use of retraction cords with or without medicaments to be the most effective, safe and easy methods for tissue displacement. Hence, in this study, the retraction cord placed by double cord technique was used as a control to compare the retracting efficacy of Merocel.
There is no consensus cited in the literature regarding criteria for evaluation of the clinical efficiency with gingival retraction cords. The only criteria for assessment of clinical performance of retraction cords identified in dental literature is the ability to stop bleeding and indirect assessments of the sulcus dilation with impression materials [2] and assessing the section of dies by travelling microscope [10].
However data on the precision and accuracy of these measurements were not reported [8]. Direct intra oral measurement with a modified Boley’s gauge [4], with a miniature video camera, periodontal probes and flexible scales were also reported. Use of video camera demands for advanced equipment, technologic experience, skill and renders the method difficult [8]. The use of flexible scales also can produce errors during visualisation of the markings intraorally.
Kamansky et al., [11] compared the gingival tissue response to rotary curettage with chemically treated cord lateral tissue displacement. In his study, vertical gingival retraction alone was measured using modified Boley’s gauge by calculating the sulcus depth after retraction by both the methods to 0.1mm accuracy manually.
In this study, vertical retraction was measured from the prepared supragingival finish line of the abutment tooth to the free gingival marginal crest before and after displacement by both materials using digital vernier caliper of 0.01mm accuracy (Digimatic Caliper, Mituyosho, Japan). Compared to the previous study, the measurements obtained in the current study were of greater degree of accuracy and use of digital values decrease the error in visualisation of the readings manually.
The gingival tissue displacement is divided into two components, vertical and lateral. Lateral retraction displaces the tissue so that an adequate bulk of impression material can be interfaced with the prepared tooth. Vertical retraction exposes the uncut portion of the tooth apical to the finish line. Some authors describe both components while others indicate only a lateral displacement [4]. Finally some amount of unprepared tooth structure and a clear demarcation of the finish line should be obtained in the die.
James Harrison [12] has reported in his study on the effect of retraction materials on the gingival sulcus epithelium as 7 to 10 days as the optimum time interval between testing two materials for gingival retraction. That time period allows the gingival health to come back to normalcy clinically. In this study, in both the groups, the interchange of retraction material was done at 2 weeks interval.
The comparison of the mean values before retraction with cord and strips in group A (13.86) and group B (13.69) was statistically insignificant (p=0.154). The order of use of the retraction materials were interchanged in both the groups to nullify the error that can occur if the same order was used.
SEM study results of the preliminary clinical report by Marco Ferrari et al., [1] has proved that the Merocel strips were free of fibers, fragments or debris when examined after use. Hence the material was considered safe for gingival health. All the cases in current study also demonstrated fluid free, haemostatic environment. The haemostatic property might be attributed to the moderate pressure exerted by the material placed in the sulcus and not because of the chemical composition.
However, use of Merocel material as a gingival retraction device carries some limitations including the need for temporary crowns at the time of impression making itself because it is difficult to secure the material in place during the process of placement and retraction. The material found to be easily placed when it is dry than when it is wet.
Limitations of this study include the difficulty in placement of the Merocel material in the gingival sulcus and the lateral gingival displacement values were not measured and included in the data. The conventional cords were used without any chemicals and the retractions achieved with both the materials were purely mechanical.
In future, studies can be conducted by changing the form of the Merocel, from strip to the cord form so that the placement becomes much easier. Lateral displacement values can also be measured and compared with mechano-chemical methods.
Summary & Conclusion
This study compared the amount of gingival displacement produced by Polyvinyl acetate strips (Merocel, Mystic, Conn) and conventional retraction cord (Ultrapak,Ultradent,USA). The study was conducted in ten patients with good general and periodontal health requiring full coverage restorations for their maxillary anterior teeth. The patients were divided into two groups. In Group A, retraction was done using cord followed by strip in two weeks interval. In Group B, retraction was done first using strip and then with cord in two weeks interval.
Measurements were recorded before and after retraction from the supragingival finish line to the crest of the free gingival margin using digital vernier caliper (Digimatic Caliper, Mitutoyo, Japan) of 0.01mm accuracy. The collected data were analysed using paired samplet-test to test the characteristics of the data. p value <0.05 indicates significant difference between the variables.
Within the limitations of this study, the following conclusions were drawn:
Merocel strip produces statistically significant amount of gingival retraction (p=0.001).
When compared with the displacement produced by conventional cord, the displacement produced by the Merocel strip is significantly more (p=0.04).
Both the materials and methods of displacement have not grossly affected the gingival health in 2 weeks follow-up (p=0.154).