Phytobezoar: A Rare Cause of Small Bowel Obstruction
Anupama Pujar K.1, Sreekar Pai A.2, Bharati Hiremath V.3
1 Assistant Professor, Department of Surgery, M.S. Ramaiah Medical College, Bangalore, India.
2 Associate Professor, Department of Surgery, M.S. Ramaiah Medical College, Bangalore, India.
3 Professor, Department of Surgery, M.S. Ramaiah Medical College, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anupama Pujar K., No 1165, 5th main, 4th block, HBr Layout, Bangalore-560043, India.
Phone: 97419687,
E-mail: anupamapujar@rediffmail.com
Phytobezoar is an unusual cause of small bowel obstruction. It accounts for about 0.4%-4% of all mechanical bowel obstruction. However, the symptoms are not very different from those caused by usual aetiologies of small bowel obstruction. The commonest site of obstruction is terminal ileum. Treatment of small bowel obstruction due to Phytobezoar is surgery. Prevention includes avoidance of high fibre diet, prokinetics particularly in patients who have undergone gastric surgery. A 57-year-old male presented with symptoms and signs of small bowel obstruction. On exploratory laparotomy Phytobezoar in the ileum was found to be the cause of obstruction. Diagnosis was confirmed by histopathology.
Intestinal obstruction, Bezoar, Phytobezoar
Case Report
A 57-year-old male patient brought to casualty with pain and distension of abdomen since one day. The pain was diffuse all over abdomen, colicky in nature, which was associated with 5-7 episodes of vomiting. He also had not passed stools for one day. The past history of patient revealed that he had undergone laparotomy, details of which were not known to the patient. There were no known comorbidities. At the time of admission vitals were stable except high blood pressure. Abdomen was distended with tenderness all over the abdomen. No guarding or rigidity was present. Bowel sounds were sluggish. Taking all this into consideration, clinical diagnosis of sub-acute intestinal obstruction due to post-op adhesions was considered.
There were dilated small bowel loops on Supine X-ray abdomen. Ultrasound abdomen revealed dilated bowel loops with to and fro movements that were suggestive of intestinal obstruction with mild free fluid in abdomen. Blood investigations and Chest X-ray were normal. The patient was managed conservatively. However, the patient did not respond to conservative management. Ryles tube aspiration was feculent on following day. Repeat X-ray showed persisting features of small bowel obstruction. The patient was subjected to exploratory laparotomy and the findings were that of dilated oedematous small bowel loops [Table/Fig-1] extending 30cm from ileocaecal junction to mid-jejunum. There was intraluminal mass felt distal to dilated loops causing obstruction. Enterotomy was done and large faecolith [Table/Fig-2] was extracted and sent for histpathology. Enterotomy closed in two layers. The patient recovered well post-operatively. The histopathology of faecolith revealed vegetable matter [Table/Fig-3]. Patient was started on liquids orally on 5th day followed by soft diet subsequently. The patient was discharged on 10th post operative day. Patient was on follow up for one month which was found uneventful.
Dilated small bowel loops withintraluminal mass being felt

Phytobezoar after being removed through enterotomy

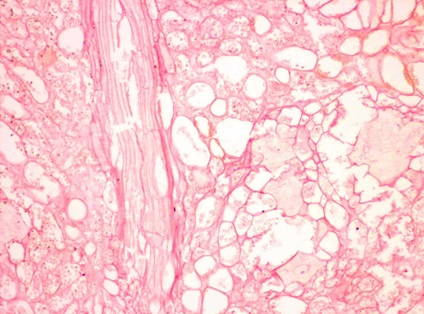
Histopathology of faecolith showing vegetable matter
Discussion
Small bowel obstruction is a common disease encountered in surgical practice. Literature shows diverse and varied aetiologies for intestinal obstruction. However, phytobezoar is rarely reported etiological factor, accounting for only 0.4%-4% of all mechanical small bowel obstruction [1]. Phytobezoars are concretions of poorly digested fruit and vegetable fibres that are found in alimentary track and are mostly composed of indigestible cellulose, tannin and lignin from ingested vegetables and fruits [2]. The commonest Phytobezoar encountered worldwide is related to the ingestion of persimmon fruit [3]. Normally, they are found in stomach and they may enter into the small bowel. The primary small bowel bezoars are very rare, and they are usually seen in patients with underlying small bowel diseases such as stricture, diverticulum or tumor [1]. There are several predisposing factors that influence Phytobezoar formation. Some of the common ones are previous gastric surgery,excessive consumption of fruits rich in fibres,poor dental health, insufficient mastication, diabetic gastro paresis, kidney failure,hypothyroidism and use of drugs which affect gastric motility [4]. The patient had undergone laparotomy 6 years back and the details of which are not known. The patient is in traffic police and mostly always eats outside food in hurry without chewing adequately. There is a slight male preponderance reported.
Primary small bowel bezoars are very rare and invariably causes obstruction of small bowel [5]. Clinical presentation of Phytobezoar induced small bowel obstruction is same as due to other causes, such as pain abdomen, distension of abdomen, nausea, vomiting and constipation [6]. Hence, it is difficult to differentiate between small bowel obstruction due to Phytobezoar and adhesions, particularly in patients who have history of previous abdominal surgery. Our working diagnosis was sub-acute intestinal obstruction due to post operative adhesions.
Plain supine X-Ray typically shows a classic obstructive pattern of small bowel. Occasionally outline of bezoar can be made out, which is difficult to differentiate from abscess or faeces within the colon [1]. The diagnostic rate of abdominal ultrasound in detecting Phytobezoar is reported to be 88%-93% [6]. But it is operator dependent and bezoar can be concealed by bowel gas. In this patient both X-ray abdomen and ultrasound showed features suggestive of small bowel obstruction. The cause of obstruction can be diagnosed by computed tomography in 73%-95% [7] of patients, and its diagnostic accuracy for bezoar induced small bowel obstruction is about 65%-100% [6]. It is operator independent investigation that confirms the level of obstruction, existence of multiple bezoars,as well as any complications such as bowel ischemia and perforation. Well defined intraluminal mass with mottled gas appearance associated with encapsulating wall is suggestive of Phytobezoar [8]. In our patient we didn’t do CT abdomen and took him for exploratory laparotomy as he developed signs of acute intestinal obstruction.
The treatment of choice for small bowel obstruction due to Phytobezoar is surgery. Most bezoars in the small bowel are found 50cm-70cm proximal from ileocaecal valve, because it is narrow, slow intestinal motility and a large amount of water absorption hardens the bezoar resulting in losing its motility [6]. Surgical options reported are manual fragmentation of Phytobezoar and pushing it towards caecum. If it is not possible enterotomy should be done to remove the bezoar. Segmental bowel resection and anastomosis may be required in presence of complications such as gangrene of bowel [9]. At the time of laparotomy thorough exploration of abdominal cavity should be done to exclude the presence of concomitant gastric bezoar or intestine bezoars [4]. About one third of patients have multiple intestinal bezoars. Laparoscopic management of Phytobezoar induced small bowel obstruction have been reported, however this requires expertise [10].
The best way to manage Phytobezoar is prevention. Good eating habits,avoiding high fibre diet particularly in patients with gastric surgery,introduction of prophylactic medications to improve gastric motility and psychiatric follow up in patients with psychiatric disease [1]. Our patient was counselled by dietician and was on prokinetics at the time of discharge.
Conclusion
Phytobezoar induced small bowel obstruction is a very rare entity and often overlooked. There should be high index of suspicion in patients with small bowel obstruction who have previous history of gastric surgery. The presence of intra-luminal mass with mottled gas pattern at the site of obstruction in CT abdomen is diagnostic of Phytobezoar. Surgery is the treatment of choice in phytobezoar induced small bowel obstruction. Diet modification is the best way of prevention.
[1]. Teng HC, Nawawi O, Ng KL, Phytobezoar:an unusual cause of intestinal obstructionBiomedical Imaging and Interventional Journal 2005 1(1) [Google Scholar]
[2]. Ladas SD, Kamberoglou D, Karamanolis G, Systematic review: Coca-Cola can effectively dissolve gastric phytobezoars as a first-line treatmentAliment Pharmacol Ther 2013 37:169-73. [Google Scholar]
[3]. Chisholm EM, Chung SCS, Leong HT, Phytobezoar: a uncommon cause of small bowel obstructionAnnals of Royal College of Surgeons of England 1992 74:342-44. [Google Scholar]
[4]. Salemis NS, Panagiotopoulos N, Sdoukos N, Niakas E, Acute Surgical Abdomen Due to Phytobezoar-indusedileal obstructionThe Journal of Emergency Medicine 2013 44(1):e21-e23. [Google Scholar]
[5]. Ezzat RF, Rashid SA, Rashid AT, Abdullah KM, Ahmed SM, Small intestinal obstruction due to phytobezoar:a case reportJournal of Medical Case Reports 2009 3:9312 [Google Scholar]
[6]. Oh HS, Namgung H, Park M, Park DG, Bezoar-induced small bowel obstructionJournal of the Korean Society of Coloproctology 2012 28(2):89-93. [Google Scholar]
[7]. Ho TW, Koh DC, Small bowel obstruction secondary to bezoar impaction: a diagnostic dilemmaWorld J Surg 2007 31:1072-78. [Google Scholar]
[8]. Delabrousse E, Lubrano J, Small bowel bezoar versus small bowel feces: C T evaluationAmerican Journal of Roentgenology 2008 Nov 191(5):1465-68. [Google Scholar]
[9]. Bedioui H, Daghfous A, Ayadi M, Noomen R, A report of 15 cases of small bowel obstruction secondary to phytobezoars: predisposing factors and diagnostic difficultiesGastroenterologie Clinique et biologique 2008 32(6-7):596-600. [Google Scholar]
[10]. Ettinger JEMT, Silva Reis JM, laparoscopic Management of intestinal obstruction due to phytobezoarJournal of Society of Laparoendoscopic Surgeons 2007 Jan-march 11(1):168-71. [Google Scholar]