Developmental anomalies of the dentition are not frequently observed in clinical practice. However, these anomalies account for a relatively low number of cases as compared to the more common oral disorders such as dental caries and periodontal diseases. Their clinical management is usually complicated, as they present with malocclusions, aesthetic problems and a possible disposition to other oral diseases.
Dental anomalies occur during the embryological and developmental life of the tooth and they usually involve a single tooth germ. The dental anomalies can be classified into different groups: as anomalies which are based on the volume, number, form, position and union of the teeth.
Although the aetiology is not clear, environmental factors, trauma, vitamin deficiencies, systemic diseases as well as certain genetic predispositions have been described as the possible causes [2–4]. Usually, there is a furrow of variable depth, that may or may not continue throughout the crown and root, indicating the line of adhesion between both tooth germs [3]. Radiographs help in delimiting the layers which are involved in fusion/gemination and to check whether the fusion is total or coronary. Gemination occurs more in primary dentition (0.5% prevalence in children) than in permanent dentition (0.1% prevalence in adults) [4,5]. Predilection is more in maxillary primary incisors and canines [2]. The frequency of a bilateral gemination is 0.02 % in both dentitions and it is found more frequently in Mongolian race (5%) than in Caucasian race(0.5%) [5].
Many epidemiological surveys have been conducted in different parts of the world, to determine the prevalence of various types of dental anomalies [6–13]. The results have shown that there are regional and ethno racial variations in the prevalence of dental anomalies. This paper has presented the results of a clinical and radiovisuographic survey which was done on anomalies of maxillary lateral incisor tooth number and morphology in Odisha, India, population along with treatment and aesthetic correction of geminated maxillary left–lateral incisor.
Methodology
A total of 1062 subjects who were aged between 15-30 years (724 males and 338 Females) were randomly screened at the Institute of Dental sciences in Bhubaneswar, Odisha, India. The clinical criteria included subject’s age, gender, number of teeth and shape and size of lateral incisors. History of extraction of lateral incisor was not considered for study. These clinical details were taken by an experienced clinician. Each subject was examined clinically for dental anomalies in relation to maxillary lateral incisors. Pregnant women were excluded from the study.
Radiovisuographic images (RVGs) (Schick Technologies Inc.) were taken in subjects with missing teeth or with abnormal sizes and shapes of maxillary lateral incisors, to detect the nature of the anomaly. Informed consents of subjects were taken for RVGs and all precautions were taken to minimize radiation exposure. The RVG images were analyzed carefully by using an inbuilt image viewing software, by an experienced clinician and by one of the authors. The data was collected and statistically analyzed by using Chi-Square and Fisher Exact tests.
Case Report
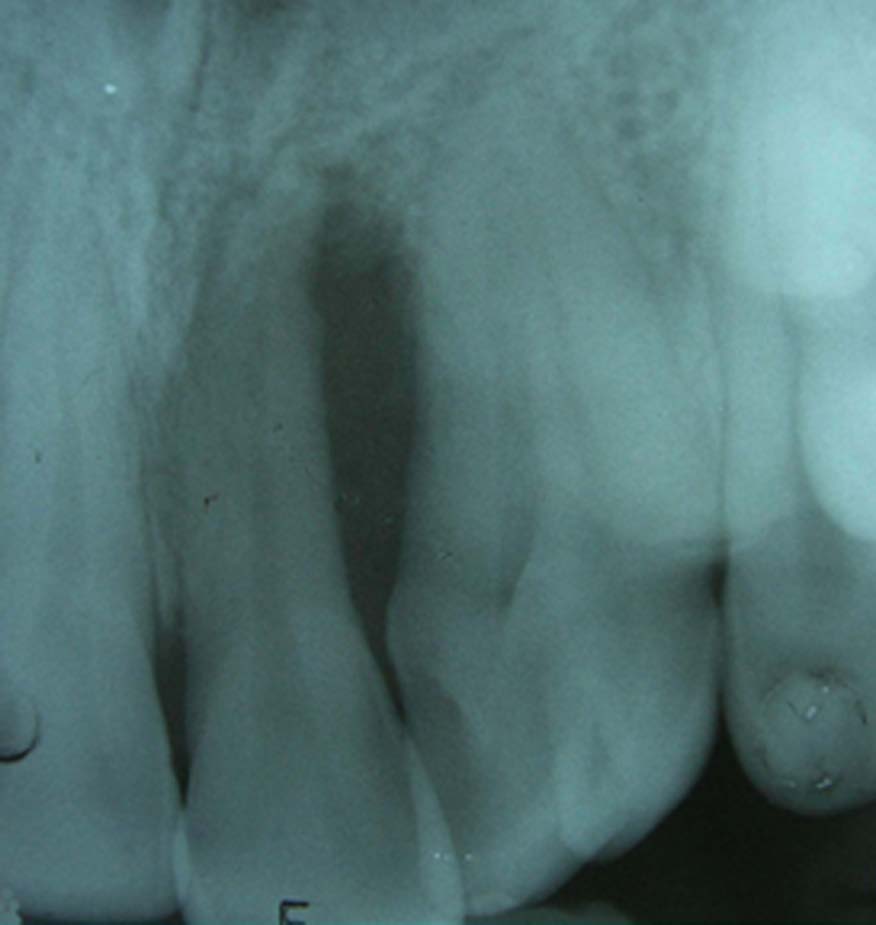
During the survey, an interesting case was identified, described below. A 20-year-old female was referred to the Department of Conservative Dentistry and Endodontics for aesthetic correction of her maxillary left lateral incisor. Her medical history was noncontributory. Clinically, the crown of the tooth which was concerned was found to be bifid and a Grade I mobility was noticed [Table/Fig-1].

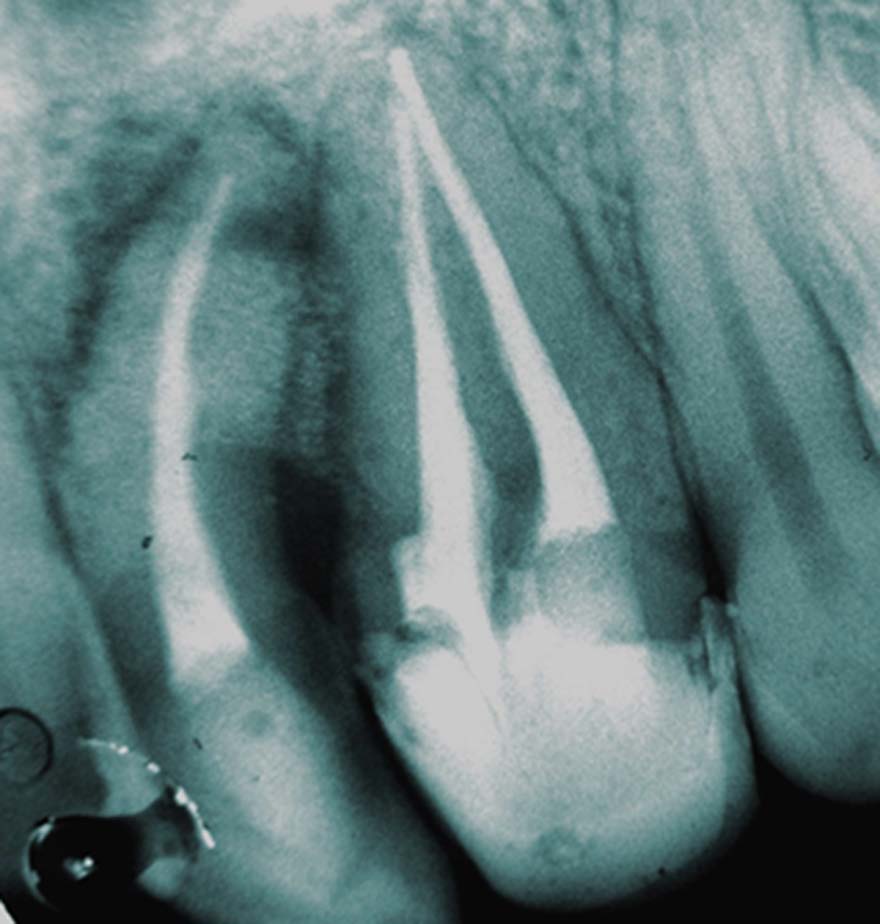
Thermal pulp testing and electric pulp testing (Digitest™ Pulp Tester-Parkell) showed a negative response in central incisor and delayed response in lateral incisor. On probing, a periodontal pocket of 10mm was revealed in between the maxillary left central and lateral incisors. Both teeth were caries free and no missing tooth was detected in the dental arch. An intra-oral periapical radiograph revealed a possible connection between the pulp canals in the lateral incisor and an apical distal curvature in the central incisor [Table/Fig-2]. A vertical bone loss was observed in between the two teeth. The corresponding tooth on the opposite side of the arch appeared clinically and radiographically normal. The tooth was anaesthetized with 2% lidocaine (1:100,000 epinephrine Xylocaine; Astra Zeneca Pharma Ind Ltd, Bangalore, India.), isolated with a rubber dam and access cavities were prepared for maxillary left central and geminated lateral incisor. Two access cavities were prepared on the geminated tooth, pulp was extirpated and pulp chambers were irrigated by using 3% sodium hypochlorite (NaOCl).
Determination of the working length was done by using an apex locator (X-SMART Dual, Dentsply Maillefer) and it was confirmed on RVG. Coronal flaring was done with gates glidden burs/drill (Mani, Inc., Tochigi, Japan), numbers 4 and 5 and cleaning and shaping of root canal was done with K-flex hand files (Dentsply) by a hybrid technique under a copious irrigation of 3% NaOCl. AH Plus resin sealer (Dentsply Maillefer, Ballaigues,Switzerland) was used for obturation with cold lateral compaction, followed by warm vertical compaction. Access cavity was sealed with IRM cement (Dentsply De Trey GmbH, Konstanz, Germany)
In the subsequent appointment, curettage was done and a bioactive synthetic bone graft material (Perioglass, Nova Bone) was used to fill the bony defect [Table/Fig-3a and 3b]. Ceram X Mono (Dentsply) composite restorative material was used for access cavity restoration of the central incisor and aesthetic correction for the Geminated tooth [Table/Fig-4].
Bone graft placement during surgery

Post-operative photograph (Lateral view)

Result of Survey
Five dental anomalies such as gemination, fusion, missing lateral incisors, peg shaped incisors and dens in dente were studied in 1062 subjects. A total of 57 subjects were found to have maxillary lateral incisor anomalies. Details of number of subjects and gender distribution of the anomalies are given in [Table/Fig-5].
showing types of anomalies of lateral incisors and their percentage
| Types of Anomaly | Percentage (%) |
|---|
| 1. Peg shaped | 2.82 |
| a) Unilateral | 1.12 |
| b) Bilateral | 1.70 |
| 2. Missing | 1.88 |
| a) Unilateral | 1.41 |
| b) Bilateral | 0.47 |
| 3. Gemination | 0.28 |
| 4. Fusion | 0.18 |
| 5. Dens in Dente | 0.18 |
Discussion
In the survey, a total of 1062 subjects were studied for dental anomalies in maxillary lateral incisors. RVGs were obtained to confirm anomalies of lateral incisors. Dental anomalies can result from many factors like a genetic predisposition, trauma, a vitamin deficit, systemic diseases and environmental causes. Although defects in certain genes are the most influential aetiological events in the prenatal period, post natal periods have also been blamed for anomalies in tooth dimensions, position, and number [2,4,5,14]. Maxillary lateral incisors vary in form more than any other tooth in the mouth, except the third molars [15].
The incidences of gemination and fusion in this study were 0.28% and 0.18% respectively. These values were lower as compared to those of other studies [5]. Traditional terminologies such as concrescence, fusion and gemination should be considered as potential embryologic causes of the anomalies and not as the exact diagnoses [6,12]. Fusion or gemination are developmental anomalies with inherently bizarre anatomies. In order to distinguish between fusion and gemination, it has been suggested that the teeth in the arch be counted, with the anomalous crown being counted as one. A full complement of teeth indicates gemination, whereas one tooth less than normal indicates fusion. This rule is compromised if a normal tooth fuses with a supernumerary tooth [13].
The incidence of peg shaped maxillary lateral incisors (2.82%) in our study was in accordance with those in other studies [16–19]. It was also noted, as in other studies, that unilateral pegs were mainly present on left side of maxilla [20].
Missing maxillary lateral incisors accounted for 1.6% subjects in this study. An earlier study which was done by Pinho [7] reported a prevalence of 1.3% for such an anomaly. Nordgarden reported a prevalence of 0.9% for this anomaly in Norway [9].
The prevalence of dens in dente ranged from 0.04%–10% [21, 22]. The teeth which were most affected were permanent maxillary lateral incisors and a bilateral occurrence was not uncommon. It occurred in 43% of all cases [23,24].
Cakici et al., reported that dens in dente was detected in only maxillary lateral incisors, with no gender difference [25]. The permanent maxillary lateral incisor appeared to be the most frequently affected tooth, with the posterior teeth being less likely to be affected [26]. A primary dentition involvement was reported in another study [27].Hamasha and Al-Omari [28], in 2004, conducted 1660 full-mouth surveys and found the frequency of dens in dente to be 2.95% in patients and 0.65% in teeth.
Incidence of dens in dente was found to be 0.18% in our study and unilateral only. General features of teeth with dens in dente included peg shaped formations, incisal notching, increased labio-lingual and mesio-distal diameters, a conical morphology and the presence of an enlarged palatal cingulum or a cusp [29].
In this case report, the number of teeth was normal and a differentiation from gemination was difficult or impossible. Concerning the treatment, an exact differentiation between fusion and gemination may not be critically important.
An access preparation was done as two separate coronal entries, to preserve as much tooth structure as possible and a communication was discovered between the two pulp canals in the apical third of the tooth.
As periodontal defect involved both the central incisor and the geminated lateral incisor, an endodontic treatment and subsequently, a periodontal treatment were done. The bioactive bone graft material which was used was Perioglass, due to its easy availability and simpler application. Except for a mesial overlapping of the geminated lateral incisor on central incisor, all teeth were arranged symmetrically in the arch. In order to enhance the aesthetics, reduction of the mesiodistal size of the maxillary lateral incisor was done, which provided the required space for composite restoration.
Other common treatment alternatives for treating geminated tooth include extraction, hemisection, reshaping after the endodontic treatment and just leveling of the dental arch without any intervention.
Conclusion
A careful clinical and radiographic examination is essential to decide the fate of the tooth. Even if mid-root connections between the pulp chamber become evident, a proper multidisciplinary approach helps in treating any anomaly of the tooth.
The present case report indicates that Geminated tooth may present aesthetic and functional problems, which may require endodontic treatment, bone grafting and composite restoration. In the present study, incidences of germination, fusion and dens in dente were found to be low.
Limitations of The Study
Although panoramic radiographic examinations of individuals would have allowed more accurate data regarding other dental anomalies and morphologies, this was not feasible in the current study
Potential Conflicts of Interest: None