Recent advances in science and technology have changed the basic approaches to many health problems. A remarkable decline in caries prevalence has been noticed worldwide, which primarily owes to the increase in scientific knowledge on the aetiology initiation, progression and prevention of disease, coupled with the widespread use of fluoride and adoption of a wide range of preventive measures [1]. Newer technologies and approaches in the field of dental caries have shifted the emphasis from the treatment of disease to prevention of disease. One of the widely used preventive dental approaches is pit and fissure sealant application.
It has been well documented that “the pits and fissures do not cause caries per se, but they provide a sanctuary to those agents which cause caries.” Pits and fissures are present on the occlusal surfaces of teeth. The complex morphology of the occlusal surface of a tooth makes mechanical cleaning (e.g. using toothbrushes) difficult and it allows plaque accumulation within deep and narrow fissures, leading to dental caries initiation within these fissures. Hence, the eradication of pits and fissures would eliminate them as caries opportunity sites, thus preventing the disease [2].
The pit and fissure sealant acts as a physical barrier, thus preventing oral bacteria and dietary carbohydrates in the oral cavity from aggregating within the pits and fissures and from developing the acidic conditions which result in the carious destruction of teeth.
However, before using a pit and fissure sealant, it is important to assess whether a dental caries process has been initiated at the base of the fissure. However, this assessment is difficult and it is possible that bacteria may be present inside a sealed narrow fissure. These bacteria may initiate caries inside the sealed fissure at a later date. Thus, 2 techniques are currently being used for sealant placements-non-invasive and invasive. The non invasive technique does not involve use of burs, while the invasive technique uses burs to open and clean out fissures. The invasive sealant approach is commonly employed, since micro-invasive treatment of the lateral fissure walls removes organic and surface debris, and thus improves adhesion of sealant materials to the occlusal enamel. This invasive technique has been reported to have better retention and diagnostic advantages [3].
One of the major problems which are usually encountered with pit and fissure sealants is the ‘retention’ of the sealant material within the fissure. The ability of pit and fissure sealants to prevent fissure caries is related to sealant retention. Therefore, maximizing wettability of tooth surface is critical in achieving a successful bond [4]. Retention of a pit and fissure sealant may be enhanced by using a bonding agent between the fissure and sealant material. The use of a bonding agent allows a fissure sealant to flow better into a fissure, by altering the rheology of the sealant material. Hitt and Feigal [5] first reported the benefit of adding a bonding agent between the etched enamel and the sealant. However, Boksman, et al., [6] suggested that the use of a bonding agent prior to the application of a pit and fissure sealant does not increase the retention rate.
The successful clinical use of a fissure sealant material depends on good bonding of the sealant material onto the tooth surface. The retention rate of a pit and fissure sealant is directly related to the micromechanical bond between the sealant and enamel. The tensile bond strength of the sealant to enamel is probably the most accurate assessment of the clinical bonding. This permits a rapid and an accurate evaluation of sealants under conditions which simulate those in the oral cavity [7]. Hence, this study was undertaken to evaluate the effect of a bonding agent on the tensile bond strength of two pit and fissure sealants by using invasive and non-invasive techniques.
Material and Methods
A total of 120 healthy, non-carious premolars, which were extracted for orthodontic purposes, were collected [Table/Fig-1]. These 120 premolars were used to study the tensile bond strength of the sealant material by using a Universal Testing Machine (UTM). The sealants which were used in the present study were Clinpro (3M ESPE) and Conseal f (SDI) [Table/Fig-2]. These teeth were divided into two groups: group-I (Clinpro) and group-II (Conseal f), with 60 teeth in each group, which would be sealed with respective materials.
Showing categorisation of different groups
| Group I (Clinpro) | Group I A | Group I A1 | Invasive with bonding agent. |
| Group I A2 | Invasive without bonding agent. |
| Group I B | Group I B1 | Non-invasive with bonding agent. |
| Group I B 2 | Non-invasive without bonding agent. |
| Group II (Conseal) | Group II A | Group II A1 | Invasive with bonding agent. |
| Group II A2 | Invasive without bonding agent |
| Group II B | Group II B1 | Non-invasive with bonding agent. |
| Group II B2 | Non-invasive without bonding agent |
Extracted teeth stored in normal saline

These groups, I and II, were subdivided according to the technique which was used, whether it was invasive (involving the use of burs) or non-invasive (without use of burs) [Table/Fig-3].
Pit & fissure sealants: Clinpro (3M ESPE) and Conseal f (SDI)

A further categorisation was done on the basis of application of bonding agent. Both invasive and non–invasive groups were classified on the basis of use or no use of bonding agent [Table/Fig-4].
Bonding agent (Prime & Bond) and Etching agent

All teeth samples were stored in distilled water at room temperature after they were cleaned. For teeth which were subjected to invasive techniques (Groups IA1, IA2, IIA1 and IIA2), fissures were prepared by using an air rotor hand piece and a 1/4 round bur, to ensure standardization and uniformity.
For non-invasive techniques, no preparation of fissures was done (Groups IB1, IB2, IIB1 and IIB2). The buccal and lingual cusps were trimmed to achieve flat occlusal surfaces without disturbing the fissures [8].
Each tooth was embedded in an acrylic block, which was made by pouring acrylic in the mould of an iron cylinder. The surfaces of all teeth were washed, cleaned and dried again. A hollow polyvinyl tube with a diameter of 6 mm and a height of 6mm was placed on the occlusal surface, almost at the centre of the specimen and it was sealed with sealant material which belonged to that group [9]. In groups I A1, IB1, IA2 and IB2, bonding agent was placed after the application of an etchant.
The sealant material was condensed to a thickness of 2 mm and it was light cured. Another 2 mm of uncured sealant was placed over it. A 26-gauge ligature wire of length 14 cm which was twisted at one end and with a loop formed at the other end was placed inside the uncured sealant material and it was then light cured. Another 2mm of sealant was then placed to stabilize the wire and it was light cured. Following complete curing, polyvinyl tubes mould was cut and removed [9] [Table/Fig-5].
All the specimens were stored for 24 hours in distilled water prior to their thermocycling 500 times [10]. Each cycle consisted of 34 secs in water baths which were set at 5± 5° and 55± 5°, with an exchange time of 13 secs between baths. A steam water bath (Labmaster) was used to maintain the temperature; glass beakers with ice cubes were also used. A lab thermometer was suspended in the glass beaker to monitor the temperature. Except for period of testing, specimens were stored in distilled water and they were tested for tensile bond strength by using a universal testing machine (LR-100, Lloyds Corp, UK) [Table/Fig-6]. Each specimen was attached between two grips of the UTM. The specimens were placed in such a position that the load was applied at right angle to the sealant plug [Table/Fig-7]. The point at which the sealant plug snapped off from the enamel surface indicated the breaking load and it signified the tensile stress.
Universal testing machine (UTM)
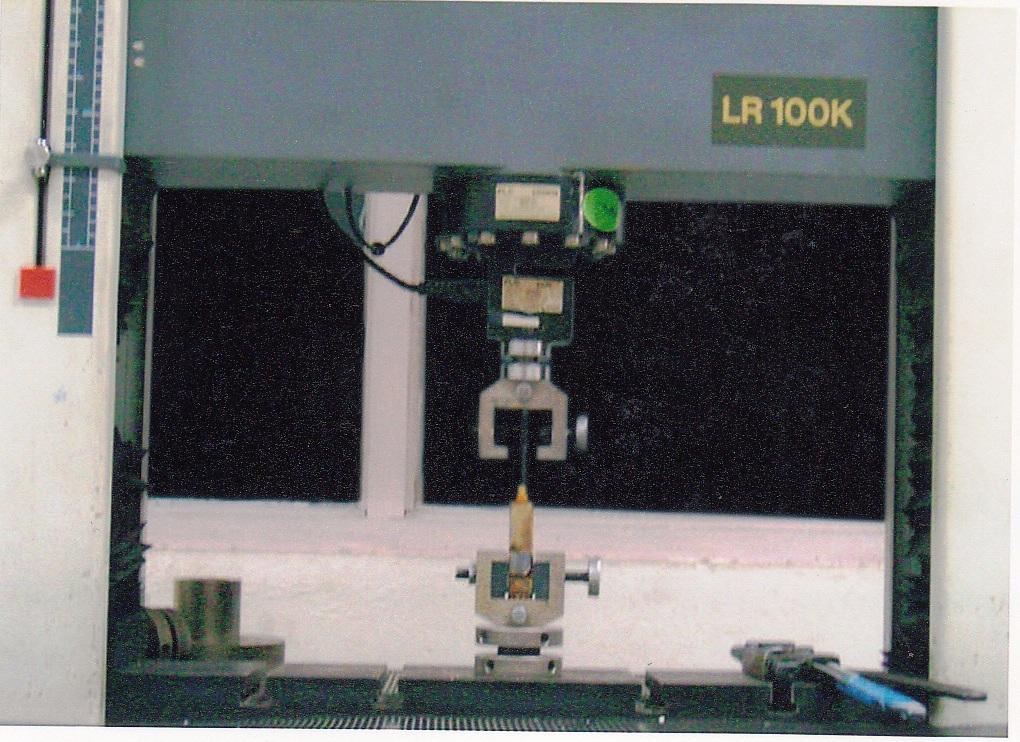
Mounted specimen undergoing testing in Universal Testing Machine (UTM)

The bond strength was calculated by the formula:
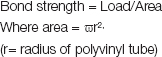
The results which were obtained were then subjected to statistical analyses.
Results
Student’s t–test was used for making a comparative analysis. When comparison of bonding agents was done, group IA1 showed a higher bond strength and statistically significant results than group IA2 (p<0.01); however, group IB1 showed statistically insignificant results than groupIB2 (p>0.05) [Table/Fig-8, 9]. Similarly, group IIA1 and IIB1 showed statistically highly significant results than IIA2 and IIB2 respectively (p<0.001) [Tables/Fig-9 and 10].
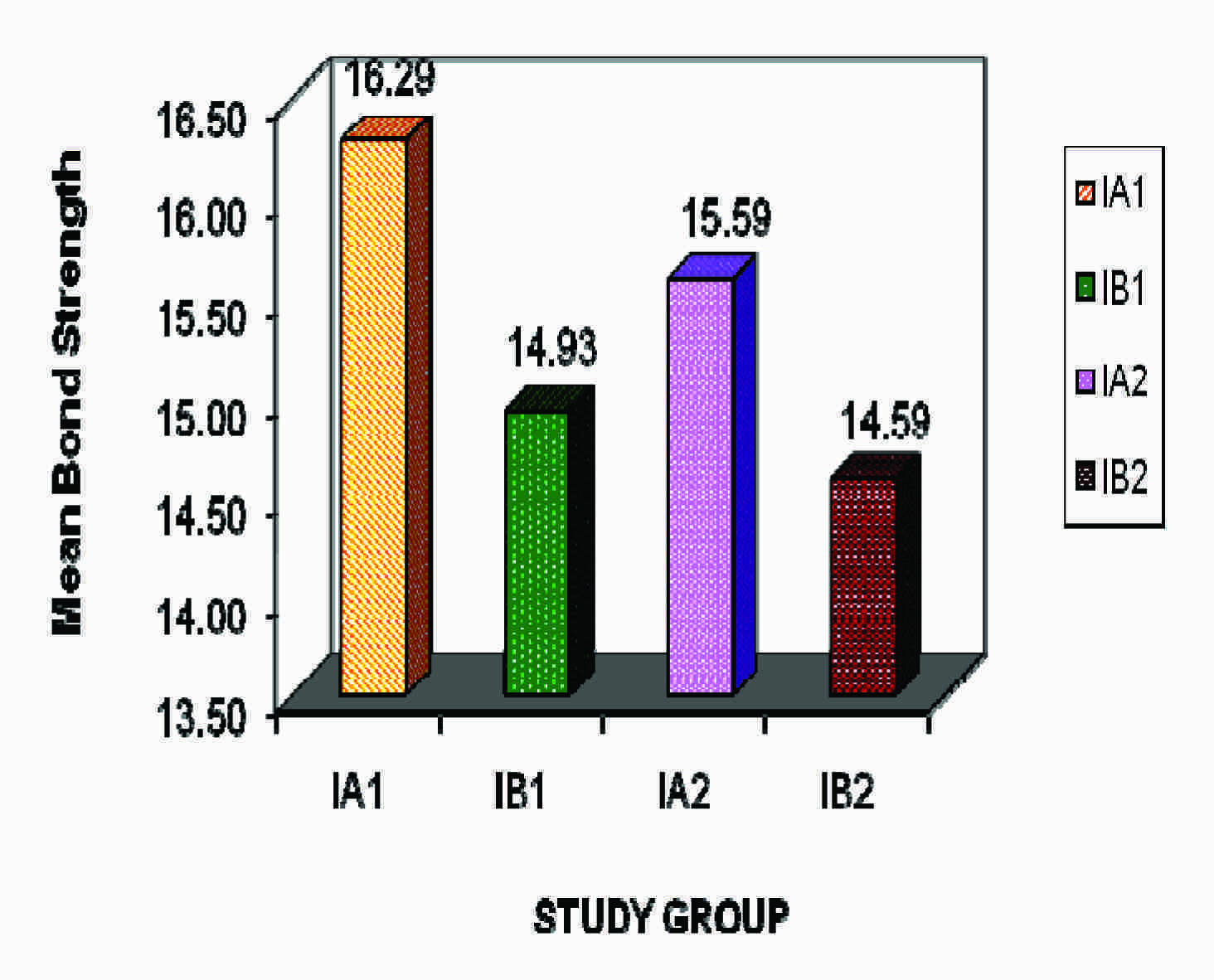
comparison of bond strength in group I (Clinpro) (with and without bonding agent)
| Particulars | Group IA1 | GroupIA2 | GroupIB1 | GroupIB2 |
|---|
| Range | 15.14-17.33 | 14.79-16.91 | 14.08-16.35 | 13.52-15.94 |
| Mean | 16.29 | 15.59 | 14.93 | 14.59 |
| Standard deviation | 0.71 | 0.63 | 0.59 | 0.70 |
Bonding agent comparison (Invasive and Non-Invasive techniques in group I & II)
| Groups | t-statistic | ‘p’ value | Significance |
|---|
| GroupIA1 | GroupIA2 | 2.856 | <0.01 | *** |
| GroupIB1 | GroupIB2 | 1.438 | >0.05 | NS |
| GroupIIA1 | GroupIIA2 | 4.560 | <0.001 | *** |
| GroupIIB1 | GroupIIB2 | 3.856 | <0.001 | *** |
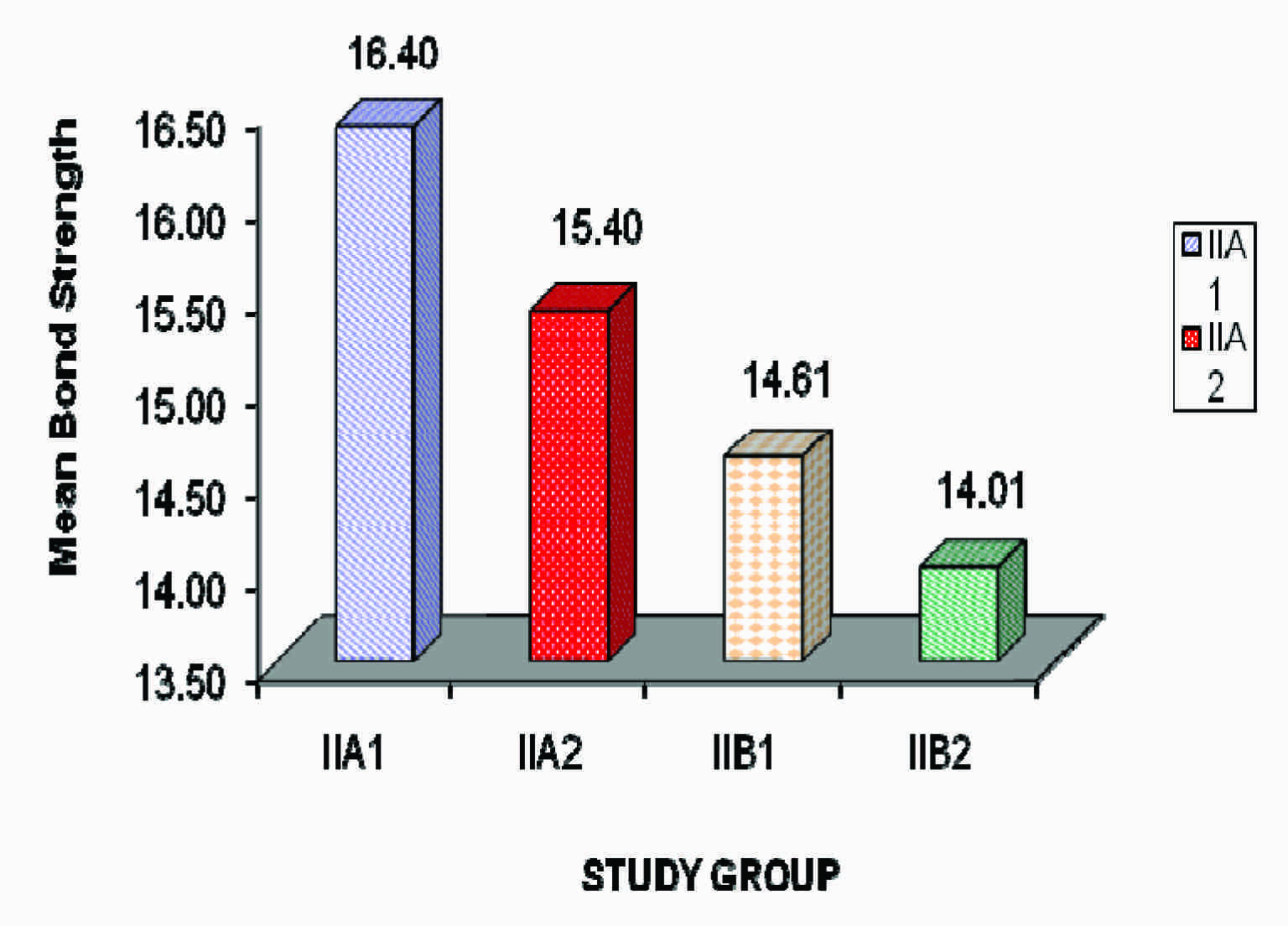
Comparison of bond strength in group II (Conseal f) (with and without bonding agent)
| Particulars | Group IIA1 | GroupIIA2 | GroupIIB1 | GroupIIB2 |
|---|
| Range | 15.49-17.62 | 14.43-16.63 | 13.65-16.13 | 12.80-15.28 |
| Mean | 16.40 | 15.40 | 14.61 | 14.01 |
| Standard deviation | 0.60 | 0.60 | 0.64 | 0.79 |
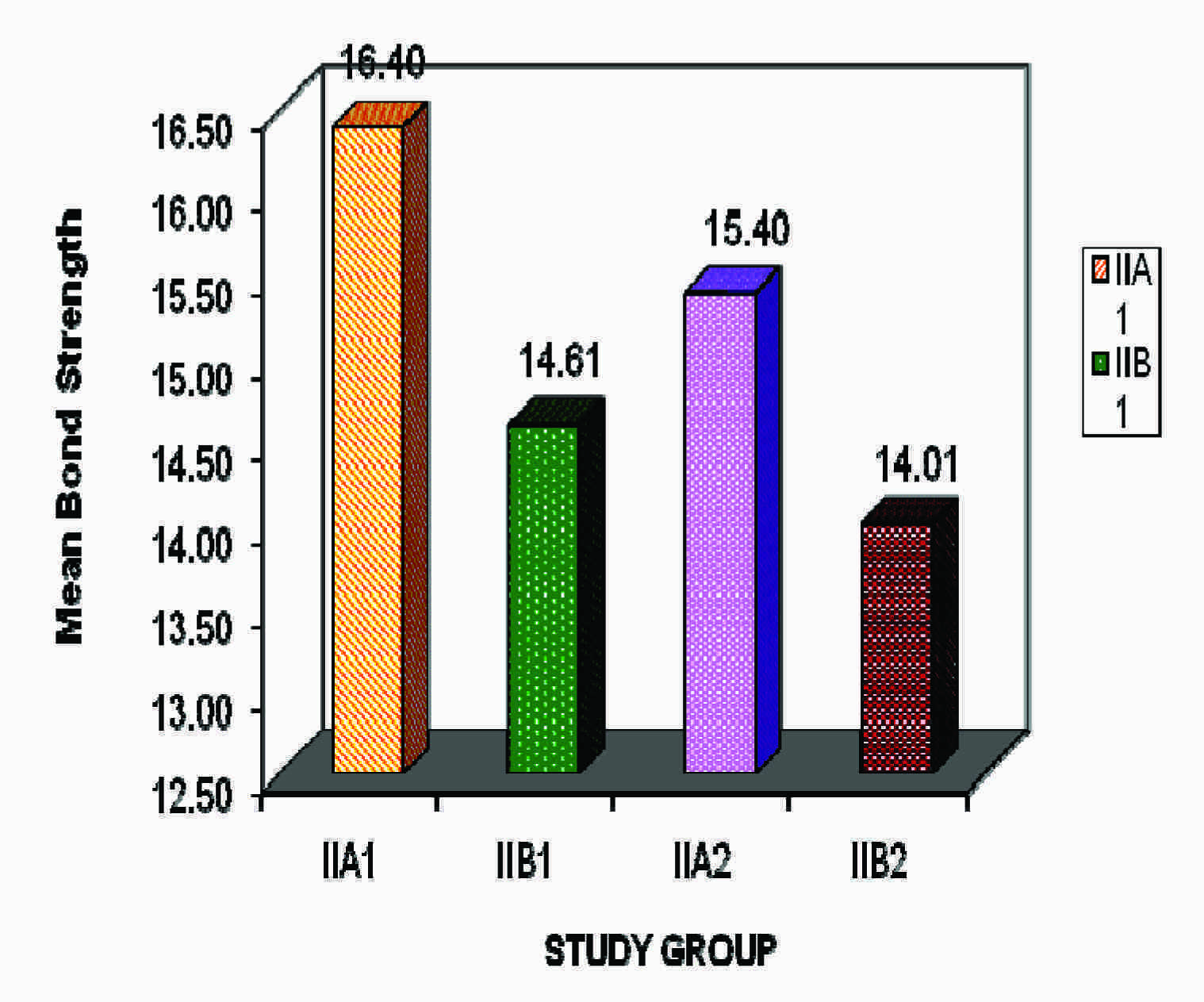
Invasive sealant placement techniques (by using bur) showed statistically highly significant results (p<0.001) as compared to non- invasive techniques in groups I and II [Table/Fig-11]. Clinpro sealant in group IB2 showed statistically significant results (p<0.05) than conseal f sealant in IIB2 (non invasive with a bonding agent), but statistically insignificant results were found when groups IA1, IA2 and IB1 were compared with groups IIA1, IIA2 and IIB2 respectively (p>0.05) [Table/Fig-12].
Comparison of Invasive with Non-invasive techniques (with and without bonding agent) in group I & II.
| Groups | t-statistic | ‘p’ value | Significance |
|---|
| GroupIA1 | GroupIB1 | 5.706 | <0.001 | *** |
| GroupIA2 | GroupIB2 | 4.113 | <0.001 | *** |
| GroupIIA1 | GroupIIB1 | 7.903 | <0.001 | *** |
| GroupIIA2 | GroupIIB2 | 5.427 | <0.001 | *** |
Sealant comparison between clinpro and conseal f
| Groups | t-statistic | ‘p’ value | Significance |
|---|
| Group I A1 | Group II A1 | 0.458 | >0.05 | NS |
| Group I A2 | Group II A2 | 0.846 | >0.05 | NS |
| Group I B1 | Group II B1 | 1.424 | >0.05 | NS |
| Group I B2 | Group II B2 | 2.128 | >0.05 | *** |
(Invasive with Non-invasive techniques with and without bonding agent)
Discussion
A lot of research has been carried out by using invasive and non-invasive techniques for the placement of sealants. Invasive techniques are considered to be better because of their advantages of better visualization of the fissures after their preparation. Also, invasive techniques allow a better diagnosis of caries which is present at the base of a fissure, as well as better retention of sealant material within a fissure. Conniff and Hamby [8] suggested that the retentive strength of acid etch bonding system was increased after a partial or a complete removal of the outermost prismless surface layer. Smutka et al., [11] reported that pre-treatment of enamel (i.e. removal of the outer most enamel surface, varied exposure to phosphoric acid and the use of an organic coupling agent) resulted in highest bond strength.
In contrast to these findings, Horsted [12] stated that the prismless surface layer of the enamel has a minimal effect on the retention of sealant. Meiers and Jensen [13], in, suggested that invasive techniques which are used in the management of questionable carious fissures provide an acceptable resolution of the bacterial infection. Dhar and Tandon [8], in and Sultana et al., [14], in 2002, suggested that invasive techniques increased the tensile bond strength of pit and fissure sealants as compared to non-invasive techniques.
However, non–invasive sealant placement techniques also present with certain advantages. The main advantage of a non–invasive fissure sealing technique is that the intact tooth structure is retained; this supports the fundamental principles of minimal invasive dentistry. This principle was supported by the work of Duangthip and Lussi [15].
Salivary contamination of the fissure surfaces has a well documented negative effect on sealant bond strength. Hitt and Feigal [5] were the first to report the benefit of adding a bonding agent between the etched enamel and the sealant, as a way of optimizing bond strength in the face of moisture and contamination. In 1993, Feigal [16] reported that sealant retention was possible on wet enamel if a bonding agent was used between enamel and sealant. Borem and Feigal [17] reported that placement of a Scotchbond bonding agent between the sealant and enamel reduced microleakage of sealants which were applied under conditions of salivary contamination.
The use of a bonding agent enhances the adhesion of a sealant material onto the tooth surfaces. The use of a bonding agent under a sealant in moisture contaminated conditions may give better results than applying a sealant alone onto non-contaminated teeth. Tulunolu et al., [4] reported that the use of an enamel–dentine bonding agent under a fissure sealant increased the bond strength and that it decreased micro leakage. Feigal [18] reported that adding a bonding agent layer between sealant and saliva contaminated enamel allowed adequate bond strength and retention of resin sealants. However, in a contrasting study, Gomes-Silva [19] concluded that individual or simultaneous curing of the intermediate bonding agent layer and the resin sealant did not seem to affect bond strength to saliva-contaminated enamel.
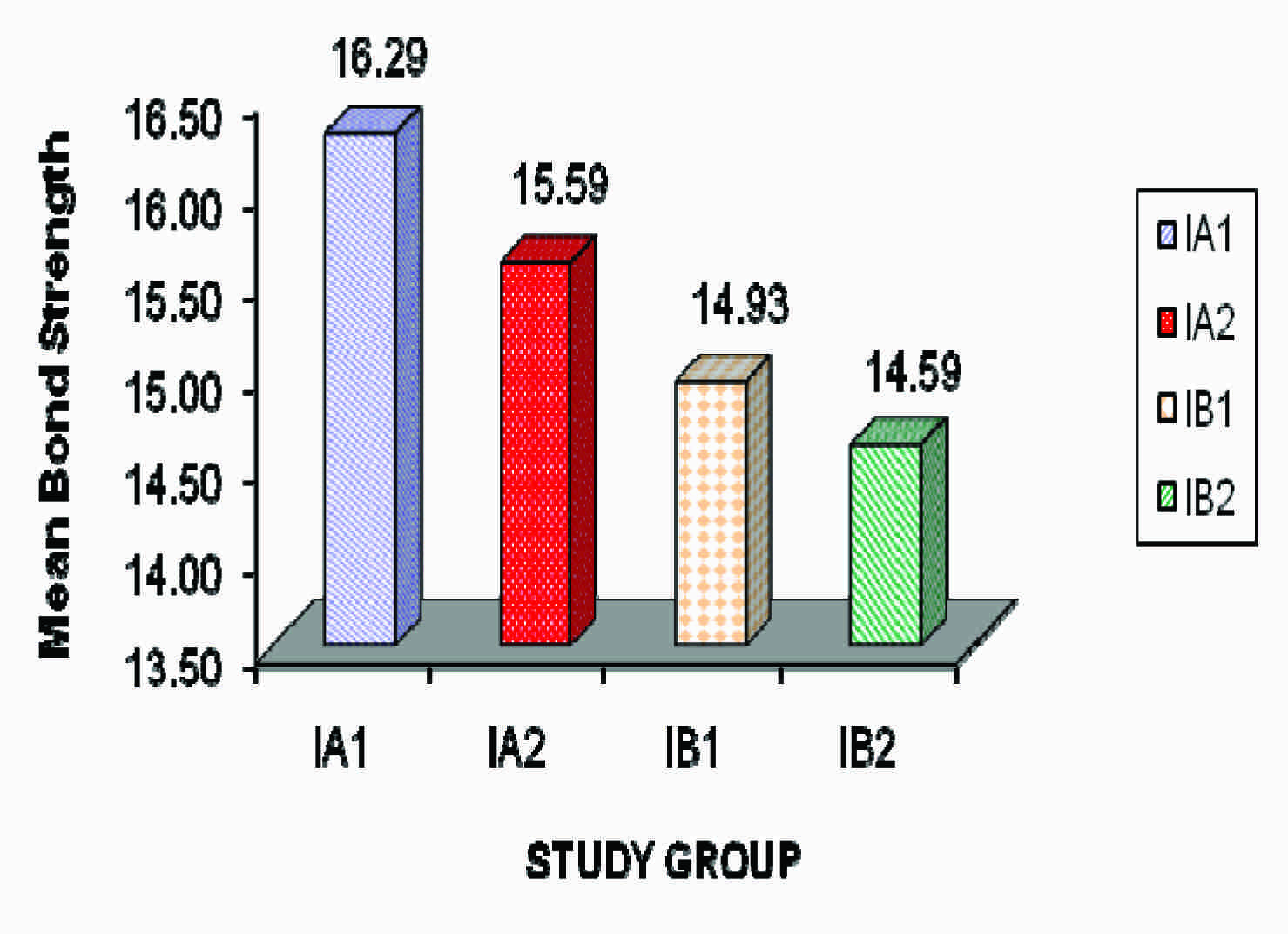
Sen Tunc et al., [20], Borsatto MC, Thomaz MY et al., [21] concluded that the oil contamination affected negatively the sealant bonding to enamel and the acetone-based adhesive system (Prime and Bond) layer applied underneath the sealant was able to prevent its deleterious effects to adhesion. In concluded that sealant microtensile bond strength values could be affected by material content and that the addition of an adhesive could improve microtensile bond strength values of sealant to enamel. In the invasive group, the mean tensile bond strength of group IA1- Clinpro (invasive with bonding agent) was found to be 16.29 MPa and 15.59 MPa for group IA2- Clinpro (invasive without bonding agent) [Table/Fig-13].Similarly group IIA1 –Conseal f (invasive with bonding agent) gave bond strength of 16.40 MPa and 15.40 MPa for group IIA2 –Conseal f (invasive without bonding agent) [Table/Fig-14]. The results of tensile bond strength in the present study were in agreement with those of a study which was done earlier by Dhar and Tandon [8].
Comparison of bond strength in group I (with and without bonding agent)
Comparison of bond strength in group II Conseal f (with and without bonding agent)
Slightly higher bond strengths than a previous studies carried out by Dhar and Tandon [8] and Sultana et al., [14]. Thus, the present study showed that the addition of bonding agents significantly increased the tensile bond strengths of the sealants in both invasive and non-invasive techniques. These findings were in agreement with those of previous studies which were done by Hitt and Feigal, [5] Feigal et al., [16] Choi et al., [22] Tulunolu et al., [4] and Perdigão et al., [23]. The increased bond strength in this study may be attributed to the alteration of rheology of the material with the use of bonding agent, which may have allowed it to flow better into the fissures and acid etched surfaces.
In the non-invasive group, the mean tensile bond strength of 14.93 MPa for group IB1-Clinpro (non-invasive with bonding agent) and 14.59 MPa for group IB2-Clinpro (non-invasive without bonding agent) [Table/Fig-13], which was not found to be statistically significant at (p >0.05). However group IIB1-Conseal f (non-invasive with bonding agent) gave mean bond strength of 14.61 MPa and 14.01 MPa for group IIB2-Conseal f (non-invasive without bonding agent), [Table/Fig-14]. These findings were similar to those of a study which was done by Dhar and Tandon [8]. This signified that addition of a bonding agent in a non-invasive technique did not significantly increase the bond strength of the sealant. This can be accounted for by the fact that no preparation was done for the non-invasive group.
In the present study, the groups with invasive techniques showed increase in bond strengths as compared to the non-invasive groups [Table/Fig-15 and 16]. These results were in agreement with those of previous studies which were done by Garcia-Godoy and de Araujo, [24] Dhar and Tandon, [8] Sultana et al., [14] Salama and Al-Hammad [25]. The probable reasons for the higher bond strengths in invasive sealant placement techniques as compared to those in non- invasive techniques may be due to:
Comparison of bond strength in group I (Invasive and non-invasive techniques)
Comparison of bond strength group II (Invasive and non-invasive techniques)
The fact that a mechanical preparation widens and deepens the fissures and provides more surface area to retain sealant.
The sealant easily penetrates the enlarged fissure and adheres to walls, resulting in a better bond strength.
The removal of prismless layer of enamel facilitates the conditioning of surface, resulting in improved bond strengths in invasive techniques.
Currently, fluoride releasing pit and fissure sealants have gained popularity because of their advantages of fluoride release and a possible cariostatic action. Taking this into consideration, in the present study, two fluoride releasing sealants were used- Clinpro (3M ESPE) which was a light cured, bis GMA/ TEGDMA-based unfilled sealant, with a colour change chemistry which could aid in placement procedure and Conseal f (SDI) which was a 7% filled resin with a submicron filler size of 0.04 microns, which could withstand wear.
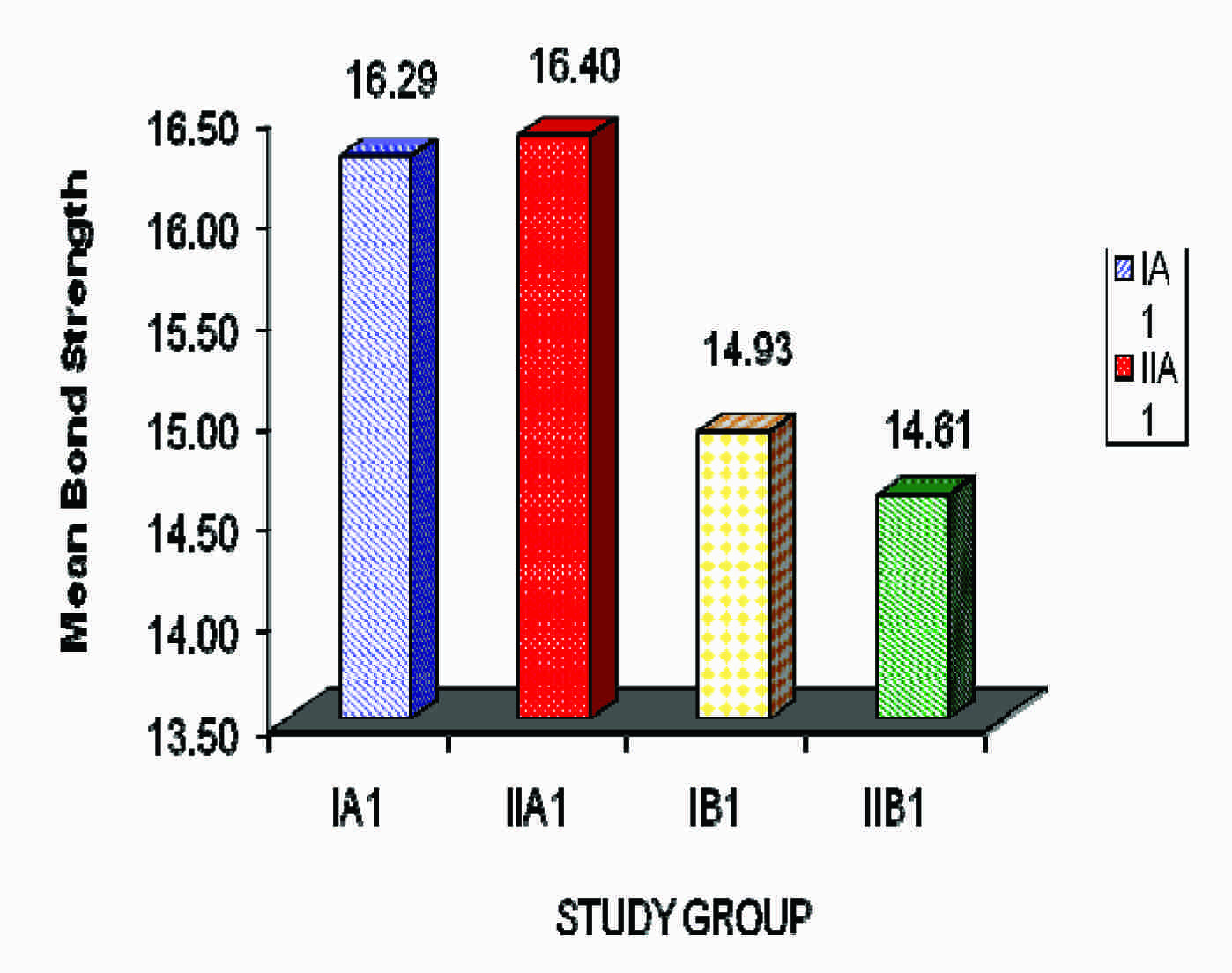
On comparison of mean tensile bond strengths which were obtained by Clinpro and Conseal f sealants, Conseal f showed a slightly higher bond strength (16.40 MPa) than Clinpro (16.29 MPa). However, the results were statistically not significant (p>0.05) [Table/Fig-17]. These findings were in accordance with those of previous studies which were done by Dhar V and Tandon S [8] and Sultana MN [14] et al., (2002). However, the present study showed significantly higher tensile bond strengths than those which were reported by other studies. This difference in bond strengths may be explained on the basis of the fact that Clinpro and Conseal f may have penetrated deeply into the pits and fissures, resulting in better bond strengths and also, the materials which were used were different.
Comparison of bond strength of clinpro and conseal f sealants (Invasive and non-invasive with bonding agent)
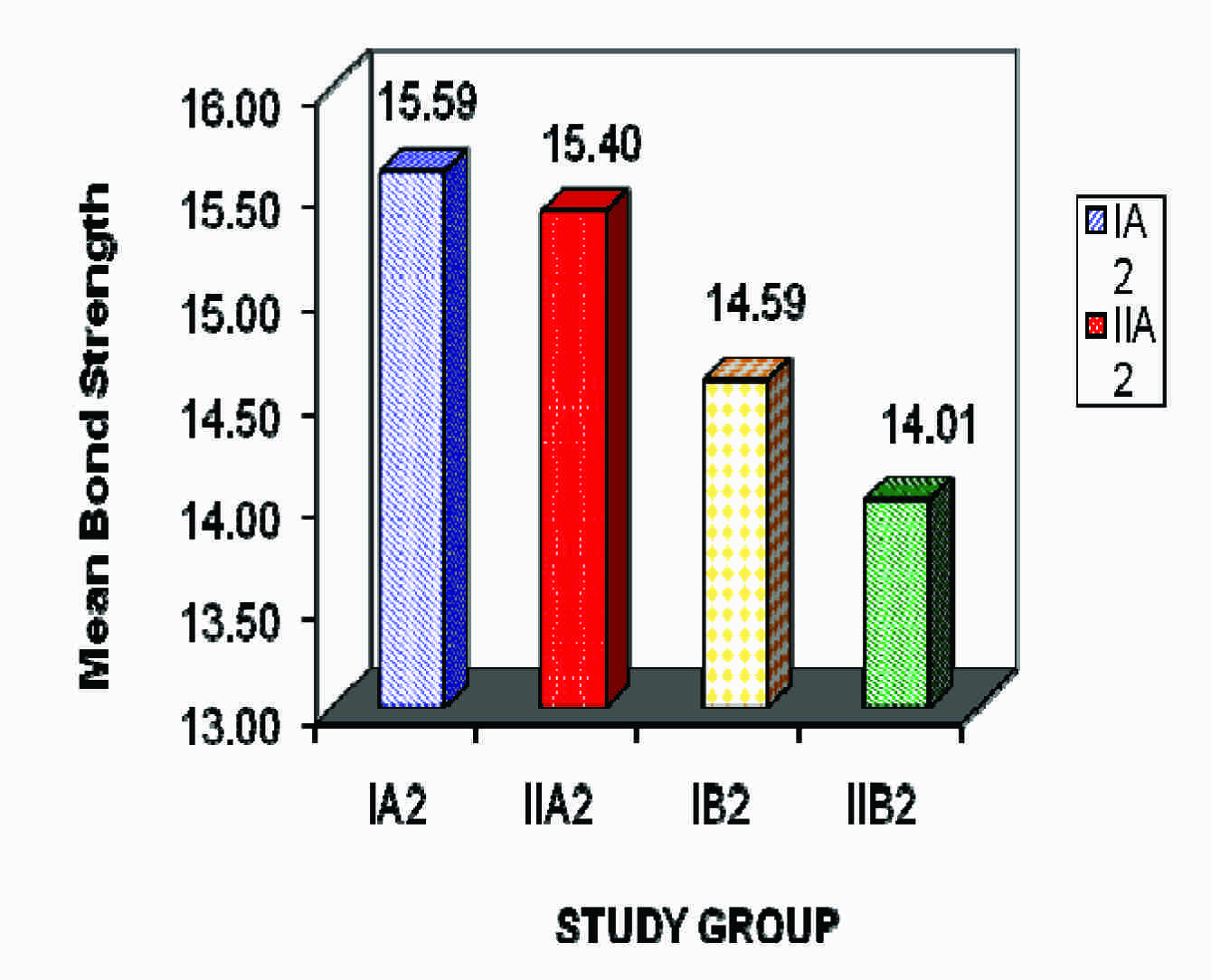
The present study showed mean tensile bond strengths of 14.93 MPa and 14.61 MPa for Clinpro and Conseal f respectively in non- invasive with bonding agent group and of 14.59 MPa and 14.01 MPa for Clinpro and Conseal f respectively in non-invasive without bonding agent group. According to an in–vitro study which was conducted by Sultana M.N. [14] in Teethmate F and 3M Concise sealants showed bond strengths of 12.66 MPa and 9.54 MPa respectively for non-invasive group. The present study showed higher bond strengths for Clinpro and Conseal f respectively in non-invasive group as compared to those which were seen in a study which was previously conducted by Sultana M.N.
However, Dhar V and Tandon S [8] found a bond strength of 14.8 MPa of Teethmate F sealant in non-invasive group, which was slightly higher than the bond strengths which were obtained in the present study in non-invasive without bonding agent group. This difference can be explained on the basis of the fact that the materials which were used are different. The results were not statistically significant in non-invasive group, but Clinpro sealant showed a higher bond strength than that of Conseal f in both the groups (non–invasive with and without bonding agent) [Table/Fig-17 and 18].
Comparison of bond strength of clinpro and conseal f sealants (Invasive and non-invasive without bonding agent)
It was seen that the use of a bonding agent underneath the sealant in invasive techniques significantly increased the tensile bond strength of the sealants. Therefore, invasive techniques with bonding agents can be considered for all types of sealant materials, whereas non-invasive methods should only be considered for materials with proven good strengths.
Though the methods which were employed in this in–vitro study proved to be effective in covering a majority of parameters, they could not simulate in vivo conditions in totality. Hence, long term clinical trials need to be undertaken, to further test the efficacy of retention of sealants with and without bonding agents by using either invasive or non-invasive techniques.
Conclusion
The invasive sealant placement technique (by using burs for fissure preparation) increased the tensile bond strengths of pit and fissure sealants as compared to the non-invasive sealant preparation technique. The use of bonding agents in non–invasive sealant placement technique did not significantly increase the bond strength of the sealant materials, but use of bonding agents in invasive technique gave better results than in the non–invasive technique. Overall, Clinpro sealant performed better than Conseal f sealant in terms of tensile bond strength.
(Invasive with Non-invasive techniques with and without bonding agent)