Perioperative Respiratory Compromise in Patients Undergoing PCNL-A Case Series
Ponnambala Namasivayam S.1, Gayathri2, Indu3
1 Professor, Department of Anaesthesiology, Goverment Stanley Medical College and Hospital, Chennai, India.
2 Assistant Professor, Department of Anaesthesiology, Goverment Stanley Medical College and Hospital, Chennai, India.
3 Post Graduate Student, Department of Anaesthesiology, Goverment Stanley Medical College and Hospital, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ponnambala Namasivayam S., Professor, Department of Anaesthesiology, Goverment Stanley Medical College and Hospital, Chennai, India.
Phone: 9444451853,
E-mail: ponnambalan@yahoo.co.in
Percutaneous Nephrolithotomy (PCNL) is a surgical procedure which is used to extract renal pelvic stones. An optimum access tract, without traumatizing the surrounding structures, is essential for the surgery. Trauma to the surrounding structures and extra–vasation of the irrigating fluid may result in complications like hydrothorax, pneumothorax, hydro pneumothorax etc. These complications may produce intra– operative respiratory compromise leading on to arterial hypoxemia and its sequelae. A series of three case reports with review is presented here. First case is accumulation of irrigating fluid in the pleura causing hydrothorax and oxygen desaturation. Second case is extra–vasation of fluid in the abdominal wall and the patient was ventilated artificially for 24 hours. Third patient developed pneumothorax and he needed chest drainage.PCNL is done under general anaesthesia in prone position. The anaesthesiologist should be vigil enough to identify the situation and take appropriate measures to correct it.
Percutaneous nephrolithotomy (PCNL), Complications, Pneumothorax
Introduction
PCNL or Percutaneous nephrolithotomy is a procedure by which a renal pelvic stone is extracted through a percutaneous tract [1]. PCNL is generally offered for staghorn calculi, stones greater than 2cm and those that are difficult to disintegrate by ESWL [2]. The advantage of PCNL over open procedure is its decreased cost, shorter operative time, decreased requirement of blood transfusion, decreased analgesic needs and an earlier return to activity [3].However, PCNL is also associated with multiple complications associated with significant morbidity. These include haemorrhage, collecting system injuries, contiguous organ injuries, hypothermia, fluid overload, sepsis, and renal loss [4,5]. Since, these complications occur during the peri-anaesthetic period, anaesthesiologist should be prepared to anticipate, identify and rectify these complications. Here we present three cases of PCNL that were associated with peri–operative respiratory compromise.
Case 1
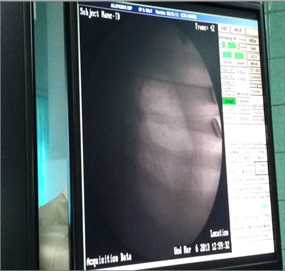
A 50-year-old lady was diagnosed with right - sided renal calculus was posted for PCNL. She was assessed under ASA I and the surgery was performed under general anaesthesia in prone position. Towards the end of the procedure, her oxygen saturation dropped down to 92%. Airway pressure was found to be elevated. Auscultation of the chest revealed decreased breath sounds on the right base. C- Arm showed right hydrothorax [Table/Fig-1]. Decreased lung expansion was noted on fluoroscopy. The patient was immediately turned to the supine position and a chest tube was inserted. Around 1500 ml of irrigation fluid was drained. The patient was then ventilated with high PEEP to expand the lung. Repeat C arm confirmed correct placement of the chest tube and re–expansion of the lung. The patient was observed for 30 minutes and then extubated. Post-operative recovery was uneventful and the chest tube was removed on the second day.
Case 2
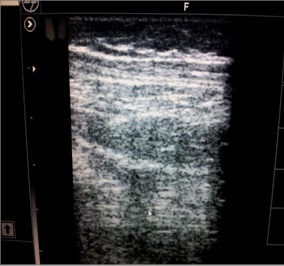
A 46-year-old gentleman was diagnosed with right-sided renal calculus was scheduled for PCNL. He had been treated for pulmonary tuberculosis 10 years back. Chest X-ray showed apical fibrosis of the right lung. He was accepted for surgery under ASA II. General anaesthesia was initiated and the patient turned to the prone position for surgery. There was no untoward event intra– operatively. At the end of the procedure, airway pressure was found to be mildly increased. Air entry was equal in all lung fields on auscultation and oxygen saturation was 100%. X-ray of the chest obtained with the C-arm was normal. However, on turning the patient to the supine position, the abdomen was found to be distended and stony hard. Ultrasound of the abdomen was performed which revealed fluid accumulationin the inter–muscular plane [Table/Fig-2]. A surgical incision was made in each flank and 1-liter of irrigation fluid was drained from the abdominal wall. The abdominal distension was decreased but not completely. The patient was not extubated on the table for fear of restriction of respiration. The patient was electively ventilated and extubated after 24- hours without further complications.
Case 3
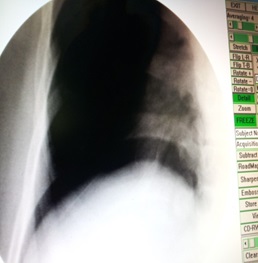
A 55- year- old lady was admitted to the hospital with left- sided renal stones. Anaesthetic assessment was obtained under ASA I and she was posted for PCNL. After the administration of general anaesthesia, the patient was turned to prone position for surgery. Intraoperative haemodynamics was stable and no complication was noted. She was reversed and extubated on table. After extubation, her oxygen saturation dropped done to 90%, and respiratory rate increased to 30 per minute. A hyperresonant note was heard on percussion of the left chest. There was decreased air entry on the left side on auscultation. She was diagnosed with left pneumothorax. This was confirmed by using C- arm and fluoroscopy [Table/Fig-3]. A chest tube was immediately inserted. Oxygen saturation picked up to 99% and the respiratory rate decreased to 22 per minute. She was shifted to ICU and observed for 24 hours. She recovered with no further complications, and was discharged after removal of chest tube on the 3rd day.
Discusssion
The success of PCNL is directly related to the ability to achieve an optimum access tract without traumatizing the kidney and its surrounding structures.
There are two ways in which the stones can be accessed through a percutaneous tract. The calculi in the lower calyces and the renal pelvis are approached through a sub–costal tract. The upper and mid-calyceal stones are removed through a supra–costal tract.
The complications of PCNL can be divided as major and minor. Minor complications include pain, fever and UTI. The two major complications are septicemia and severe hemorrhage.
When the sub–costal approach is used to access the inferior calyx, there is considerable angulation and torque applied on the kidney that can cause trauma and bleeding. The supra–costal approach on the other hand has the potential for injury to the pleura and the lung leading to morbid complications such as pneumothorax, hydrothorax and hydro pneumothorax [6,7,8]. Accumulation to irrigation fluid in the pleural space can lead to hydrothorax. The incidence of hydrothorax is 0-12% [9–11]. This occurs, either due to failure to seal the tract with the working sheath during the procedure or as a result of inadequate drainage of the kidney afterward [12]. A more cephalad access, higher than the 11th rib can cause visceral injury to the liver and the spleen. If care is not taken to stay above the upper border of the lower rib when making serial dilatations, the inter–costals artery can get lacerated leading to massive blood loss [12].
Anaesthetic Implications
Percutaneous nephrolithotomy is done under general anaesthesia. Hence, it becomes mandatory for the anaesthesiologist to actively participate in the prevention and management of its complications. The rate of complications appears to be proportional to the comorbidities. Pre–operative investigations should include a Chest X-ray, complete blood picture, renal function tests, and a coagulation profile. Information about the probable need for intercostal drainage should be explained to all patients and informed consent should be obtained before surgery. Intra–operative monitoring should include pulse oximetry, ECG, NIBP, temperature, Et CO2 and airway pressure. Any rise in airway pressure, or a dip in oxygen saturation should be seriously investigated. Tube displacement, kinking must also be ruled out, as these patients are in the prone position. It may be helpful to place a stethoscope near the ipsilateral base of the chest for frequent auscultation. There should be no hesitation to use the C arm to rule out pleural injury when suspected. It must be remembered, however, that the images on the C arm are usually inverted- (i.e.) air appears white and fluid black. A comprehensive understanding of the renal anatomy by the anaesthesiologist is also essential to prevent complications. This is because respiration needs to be coordinated when the surgeon makes the tract by sequential dilatation. The parietal pleura is reflected at to the level of the 10th rib in the mid axillary line; posteriorly it is usually reflected obliquely at the midpoint of the 12th rib. In full expiration, the visceral pleura never descends to the level of the midpoint of the 12th rib [7]. Hopper et al., [13] used CT with sagittal reconstruction at both maximum inspiration and expiration and proved that the needle path had a 29% chance on the right and a 14% chance on the left of transgressing the pleura. During forced maximum inspiration, the lung would be in the path of the needle in most patients. Hence, initial needle puncture must be made only during full expiration to avoid inadvertent pleural injury damage to the visceral pleura [14]. It must be ensured that the needle is advanced just above the upper border of the 12th rib. In order to provide full downward displacement of the kidney for easy access to the superior pole and posterior calyx, the entry into the renal parenchyma must be made during deep inspiration.
Another major concern in these procedures is the risk of septicemia in the immediate post–operative period.The risk of infection is proportional to the amount of irrigation fluid used and the duration of surgery [15]. Hence, it must be ensured that the patient is started on antibiotics pre–operatively, and continued into the post-operative period. The patient is also at a risk for hypothermia because of the use of large amounts of irrigation fluid.
Before exubation, the absence of pleural injury can be confirmed with C arm. A routine chest X-ray post operatively is mandatory. A complete blood picture must be ordered post operatively to assess blood loss and indication for transfusion.
All supra–costal punctures would traverse the diaphragm; although harmless, this can be a source of intense pain after the procedure. Adequate pain relief also contributes to a smooth recovery.
Conclusion
PCNL is a common urological procedure done under general anaesthesia in prone position. Although it has several advantages, it is also associated with some life threatening complications like pneumothorax, hydrothorax, concealed haemorrhage etc. Anaesthesiologist, as a peri-operative physician should be vigil enough to diagnose promptly and treat appropriately these complications.
[1]. Fernstrom I, Johansson B, Percutaneous pyelolithotomy. A new extraction techniqueScand J UrolNephrol 1976 10(3):257-9. [Google Scholar]
[2]. Liatsikos EN, Kapoor R, Lee B, Jabbour M, Barbalias G, Smith AD, “Angular percutaneous renal access”. Multiple tracts through a single incision for staghorncalculous treatment in a single sessionEur Urol 2005 48:832-7. [Google Scholar]
[3]. Snyder JA, Smith AD, Staghorn calculi: percutaneous extraction versus anatrophicnephrolithotomyJ Urol 1986 136:351-4. [Google Scholar]
[4]. Assimos DG, Complications of Stone Removal. In: Marshall L, Stoller MD, Smith AD, et al., edsSmith’s Textbook of Endourology 1996 Vol 1St. LouisQuality Medical Publishing:298-308. [Google Scholar]
[5]. Michel MS, Trojan L, Rassweiler JJ, Complications in percutaneous nephrolithotomyEur Urol 2007 51:899-906.discussion [Google Scholar]
[6]. Coleman CC, Kimura Y, Reddy P, Complications of nephrolithotomySeminInterv Radiol 1984 1:70-74. [Google Scholar]
[7]. Hossain M, Ullah ATMA, Regmi S, Rahman H, Kibria SAMG, Safety and efficacy of the supracostal access for percutaneous nephrolithotomy: Our initial experienceBangladesh Med Res Counc Bull 2011 37:34-38. [Google Scholar]
[8]. Shaban A, Kodera A, Elghoneimy Mohamed N, Orban TZ, Mursi K, Hegazy A, Safety and Efficacy of Supracostal Access in Percutaneous Renal SurgeryJournal of Endourology January 2008 Volume 22(Number 1) [Google Scholar]
[9]. Kekre NS, Gopalakrishnan GG, Gupta GG, Supracostal approach in percutaneous nephrolithotomy: experience with 102 casesJ Endourol 2001 15:789-791. [Google Scholar]
[10]. Golijanin D, Katz R, Verstanding A, The supracostal percutaneous nephrostomy for treatment of staghorn and complex kidney stonesJ Endourol 1998 12:403-05. [Google Scholar]
[11]. Lojanapiwat B, Prasopsuk S, Upper-pole access for percutaneous nephrolithotomy: comparison of supracostal and infracostal approachesJ Endourol 2006 20:491-94. [Google Scholar]
[12]. Gupta R, Kumar A, Kapoor R, Prospective evaluation of safety and efficacy of the supra–costal approach for percutaneous nephrolithotomyBJU Int 2002 90:809-13. [Google Scholar]
[13]. Hopper KD, Yakes WF, The posterior intercostal approach for percutaneous renal procedures. Risk of puncturing the lung, spleen, and liver as determined by CTAJR 1990 154:115-7. [Google Scholar]
[14]. Maheshwari PN, Andankar MG, Hegde S, Bansal M, The supracostal approach for percutaneous nephrolithotomyBJU Inter–national 2000 85(4):557-914. [Google Scholar]
[15]. Dogan HS, Sahin A, Cetinkaya Y, Akdogan B, Ozden E, Kendi S, Antibiotic prophylaxis in percutaneous nephrolithotomy: prospective study in 81 patientsJ Endourol 2002 16:649-53. [Google Scholar]