Left-sided Gastroschisis: A Rare Congenital Anomaly
Ankur Mandelia1, Sandeep Agarwala2, Nitin Sharma3, Shailesh Solanki4, Shashank Panda5
1 Senior Resident, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi–110029, India.
2 Additional Professor, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi–110029, India.
3 Senior Resident, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi–110029, India.
4 Senior Resident, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi–110029, India.
5 Senior Resident, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi–110029, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ankur Mandelia, Senior Resident, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi-110029, India.
Phone: 9557491171,
E-mail: drankurmandelia@gmail.com
In gastroschisis, the defect in the abdominal wall is located almost always to the right of the umbilicus. Left-sided gastroschisis is a very rare entity. A case of left sided gastroschisis has been described here, with review of literature.
Gastroschisis, Left sided
Case Report
A baby boy presented to us twelve hours after birth with eviscerated stomach and bowel loops [Table/Fig-1a]. The patient weighed 2260g and he was delivered vaginally at term to a 20-year-old healthy primigravida. Antenatal ultrasound scans at 18 and 24 weeks of gestation had revealed no foetal anomalies. On physical examination, an abdominal wall defect was identified at the left side of intact umbilical cord, which was consistent with the diagnosis of a left-sided gastroschisis. The defect was circular and approximately 3 × 3 cm in dimension. The eviscerated stomach and small and large bowel loops were thickened and oedematous. No membrane covered the eviscerated bowel loops. Rest of the systemic examination was normal. Echocardiography revealed patent ductus arteriosus with a left to right flow.
(a) Showing the patient with eviscerated bowel loops from a defect on the left of the umbilical stump. (b) Creation of a silo, (c) silo reduction over the next 5 days, (d) Position of reduced loops on removal of silo at reoperation,(e) Defect closure with a Gortex and prolene patch, (f) Skin closure over the patch.
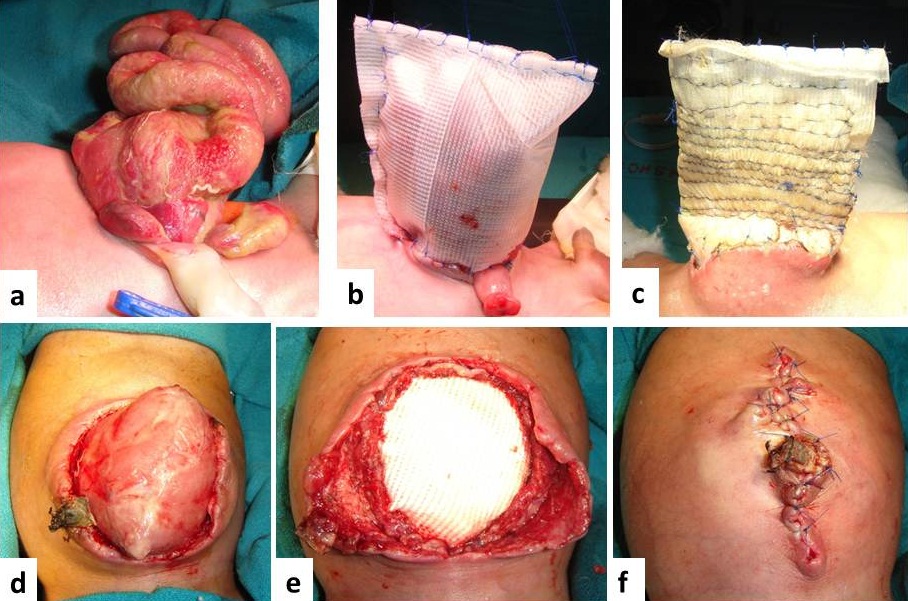
After initial resuscitation, he was taken to the operating room for repair of the defect. The findings at surgery were an abdominal wall defect to the left of umbilicus.The edges of the defect were well formed and the surrounding muscle and fascia were normal.The eviscerated stomach and small and large bowel loops were thickened and oedematous. The normal 3-vessel cord included a vein and two arteries. There was no situs inversus and the liver and falciform ligament were normally located.
The defect was extended to 2 cm in both directions vertically and abdominal wall was stretched in all four quadrants. However, the eviscerated bowel could not be reduced into the abdominal cavity. Therefore, an artificial silo was constructed with a prolene mesh, which was lined with steridrape on both surfaces and this was used to cover the herniated bowel [Table/Fig-1b]. Post–operatively, the baby was ventilated and he received parenteral nutrition. The silo was reduced progressively over 5 days [Table/Fig-1c] before an abdominal wall closure was attempted. The patient was then taken up for closure of the fascial defect, but as this was still not possible, a mesh closure which used a gortex patch with a prolene mesh was done [Table/Fig-1d,Table/Fig-1e]. The abdominal skin was mobilized and it was closed over the patch [Table/Fig-1f]. Post-operatively, the baby required ventilatory support for 7 days. He was maintained on total parenteral nutrition till the ileus subsided and oral feeds could be resumed. The baby, however, succumbed to severe pneumonia and sepsis on day 26 of his life.
Discussion
Gastroschisis is a full-thickness defect in the abdominal wall, just to the right of a normal insertion of the umbilical cord into the body wall. Left-sided gastroschisis is extremely rare, with only 20 cases being reported till date [Table/Fig-2]. Out of the twenty cases, six (30%) were males. Two cases had a defect away from the umbilicus, in the left flank and only one had situs inversus. Nine patients had major associated anomalies. In 13 cases, primary closures of the defects were possible, while in the remaining, staged closures were carried out.
Summary of reported cases of left-sided gastroschisis
| S.No. | Year | Authors | Gestational age (week) | Birth weight (gm) | Sex | Location of the defect | Associated anomalies | Method of closure |
|---|
| 1 | 1988 | Blair et al., [1] | - | - | M | Left of umbilicus | None | Primary closure |
| 2 | 1989 | Hirthler et al., [1] | 27 | 900 | F | Left of umbilicus | Hyaline membrane disease | Primary closure |
| 3 | 1989 | Hirthler et al., [1] | Term | 3800 | M | Left of umbilicus | None | Primary closure |
| 4 | 1993 | Toth et al., [1] | 35 | 1540 | F | Left of umbilicus | None | Primary closure |
| 5 | 2000 | Thepcharoennirund et al., [1] | 36 | 1700 | F | Left of umbilicus | None | Primary closure |
| 6 | 2000 | Thepcharoennirund et al., [1] | 40 | 2450 | F | Left of umbilicus | None | Primary closure |
| 7 | 2001 | Pringle KC [2] | 34 | 2065 | M | Left of Umbilicus | Left testis herniating through defect | Primary closure |
| 8 | 2002 | Fraser et al., [3] | 28 | 880 | M | Left upper quadrant | None | Primary closure |
| 9 | 2002 | Ashburn et al., [1] | 37 | 2800 | F | Left of umbilicus | None | Primary closure |
| 10 | 2004 | Ameh et al., [4] | Term | - | M | Left flank | None | Staged closure |
| 11 | 2004 | Orpen et al., [1] | Term | 2,750 | F | Left of umbilicus | Pseudoexstrophy, ASD, PDA, ureteral reflux | Primary closure |
| 12 | 2004 | Wang et al., [1] | - | - | - | Left of umbilicus | Situsinversus | Staged closure |
| 13 | 2004 | Yoshioka et al., [1] | 38 | 2,604 | F | Left of umbilicus | None | Staged closure |
| 14 | 2004 | Yoshioka et al., [1] | 34 | 1700 | F | Left of umbilicus | Necrosis of the herniated bowel | Primary closure |
| 15 | 2006 | Gow et al., [1] | 39 | 2,815 | F | Left of umbilicus | None | Primary closure |
| 16 | 2007 | Prasun et al., [1] | 24 (terminated) | - | M | 1.5 cm left and lateral to umbilicus | Multicystic renal dysplasia | - |
| 17 | 2008 | Suver et al., [1] | 34 | 3100 | F | Left of umbilicus | Jejunal atresia, microcolon, Absent corpus callosum, optic dysplasia, panhypopituitarism, intestinal atresia | Staged closure |
| 18 | 2008 | Suver et al., [1] | 35 | 2,200 | F | Left of umbilicus | Cerebral arterio-venous malformations | Staged closure |
| 19 | 2008 | Suver et al., [1] | 34 | 2200 | F | Left of umbilicus | Atrial septal defect, pulmonary valve stenosis | Staged closure |
| 20 | 2010 | Patel et al., [5] | 34 | 2160 | F | Left of umbilicus | Small left colon syndrome | Primary closure |
A favoured theory of pathogenesis of gastroschisis is an abnormality in the timing of involution of the right umbilical vein, which normally occurs during the sixth gestational week in the human embryo. At this stage, the developing para-umbilical abdominal wall undergoes a transition in nutrient support and vascular drainage, from umbilical vein to nutrient aortic vessels and caval veins. According to de Vries, it is during this transition to a secondary circulation, that either a premature or a delayed atrophy of the right umbilical vein can lead to a localized ischaemic mesenchymal damage [6]. This theory, perhaps, best explains as to why the defect in gastroschisis occurs to the right of the umbilicus. Other theories have suggested that gastroschisis was the result of an interruption of the omphalo-mesenteric artery, or that it evolved from rupture of the amniotic membrane, at the base of an umbilical cord mass [7].
The aetiology for left-sided gastroschisis is unknown, and the theories which have been proposed previously had been unable to account for the majority of defects which occur on the right. The early regression of the left umbilical vein may explain the pathogenesis of left-sided gastroschisis. An alternative hypothesis is one that reconciles a disorder of right-left axis orientation as the primary abnormality in morphogenesis [6,7].
Feldkamp et al., [7] have recently proposed a theory that gastroschisis resulted from failure of one or more folds which were responsible for wall closure and that a right-sided defect predominated because the yolk stalk was positioned on the right, as the connecting stalk and yolk stalk merged. They proposed that slight malpositioning of the yolk stalk to the left of midline in the setting of wall fold failure could lead to left-sided defects. This theory was appealing, because it explained both right- and left-sided gastroschisis. Torfs et al., [8] reported that polymorphisms of several genes which represented enzymes which involved inangiogenesis, blood vessel integrity, inflammation, wound repair, and dermal or epidermal strength, alongwith maternal smoking, were associated with the developmentof gastroschisis. This work supported the concept of a multifactorial aetiology of gastroschisis which involves both genetic issues and environmental factors. These factors may be better understood when more becomes known about role of genes and influence of hormones in the causation of the defect. Identifying and reporting these unusual cases is essential to further expand our understanding of these conditions and their potential associations.
[1]. Suver D, Lee SL, Shekherdimian S, Left-sided gastroschisis: higher incidence of extra-intestinal congenital anomaliesAm J Surg 2008 195:663-66. [Google Scholar]
[2]. Pringle KC, Testicular proximity can induce gubernaculum formation after deliveryJ Pediatr Surg 2001 36:1708-09. [Google Scholar]
[3]. Fraser N, Crabbe DC, An unusual left-sided abdominal-wall defectPediatr Surg Int 2002 18:66-67. [Google Scholar]
[4]. Ameh EA, Mshelbwala PM, Sabiu L, A rare left-sided abdominal wall defectEur J Pediatr Surg 2004 14:427-28. [Google Scholar]
[5]. Patel R, Eradi B, Ninan G, Mirror-image left-sided gastroschisisAust N Z J Surg 2010 80:472-73. [Google Scholar]
[6]. De Vries P, The pathogenesis of gastroschisis and omphaloceleJ Pediatr Surg 1980 15:245-46. [Google Scholar]
[7]. Feldkamp ML, Carey JC, Sadler TW, Development of gastroschisis: review of hypotheses, a novel hypothesis, and implications for researchAm J Med Genet 2007 143:639-52. [Google Scholar]
[8]. Torfs CP, Christianson RE, Lovannisci DM, Selected gene polymorphisms and their interaction with maternal smoking, as risk factors for gastroschisisBirth Defects Research A Clin Mol Teratol 2006 76:723-30. [Google Scholar]