Fonsecaea Pedrosoi: A Rare Etiology in Fungal Keratitis
Jyoti Sangwan1, Sumit Lathwal2, Deepak Juyal3, Neelam Sharma4
1 Assistant Professor, Department of Microbiology & Immunology, Veer Chandra Singh Garhwali Govt. Medical Sciences & Research Institute, Srinagar Garhwal-246174, Uttarakhand, India.
2 Deputy Assistant Director Health, Indian Armed Forces.
3 Senior Demonstrator, Department of Microbiology & Immunology, Veer Chandra Singh Garhwali Govt. Medical Sciences & Research Institute, Srinagar Garhwal-246174, Uttarakhand, India.
4 Professor and Head, Department of Microbiology & Immunology, Veer Chandra Singh Garhwali Govt. Medical Sciences & Research Institute, Srinagar Garhwal-246174, Uttarakhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Jyoti Sangwan, Assistant professor, Department of Microbiology & Immunology, Veer Chandra Singh Garhwali Govt. Medical Sciences & Research Institute, Srinagar Garhwal-246174, Uttarakhand, India.
Phone: +919627759902,
E-mail: jyolathwal@yahoo.co.in
Fungal corneal ulcer is common in India due to tropical climate and a large agrarian population that is at risk. Fonsecaea pedrosoi is the most common agent of chromoblastomycosis, a chronic localized fungal infection of the skin and subcutaneous tissues mainly involving lower extremities. We report a rare case of corneal chromoblastomycosis caused by F.pedrosoi, which was successfully treated with topical Amphotericin B followed by a long course of oral antifungal therapy. To the best of our knowledge, this is the first case of mycotic keratitis caused by F.pedrosoi, from the foothills of Himalayas.
Amphotericin B, Corneal ulcer, Fonsecaea pedrosoi, Ketoconazole
Introduction
Mycotic keratitis is a fungal infection of cornea primarily affecting the corneal epithelium and stroma with involvement of endothelium and anterior chamber of eye in severe cases [1]. It is an important ophthalmological problem, particularly in agricultural communities, and more than 50 genera of fungi have been implicated in its etiology [2]; most of these are saprobic organisms that cause opportunistic corneal infections in traumatized or immunologically compromised eyes. The genera of fungi most frequently implicated as causes of mycotic keratitis worldwide include Aspergillus, Candida, Curvularia, Fusarium and Penicillium. In addition, certain other species of fungi may rarely cause keratitis. New infectious agents are continually appearing, around 20 species yearly. It is possible that many of the recently reported taxa have caused infections which previously passed unnoticed due to inadequate diagnostic expertise [3]. This paper describes a case of keratitis due to Fonsecaea pedrosoi, a primary cause of cutaneous chromoblastomycosis, but a rarely reported etiology in fungal keratitis. To the best of our knowledge this is a first such case to be reported from foothills of Himalayas.
Case Report
A 35-year-old agriculture worker presented with the complains of pain, redness, irritation, watering, and photophobia in the right eye (RE) of 20 days duration, following injury by a sugarcane leaf. On slit lamp examination, the patient was found to have a dirty white corneal ulcer (5× 6 mm) with feathery margins, stromal infiltration and hypopyon (1mm) in the RE [Table/Fig-1]. There were no satellite lesions; the visual acuity in this eye was “perception of light” (PL) only. The visual acuity in the patient’s left eye was 6/18 with no other detected abnormality.
Corneal ulcer in the right eye of the patient

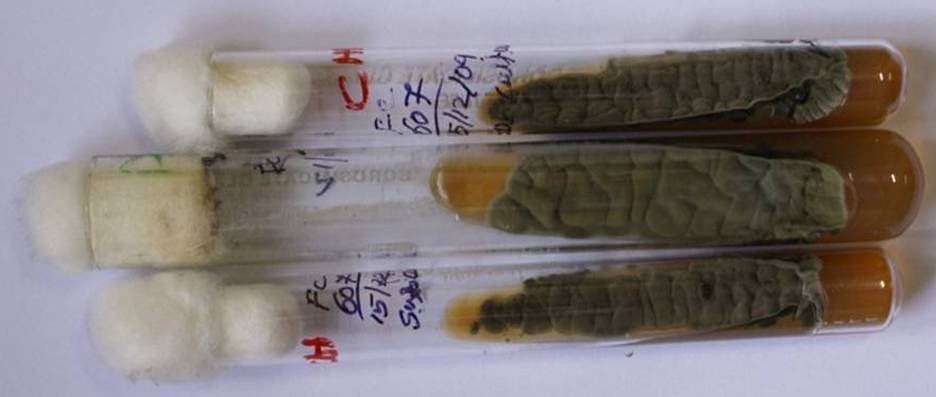
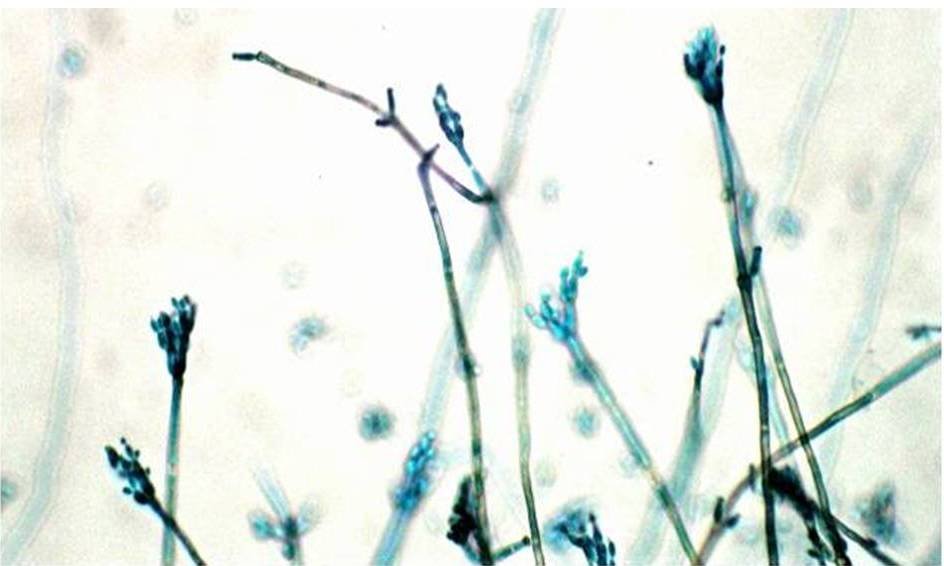
Under local anaesthesia (4% lignocaine), multiple scrapings were obtained from the base and edges of the corneal ulcer with a sterile blunt cataract knife. A potassium hydroxide (KOH) wet mount and Gram-stained smear of the scrapings were prepared for direct microscopic examination. Scrapings were also inoculated on Sabouraud Dextrose agar (SDA) and blood agar, which were incubated at 28°C and 37°C respectively. Direct microscopic examination of the KOH wet mount revealed septate fungal hyphae in the scraped material morphologically suggestive of pheoid fungus [Table/Fig-2a and 2b]. After seven days of incubation, SDA showed heaped, brittle colonies dark green to black in colour with short aerial mycelia. Blood agar plate did not show any growth. Subcultures made on SDA [Table/Fig-3] and potato dextrose agar (PDA) again showed fungal colonies which were flat to heaped, folded, olivaceous to black obverse and black reverse. A cellophane tape lactophenol cotton blue (LPCB) mount prepared from the cultures (primary and subculture tubes) revealed that the mycelium was composed of branching septate pigmented hyphae with short chains of elliptical conidia formed at the ends of conidiophores (Cladosporium like conidiation) [Table/Fig-4]. Isolate was identified as F. pedrosoi. The patient was put on topical natamycin (5%) hourly and cyclopentolate (1%) drops three times a day. Although in vitro susceptibility testing does not reliably predict in vivo efficacy for fungi, and minimum inhibitory concentration (MIC) cannot be used as strict guidelines for therapy, the possibility of performing in vitro tests was considered. In this way, one may avoid ineffective, costly and prolonged course of treatment. Antifungal susceptibility testing was performed according to the guidelines of National Committee for clinical laboratory Standards (NCCLS) for moulds, using RPMI- 1640 medium buffered to pH 7.0 with 0.165 M morpholinepropanesulfonic acid (MOPS) agar plates, which revealed MIC of 0.087 μg/mL for amphotericin B, 8 μg/mL for flucytosine, 0.023 μg/mL for itraconazole, 0.03 μg/mL for ketoconazole and 0.064 μg/mL for voriconazole. Natamycin therapy was discontinued and treatment with topical amphotericin B (0.5%) was initiated every hour along with oral ketoconazole. After 12 weeks, the treatment was discontinued because clinical healing occurred. The hypopyon disappeared, the epithelial defect healed, and the stromal infiltration was yet almost completely resolved; the visual acuity of the eye improved from PL to 1/60. No relapse of infection was observed and the patient was doing fine till three months of follow up.
Pottasium hydroxide (KOH) mount preparation showing hyphal segments of a phaeoid fungus

Colony morphology on Sabouraud dextrose agar (SDA)
Lactophenol cotton blue (LPCB) mount picture showing Fonsecaea pedrosoi (Cladosporium type)
Discussion
Mycotic keratitis is an important ophthalmologic problem, particularly in rural workers. An increase in ocular infections produced by pathogenic or saprobic fungi has been documented [4,5]. Many different fungal species have been reported as causative agents of keratitis, which is not surprising since they, as saprophytic inhabitants of soil, plants and trees, can be traumatically implanted into the cornea.
In our patient, history of ocular trauma with vegetable matter (sugarcane leaf) suggested the possibility of fungal infection. Dwelling in an environment with dust pollution has been reported as a risk factor for mycotic keratitis [6,7]. Mycotic keratitis is often associated with considerable morbidity and in severe cases can even lead to endophthalmitis. Prompt and proper treatment are the best predictors of positive patient outcome. In the present case, after 12 weeks of intensive medical therapy, the corneal lesion resolved and the visual acuity of the eye improved from PL to 1/60.
Fonsecaea pedrosoi is the commonest causative agent of cutaneous chromoblastomycosis [8]. Treatment of the mycosis caused by this dematiaceous fungus is unrewarding not only because of the scarcity of effective antifungals but also due to the need for prolonged therapy, which has been reported to be as long as two years to achieve a mycological cure [9]. In the ophthalmic literature, very few cases of corneal chromoblastomycosis caused by F.pedrosoi are reported [10,11,12].
Due to diversity in the causative agents of mycotic keratitis and various dematiaceous fungi involved in such infections, F.pedrosoi although rare should be considered as one of the important etiological agents. Prompt diagnosis and intensive treatment can prevent the considerable morbidity associated with the disease.
[1]. Tuli SS, Fungal keratitisClin Ophthalmol 2011 5:275-9. [Google Scholar]
[2]. Thomas PA, Current perspectives on ophthalmic mycosesClin Microbiol Rev 2003 16:730-97. [Google Scholar]
[3]. Guarro J, Gené J, Stchigel AM, Developments in fungal taxonomyClin Microbiol Rev 1999 12:454-500. [Google Scholar]
[4]. Kaliamurthy J, Kalavathy CM, Ramalingam MD, Prasanth DA, Jesudasan CA, Thomas PA, Keratitis due to a coelomycetous fungus: case reports and review of the literatureCornea 2004 23:3-12. [Google Scholar]
[5]. Kaliamurthy J, Jesudasan CA, Prasanth DA, Thomas PA, Keratitis due to Cylindrocarpon lichenicolaJ Postgrad Med 2006 52:155-57. [Google Scholar]
[6]. Leck AK, Thomas PA, Hagan M, Kaliamurthy J, Ackuaku E, John M, Aetiology of suppurative corneal ulcers in Ghana and south India, and epidemiology of fungal keratitisBr J Ophthalmol 2002 86:1211-215. [Google Scholar]
[7]. Thomas PA, Geraldine P, Infectious keratitisCurr Opin Infect Dis 2007 20:129-41. [Google Scholar]
[8]. Kim DM, Hwang SM, Suh MK, Ha GY, Choi GS, Shin J, Han SH, Chromoblastomycosis Caused by Fonsecaea pedrosoiAnn Dermatol 2011 Aug 23(3):369-74. [Google Scholar]
[9]. Esterre P, Andriantsimahavandy A, Ramarcel ER, Pecarrere JL, Forty years of chromoblastomycosis in Madagascar: a reviewAm J Trop Med Hyg 1996 55:45-47. [Google Scholar]
[10]. Barton K, Miller D, Pflugfelder SC, Corneal chromoblastomycosisCornea 1997 16:235-39. [Google Scholar]
[11]. Kim YS, Song YS, Kim JC, Fungal keratitis caused by ChromomycetesJ Korean Ophthalmol Soc 2003 44:755-59. [Google Scholar]
[12]. Höfling-Lima AL, Guarro J, Freitas Dd, Godoy P, Gené J, Souza LB, Clinical treatment of corneal infection due to Fonsecaea pedrosoi—case reportArq Bras Oftalmol 2005 68:270-72. [Google Scholar]