Painful Late Recurrence of Dermatofibrosarcoma Protuberans of Breast in a Centurian Female
Asitava Deb Roy1, Kumar Nishant2, Deepti Joshi3
1 Assistant Professor, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Tadong, East Sikkim 737102, India.
2 Assistant Professor, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Tadong, East Sikkim 737102, India.
3 Associate Professor, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Tadong, East Sikkim 737102, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Asitava Deb Roy, Assistant Professor, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Tadong, East Sikkim 737102, India.
Phone: 9475587658,
E-mail: asitavadr@gmail.com
Dermatofibrosarcoma protuberans (DFSP) of the breast is rare. Late and painful local recurrence of this entity on this site is even more uncommon. We describe such a case in a 102-year-old woman, who at the age of 77 years had been operated for a breast lump for which only a cytopathological diagnosis of fibrohistiocytic tumour was available. Twenty years later, she noticed a small mass in her right breast over the postsurgical scar area, which gradually increased in size over the last five years. She presented to the surgical out-patient clinic with pain and redness over the swelling. Wide local excision of the tumor with generous tissue margin was performed under intercostal block on account of her age and suboptimal cardiac status. The microscopic and immunohistochemical findings established the diagnosis of recurrent DFSP. We report an exceptionally rare case of local recurrence of DFSP in the female breast and discuss in detail the diagnostic and therapeutic implications of this pathology.
Dermatofibrosarcoma, Painful, Recurrence, Breast
Introduction
Dermatofibrosarcoma protuberans (DFSP) was first described by Darier and Ferrand in 1924 [1]. It is a rare, locally aggressive, but rarely metastasizing tumour of the deep dermis and subcutaneous tissue, with a propensity to recur. It may occur at almost any site, but is more common in the trunk and extremities [2]. DFSP of the breast has been rarely reported. We are presenting a case of recurrent dermatofibrosarcoma protuberans of breast which occurred in a centurian female.
Case Report
A 102–year–old female presented with swelling and pain in her right breast. She had been operated 25 years ago for a lump on the right breast, with a pre-operative cytopathological diagnosis of fibrohistiocytic tumour. No other documents related to surgery or histopathological diagnosis were available. Five years ago, she had noticed a small lump at the site of previous surgical scar, which had kept on increasing in size gradually and since past one month, she started developing pain and redness over the swelling. Physical examination showed a firm, well-defined, tender, mobile, erythematous (8 x 6 cm) mass on the upper outer part of the right breast. A transverse radial healed scar was evident over the centre of the swelling. No lymph nodes in the axilla or supraclavicular fossa were palpable.
Patient opted for surgical excision of her lump. Her pre-operative assessment was unremarkable, except for aortic valve calcification. A wide excision of the lump was done under intercostal block, with monitored operative care. Pre-operatively, the lump was not adherent to the underlying muscles.
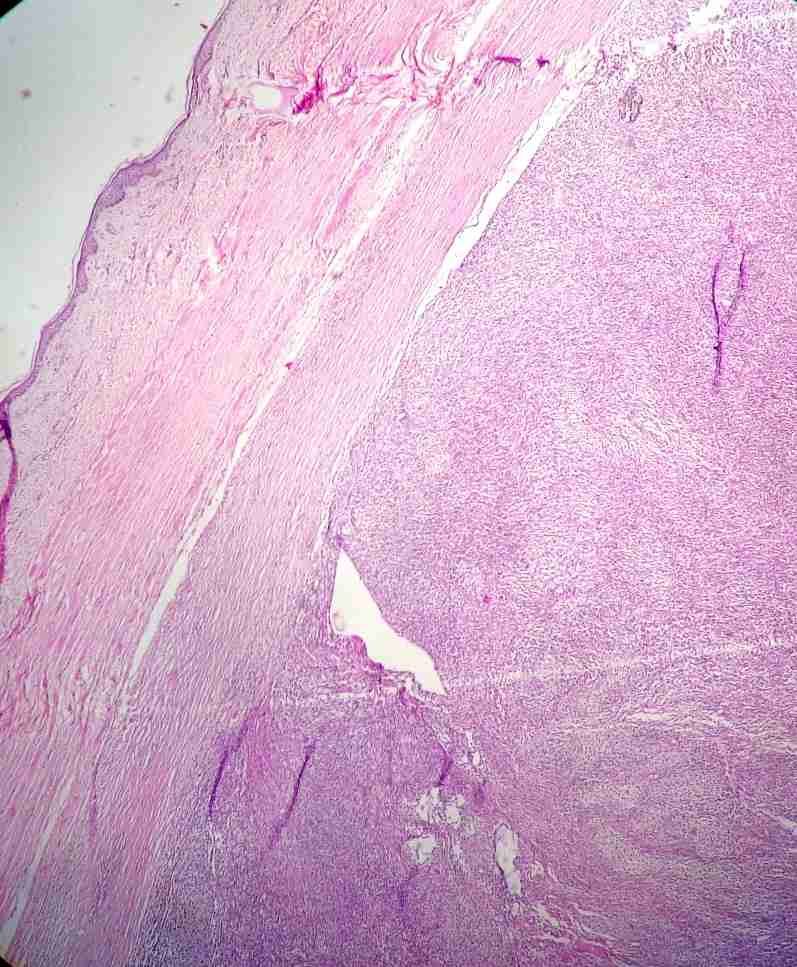
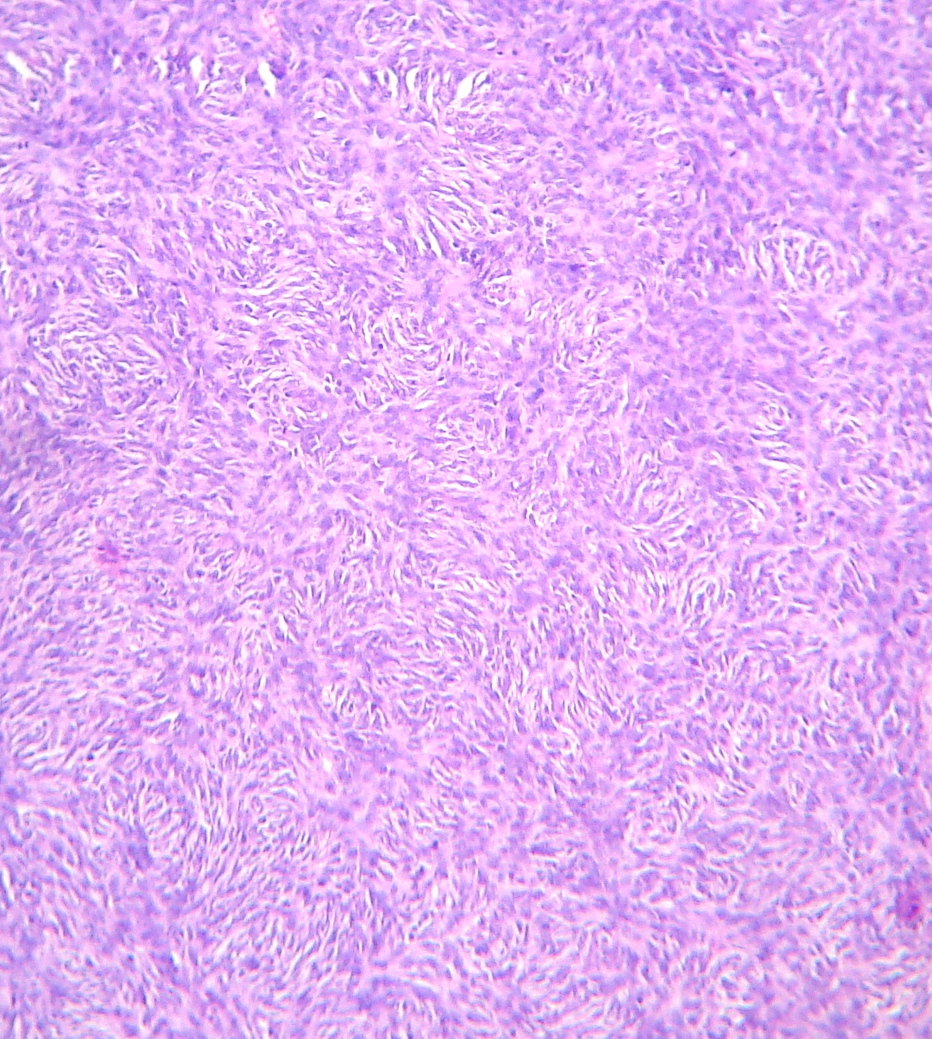
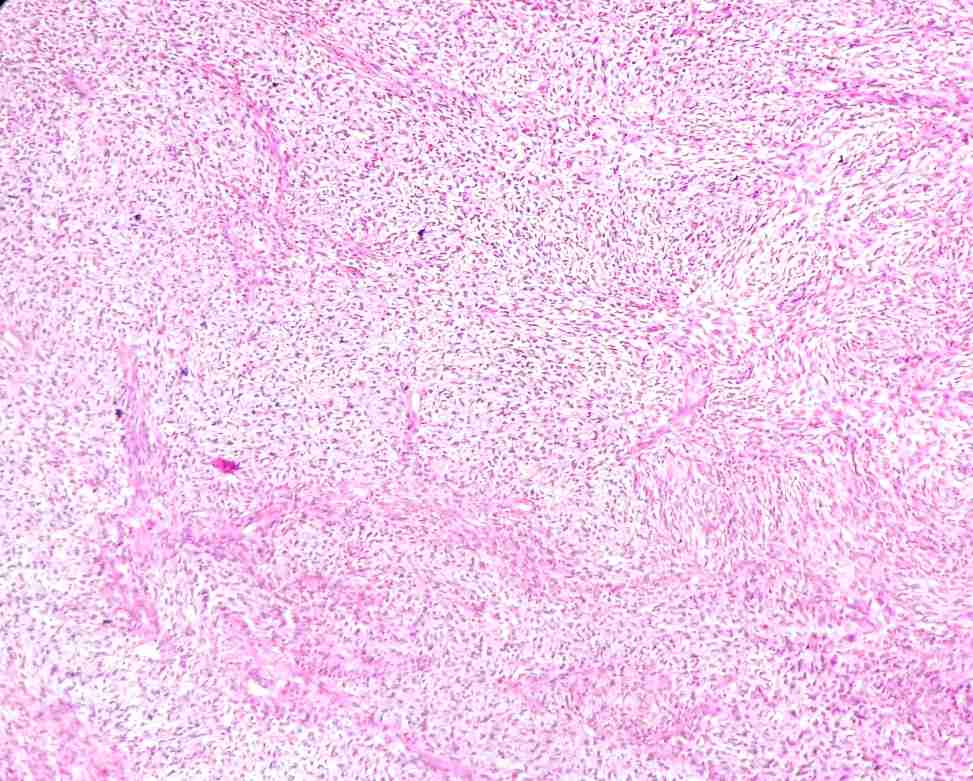
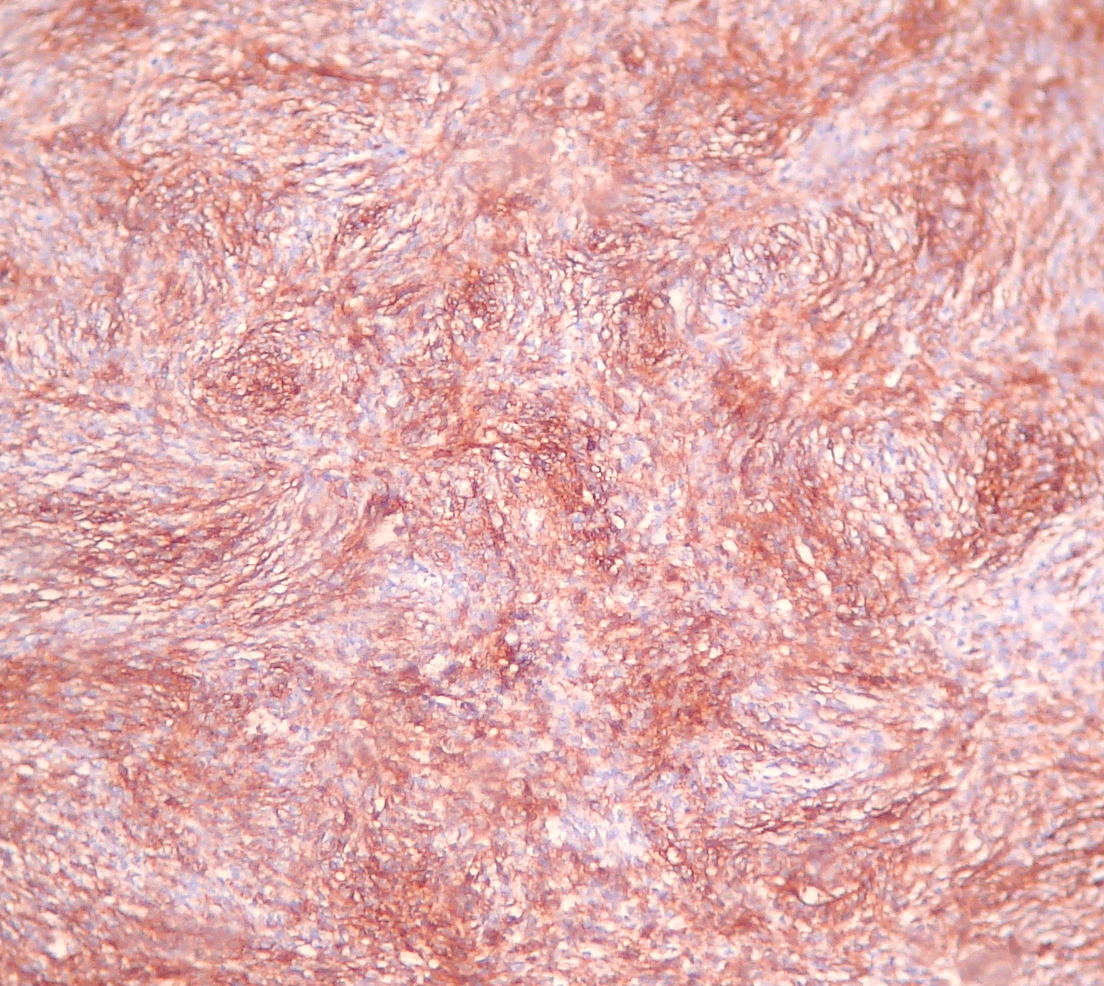
Microscopy showed a dermal proliferation of spindle cells [Table/Fig-1] arranged in storiform pattern [Table/Fig-2], with extension into adipose tissue lobule. The tumour was highly cellular, but had relatively few mitoses (5-6 per 10 high power fields). Areas of necrosis and myxoid degeneration [Table/Fig-3] with presence of stellate cells were noted. The neoplastic spindle cells showed intense positivity for vimentin and CD34 [Table/Fig-4]. The final histological diagnosis was dermatofibrosarcoma protuberans (DFSP) of breast.
Dermal proliferation of spindle cells (40X, H and E)
Storiform pattern of DFSP (100x, H and E)
Areas of myxoid degeneration (100x, H and E)
Neoplastic cells showing CD 34 positivity (100x)
Discussion
Breast is an unusual location for DFSP to occur. The present case showed few other unusual features. Firstly, it was a case of painful local recurrence and secondly, it presented as a case of late recurrence in a centurian female who had been operated for a similar lesion 25 years back. Previously described lesions had been mostly asymptomatic and they had been seen in younger women [2,3,4]. Our literature search revealed only two cases with a late recurrence (> 20 years) of DFSP in breast and that too, in younger women, in their 40s and 50s. In a review done on 115 cases of DFSP, Taylor and Helwig [5] cited a single recurrence after 20 years, while Swan et al observed a late recurrence of DFSP in the breast after 26 years [6]. Thirdly, presence of myxoid areas in the present tumour was also a significant finding, because these areas are believed to be a feature of recurrent lesions [5].
The diagnosis of DFSP mainly depends on histopathology and immunohistochemistry. Histopathology of DFSP is very typical, with its characteristic storiform pattern of dermal proliferation and subcutaneous tissue infiltration. However, immunohistochemistry for CD34 is required to confirm the diagnosis. CD34 positivity in the neoplastic cells of DFSP proves that it is closely linked to the normal CD34 positive dendritic cells [2].
The histopathological differential diagnoses of other spindle cell lesions in the breast include fibromatosis-like metaplastic carcinoma, fibromatosis, inflammatory myofibroblastic tumour, phyllodes tumour and periductal stromal hyperplasia [7]. Negative staining of the tumour for epithelial membrane antigen (EMA) excluded the possibility of a fibromatosis-like metaplastic carcinoma. The typical storiform pattern and CD34 immunoreactivity were also against the diagnosis of a fibromatosis. The diagnosis of inflammatory myofibroblastic tumour was excluded, because of lack of a conspicuous inflammatory infiltrate and negative smooth muscle markers in the present tumour. Both phyllodes tumour and periductal stromal hyperplasia/tumour show a biphasic pattern composed of spindle cells around tubular or ductal structures, that was not present in the present tumour.
The standard treatment of DFSP is wide excision [8]. A wider margin of excision ensures lesser chances of recurrence. Arnaud et al. suggested that the surgical margin should not be less than 3.5-5 cm for a minimal recurrence rate [9]. Some authors suggest the use of Moh’s micrographic surgery for cosmetic reasons 8. Adjuvant radiation therapy has been recommended after a planned marginal excision in critical anatomic sites or as the sole treatment in advanced cases where surgery is no longer feasible [8].
Conclusion
DFSP of the breast is an uncommon condition diagnosed by histopathology and immunohistochemistry. Late recurrences of the tumour do occur, but have been reported only in women of younger age groups. Painful late recurrence of the tumour in a centurian female is unusual. Better awareness of this entity can lead to a prompt diagnosis and proper management of the disease. The peculiarity of this case lies in the infrequency of its anatomic location and its unusual clinical presentation.
[1]. Darier J, Ferrand M, Dermatofibromes progressifs et recidivants ou fibrosarcoma de la peauAnn Dermatol Venereol 1924 5:545-62. [Google Scholar]
[2]. Weiss SW, Goldblum JR, Fibrohistiocytic tumours of intermediate malignancyIn: Enzinger and Weiss’s soft tissue tumors 2008 5th editionSt. LouisMosby, Inc.:371-381.Weiss SW, Goldblum JR (Eds) [Google Scholar]
[3]. Dragoumis DM, Katsohi LK, Amplianitis IK, Tsiftsoglou AP, Late local recurrence of dermatofibrosarcoma protuberans in the skin of female breastWorld Journal of Surgical Oncology 2010 8:48 [Google Scholar]
[4]. Jong-Yueh Lin, Shyr-Ming Sheen-Chen, Wayne Hsu, Chao-Cheng Huang, Sheung-Fat Ko, Hock-Liew Eng, Dermatofibrosarcoma protuberans of the breastTumori 2008 94:861-63. [Google Scholar]
[5]. Taylor RW, Helwig EB, Dermatofibrosarcoma protuberans: a study of 115 casesCancer 1962 15:717-25. [Google Scholar]
[6]. Swan MC, Banwell PE, Hollowood K, Goodacre TE, Late recurrence of dermatofibrosarcoma protuberans in the female breast: a case reportBr J Plast Surg 2005 58:84-87. [Google Scholar]
[7]. Tse GM, Tan PH, Lui PC, Putti TC, Spindle cell lesions of the breast: the pathologic differential diagnosisBreast Cancer Res Treat 2008 109:199-207. [Google Scholar]
[8]. DuBay D, Cimmino V, Lowe L, Johnson TM, Sondak VK, Low recurrence rate after surgery for dermatofibrosarcoma protuberans: a multidisciplinary approach from a single institutionCancer 2004 100:1008-16. [Google Scholar]
[9]. Arnaud EJ, Perrault M, Revol M, Servant JM, Banzet P, Surgical treatment of dermatofibrosarcoma protuberansPlast Reconstr Surg 1997 100:884-95. [Google Scholar]